You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Landmark Papers in AnaesthesiaDocument513 pagesLandmark Papers in AnaesthesiaLau Hon WaiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Physical Assessment Exam Study GuideDocument35 pagesPhysical Assessment Exam Study GuideMustaf Mohamed91% (44)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ZAMIL PY Series Installation, Operation & Maintenance ManualDocument33 pagesZAMIL PY Series Installation, Operation & Maintenance Manualambuenaflor67% (9)
- Thoracic Hinge - Edited8.1.15 PDFDocument5 pagesThoracic Hinge - Edited8.1.15 PDFnambaccucNo ratings yet
- Nugget ListDocument1 pageNugget ListmsbunnileeNo ratings yet
- Cupping TherapyDocument6 pagesCupping TherapymsbunnileeNo ratings yet
- Icu Head To Toe AssessmentDocument3 pagesIcu Head To Toe Assessmentmsbunnilee100% (2)
- Clinical Learning ObjectivesDocument4 pagesClinical Learning ObjectivesmsbunnileeNo ratings yet
- NCLEX TIPS 2010 Final PDFDocument24 pagesNCLEX TIPS 2010 Final PDFmsbunnileeNo ratings yet
- Nurs 197 Paper PPD Cultural CareDocument1 pageNurs 197 Paper PPD Cultural CaremsbunnileeNo ratings yet
- Expanded PP AsmtDocument1 pageExpanded PP AsmtmsbunnileeNo ratings yet
- Key Concepts, Chapter 16, Documenting, Reporting, Conferring, and Using InformaticsDocument4 pagesKey Concepts, Chapter 16, Documenting, Reporting, Conferring, and Using InformaticsmsbunnileeNo ratings yet
- Key Concepts, Chapter 20, CommunicatorDocument2 pagesKey Concepts, Chapter 20, CommunicatormsbunnileeNo ratings yet
- Assessment of Fetal Well-Being Diagnostic Tests Sheet1Document2 pagesAssessment of Fetal Well-Being Diagnostic Tests Sheet1msbunnileeNo ratings yet
- Key Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthDocument4 pagesKey Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthmsbunnileeNo ratings yet
- Key Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthDocument4 pagesKey Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthmsbunnileeNo ratings yet
- Key Concepts, Chapter 14, ImplementingDocument3 pagesKey Concepts, Chapter 14, ImplementingmsbunnileeNo ratings yet
- KC Chapter 11Document3 pagesKC Chapter 11msbunnileeNo ratings yet
- KC Chapter 10Document4 pagesKC Chapter 10msbunnileeNo ratings yet
- KC Chapter 12Document2 pagesKC Chapter 12msbunnileeNo ratings yet
- KC Chapter 13Document3 pagesKC Chapter 13msbunnileeNo ratings yet
- KC Chapter 06Document2 pagesKC Chapter 06msbunnileeNo ratings yet
- KC Chapter 07Document3 pagesKC Chapter 07msbunnileeNo ratings yet
- 2016 RN Test Plan CandidateDocument61 pages2016 RN Test Plan CandidateKaren Mae Ü DonaireNo ratings yet
- The Nursing Student's Practical Guide To Writing Care Plans by Luanne BeginDocument67 pagesThe Nursing Student's Practical Guide To Writing Care Plans by Luanne Beginsoghosa100% (1)
- 1224 Threading Machine - Operator's Manual PDFDocument71 pages1224 Threading Machine - Operator's Manual PDFAlberto Flores FrancoNo ratings yet
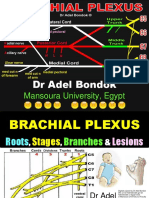
- Brachial Plexus, DR Adel BondokDocument20 pagesBrachial Plexus, DR Adel BondokSafeNo ratings yet
- Skull Osteology & Cranial Cavity - TUSKDocument66 pagesSkull Osteology & Cranial Cavity - TUSKterima kasihNo ratings yet
- 06 - Sullivan - C ReviewerDocument60 pages06 - Sullivan - C ReviewerCatrina TanNo ratings yet
- What Is Lateral Collateral Ligament Sprain?Document9 pagesWhat Is Lateral Collateral Ligament Sprain?mochamad ilham kurniaNo ratings yet
- Indian Fatal Accidents Act 1855Document2 pagesIndian Fatal Accidents Act 1855Gopi KrishnaNo ratings yet
- User GuideDocument5 pagesUser Guidecmkflorida7011No ratings yet
- Cerebral Blood Flow & StrokeDocument35 pagesCerebral Blood Flow & Stroke-'Henri Djhevon Kaary'-No ratings yet
- Bitts Park Risk AssessmentDocument4 pagesBitts Park Risk Assessmentapi-339095212No ratings yet
- Good Posture ManualDocument17 pagesGood Posture ManualJames Grobler100% (1)
- Ch-8 Body Movements - Day1Document12 pagesCh-8 Body Movements - Day1dr satnam kaurNo ratings yet
- PE03 Midterm Week 3 ModuleDocument6 pagesPE03 Midterm Week 3 ModuleCorn FlakesNo ratings yet
- Client Screening Website FormDocument2 pagesClient Screening Website FormBrett Whipp100% (2)
- PM00479 Titan Bioflex InfographicDocument2 pagesPM00479 Titan Bioflex InfographicMauro PojmaevichNo ratings yet
- Lab Safety Procedures and Common Lab EquipmentDocument18 pagesLab Safety Procedures and Common Lab EquipmentLuqman X AidilNo ratings yet
- Chinese Herbal FormulasDocument8 pagesChinese Herbal Formulasryandakota100% (1)
- Slip-And-Fall Facts by Easter Law FirmDocument3 pagesSlip-And-Fall Facts by Easter Law Firmjoe379No ratings yet
- Head To Toe Physical AssessmentDocument9 pagesHead To Toe Physical Assessmentthe studentNo ratings yet
- Additional RRLDocument3 pagesAdditional RRLManuel Jaro ValdezNo ratings yet
- Target MRB Test Series 1Document1 pageTarget MRB Test Series 1SanthiyaNo ratings yet
- High Riding ProstateDocument13 pagesHigh Riding ProstateHendry DimasNo ratings yet
- Ankle Injury EvaluationDocument7 pagesAnkle Injury EvaluationManiDeep ReddyNo ratings yet
- Full Download Ebook PDF Nursing and Midwifery Students Clinical Midwifery Survival Guide PDFDocument48 pagesFull Download Ebook PDF Nursing and Midwifery Students Clinical Midwifery Survival Guide PDFsharon.henry951100% (36)
- Floyd's 99 v. Chavalo 77 - Floyd's Barbershop Trademark Complaint PDFDocument13 pagesFloyd's 99 v. Chavalo 77 - Floyd's Barbershop Trademark Complaint PDFMark JaffeNo ratings yet
- A Fighter's Lines by Marzuki AliDocument5 pagesA Fighter's Lines by Marzuki AliAnonymous TADs3BevnNo ratings yet
- Fox Written RulingDocument62 pagesFox Written RulingAnthony WarrenNo ratings yet
- Let The Evidence Speak For ItselfDocument15 pagesLet The Evidence Speak For ItselfAnchiano AixNo ratings yet