You might also like
- Cure For All DiseasesDocument4 pagesCure For All DiseasesNiquezNo ratings yet
- Understanding & Practices of Weight ManagementDocument445 pagesUnderstanding & Practices of Weight ManagementOnlineGatha The Endless TaleNo ratings yet
- A Clinical Approach To Neuro-Ophthalmic DisordersDocument369 pagesA Clinical Approach To Neuro-Ophthalmic DisordersVictor Yunan Garcia100% (1)
- Diseases of Lens DR D.JLDocument113 pagesDiseases of Lens DR D.JLNithya GunasekaranNo ratings yet
- PBL Modul Blindness KLP 14Document25 pagesPBL Modul Blindness KLP 14033010969No ratings yet
- Imaging of OrbitDocument69 pagesImaging of OrbitFaisal ShembeshNo ratings yet
- Congenital Strabismus: S. Vanitha, B.optom, 3 YearDocument23 pagesCongenital Strabismus: S. Vanitha, B.optom, 3 YearDivya Priya Dharmalingam100% (1)
- Surgical Management of Third Nerve PalsyDocument7 pagesSurgical Management of Third Nerve Palsyhanaddul100% (1)
- Lactulose: (Enuluse, Kristalose, Duphalac, Chronulac Syrup)Document30 pagesLactulose: (Enuluse, Kristalose, Duphalac, Chronulac Syrup)Joanna Dela Torre100% (2)
- Neuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawangDocument65 pagesNeuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawanggeorgyNo ratings yet
- Atlas of Retinal OCTDocument211 pagesAtlas of Retinal OCTVianka García LópezNo ratings yet
- Anomalie VisionDocument13 pagesAnomalie VisionblueiceNo ratings yet
- Kanski S Clinical Ophthalmology A Systematic.20Document1 pageKanski S Clinical Ophthalmology A Systematic.20dyiah ayuNo ratings yet
- Diabetes Mellitus Overview LayDocument17 pagesDiabetes Mellitus Overview LaychelitvaleramdNo ratings yet
- Visual Fields Interpretation in Glaucoma A Focus On Static Automated PerimetryDocument8 pagesVisual Fields Interpretation in Glaucoma A Focus On Static Automated PerimetryMoisés Sergio Nina BaldeónNo ratings yet
- 20 Practical Ways To Kick Fear in The ButtDocument3 pages20 Practical Ways To Kick Fear in The ButtPrinsesaJuuNo ratings yet
- Congenital Nasolacrimal Duct ObstructionDocument43 pagesCongenital Nasolacrimal Duct ObstructionAnumeha JindalNo ratings yet
- TF00001028 (Autosaved)Document10 pagesTF00001028 (Autosaved)Cid MusaNo ratings yet
- Ptosis Definition of Eyelid Ptosis: Abnormally Low Position of The Upper Eyelid Margin Caused by PoorDocument6 pagesPtosis Definition of Eyelid Ptosis: Abnormally Low Position of The Upper Eyelid Margin Caused by PoortiamaharaniNo ratings yet
- Superior Oblik PalsyDocument13 pagesSuperior Oblik PalsyYunita ManurungNo ratings yet
- Diagnosis, Differential Diagnosis, And.5Document25 pagesDiagnosis, Differential Diagnosis, And.5Rahul RaiNo ratings yet
- Visual Field DefectsDocument5 pagesVisual Field DefectsHilary SteeleNo ratings yet
- CardiomyopathyDocument45 pagesCardiomyopathyHiLmy Zakiyah100% (1)
- Ocular TraumaDocument67 pagesOcular TraumaRenita Siwi M WNo ratings yet
- AdelineDocument34 pagesAdelineEmmanuel NdukaNo ratings yet
- ZEISS AngioPlex Case Reports US 31 150 0032IDocument12 pagesZEISS AngioPlex Case Reports US 31 150 0032Idarkspawn69No ratings yet
- College of Medicine and Health Science, Department of OptometryDocument47 pagesCollege of Medicine and Health Science, Department of Optometryhenok birukNo ratings yet
- The Glaucoma BookDocument1,019 pagesThe Glaucoma BookPotencia SalasNo ratings yet
- Ischemic Optic Neuropathies - S. HayrehDocument469 pagesIschemic Optic Neuropathies - S. HayrehEliMihaela100% (2)
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Retinal AnatomyDocument86 pagesRetinal AnatomySean ScogginsNo ratings yet
- 2019-Epilepsy Overview and Revised Classification Of.4-2Document16 pages2019-Epilepsy Overview and Revised Classification Of.4-2BryanNo ratings yet
- TrabeculectomyDocument28 pagesTrabeculectomyAlfu RafdiNo ratings yet
- Nursing Care of DiarrheaDocument30 pagesNursing Care of DiarrheayustiNo ratings yet
- NICE Guidlines 2022 Epilepsies in Children Young People and Adults PDFDocument139 pagesNICE Guidlines 2022 Epilepsies in Children Young People and Adults PDFGabriela WidjajaNo ratings yet
- Red Eye: A Guide For Non-Specialists: MedicineDocument14 pagesRed Eye: A Guide For Non-Specialists: MedicineFapuw Parawansa100% (1)
- 2735 Pediatric Cataract Manual - CompressedDocument66 pages2735 Pediatric Cataract Manual - CompressedKevin RamsahaiNo ratings yet
- Anaesthesia For Cataract Surgery and Its ComplicationDocument28 pagesAnaesthesia For Cataract Surgery and Its Complicationbala16690No ratings yet
- A Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyDocument7 pagesA Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyIJAR JOURNALNo ratings yet
- Diplopia (Double Vision), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiplopia (Double Vision), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Ocular AnesthesiaDocument61 pagesOcular AnesthesiaAdarsh Keshari100% (1)
- Optic Neuritis: DR Rishi JhalaniDocument64 pagesOptic Neuritis: DR Rishi JhalaniRishi Jhalani100% (1)
- Diagnosis Approach of Optic Neuritis 2155 9562 1000345Document13 pagesDiagnosis Approach of Optic Neuritis 2155 9562 1000345Juaan AvilaNo ratings yet
- Nystagmus and Localizing ValuesDocument9 pagesNystagmus and Localizing Valueshikmat sheraniNo ratings yet
- AION Anterior Ischemic Optic Neuropathy AIONDocument22 pagesAION Anterior Ischemic Optic Neuropathy AIONNyak Rahmat100% (1)
- Clinical Procedures in Primary Eye Care-David Elliott - 158Document3 pagesClinical Procedures in Primary Eye Care-David Elliott - 158Danielle SangalangNo ratings yet
- Non-Concomitant Strabismus 2Document60 pagesNon-Concomitant Strabismus 2Ijeoma Okpalla100% (2)
- Astigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAstigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Glaucoma LectureDocument166 pagesGlaucoma LectureSonali Gupta100% (1)
- 106 - CH 22 - Anomalies of Convergence and Divergence, P. 500-507Document8 pages106 - CH 22 - Anomalies of Convergence and Divergence, P. 500-507Francisco Vicent PachecoNo ratings yet
- Hypertensive Retinopathy - Yanoff and DukerDocument13 pagesHypertensive Retinopathy - Yanoff and DukerriveliNo ratings yet
- Managing Complications in Glaucoma SurgeryDocument121 pagesManaging Complications in Glaucoma Surgeryshetya_8212No ratings yet
- Anesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFDocument11 pagesAnesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFtiaraleshaNo ratings yet
- Traumatic Optic Neuropathy - Prof. N. KarthikeyanDocument22 pagesTraumatic Optic Neuropathy - Prof. N. KarthikeyanDobrin_Nicolai_8219No ratings yet
- Anaesthesia For Eye Surgery 1208455650159329 8 (2) .PPTDSDDocument32 pagesAnaesthesia For Eye Surgery 1208455650159329 8 (2) .PPTDSDfariz_maulana88_9890No ratings yet
- Understanding Visual Fields Part I Goldmann PerimeDocument11 pagesUnderstanding Visual Fields Part I Goldmann PerimeAngelaNo ratings yet
- Case Studies PresbyopiaDocument33 pagesCase Studies PresbyopiaMalaika ZubairNo ratings yet
- Oculomotor Nerve: Arista Prima NDocument7 pagesOculomotor Nerve: Arista Prima NArista Prima N100% (1)
- Extraocular Muscle Anatomy and Physiology NotesDocument13 pagesExtraocular Muscle Anatomy and Physiology NotesRahul Jasu100% (1)
- Asbury - Assesment of Current Diagnostic Criteria For GBSDocument4 pagesAsbury - Assesment of Current Diagnostic Criteria For GBSMarcelo BedoyaNo ratings yet
- Periorbital and Orbital CellulitisDocument51 pagesPeriorbital and Orbital CellulitisJoanne BlancoNo ratings yet
- Visual Field DefectsDocument1 pageVisual Field DefectsLauren LevyNo ratings yet
- 09 LensDocument37 pages09 LensFrederica Mutiara100% (1)
- Strabismus Quick GuideDocument4 pagesStrabismus Quick Guideghitza80100% (1)
- Amrit Bindu A4 Display PosterDocument1 pageAmrit Bindu A4 Display PostersdoctorNo ratings yet
- CHRONIC HEPATITIS Prof DR Tarek ShetaDocument38 pagesCHRONIC HEPATITIS Prof DR Tarek ShetaSheren GamaleldenNo ratings yet
- QuestionsDocument6 pagesQuestionsLorvic Andrew Juanson UmaliNo ratings yet
- Ed 2020 1Document25 pagesEd 2020 1Alejandra Loyo MonsalveNo ratings yet
- Jurnal 2Document0 pagesJurnal 2Seftiana SaftariNo ratings yet
- AIIMS PG 2005 Question Paper PDFDocument26 pagesAIIMS PG 2005 Question Paper PDFramNo ratings yet
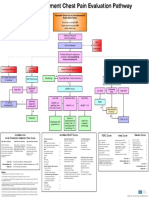
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Significant Life Experiences of Healthcare Workers in Olongapo City During The Start of COVID-19 OutbreakDocument301 pagesSignificant Life Experiences of Healthcare Workers in Olongapo City During The Start of COVID-19 OutbreakNexander OcampoNo ratings yet
- Speech DelayDocument16 pagesSpeech Delayian ismail100% (1)
- Newsletter: WHO PharmaceuticalsDocument27 pagesNewsletter: WHO PharmaceuticalsGammachuu Leejjiisa Mul'ataa SabbooqaaNo ratings yet
- IM-CAP Concept MapDocument1 pageIM-CAP Concept MapTrisNo ratings yet
- Prosthodontic DiagnosisDocument15 pagesProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
- Submandibular Abscess Caused by Salmonella - International Journal of Oral and Maxillofacial SurgeryDocument1 pageSubmandibular Abscess Caused by Salmonella - International Journal of Oral and Maxillofacial SurgeryTri Sakti Sunda RomdhoniNo ratings yet
- Pub1566 WebDocument124 pagesPub1566 WebRadoi Sandina RodicaNo ratings yet
- Translate TineaDocument12 pagesTranslate TineaIndah Permata SariNo ratings yet
- READINGDocument21 pagesREADINGdiya baby100% (1)
- English Task IDocument4 pagesEnglish Task Idwi septiyaniNo ratings yet
- Intensive Care Unit Acquired WeaknessDocument35 pagesIntensive Care Unit Acquired WeaknessEviNo ratings yet
- Krok2 - Medicine - 2008Document26 pagesKrok2 - Medicine - 2008Badriya YussufNo ratings yet
- Understanding AuriculotherapyDocument4 pagesUnderstanding AuriculotherapyFelipe de Jesus HernandezNo ratings yet
- Jandy Aqualink RS Owners ManualDocument88 pagesJandy Aqualink RS Owners ManualAeres707No ratings yet
- Your Dynamic Profile: Wellness ReportDocument17 pagesYour Dynamic Profile: Wellness Reportvica sibueaNo ratings yet
- 5 6323480972671058006Document195 pages5 6323480972671058006Anonymous QOCn5dNo ratings yet