You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- PRN Medications: Indications & UseDocument23 pagesPRN Medications: Indications & Usedis_is_me100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Script Otomatis BTC SpinerDocument2 pagesScript Otomatis BTC SpinerAdy Nanda Lamuda25% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- July Exclusive Lines 2015Document1 pageJuly Exclusive Lines 2015dis_is_meNo ratings yet
- July Deals Injectables 2015Document1 pageJuly Deals Injectables 2015dis_is_meNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- July Deals Orals 2015Document1 pageJuly Deals Orals 2015dis_is_meNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Senior Citizen NewDocument3 pagesSenior Citizen Newdis_is_meNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Compilation of MS NotesDocument81 pagesCompilation of MS Notesdis_is_meNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Smoking: Good or Bad?Document56 pagesSmoking: Good or Bad?dis_is_meNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grow and Be Like The MolaveDocument3 pagesGrow and Be Like The MolaveMaria Fatima BagayNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 80do Food-List Vegan 021318Document4 pages80do Food-List Vegan 021318javi martinezNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Nutritional AssessmentDocument5 pagesNutritional AssessmentimnasNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Surgery 1.04 Surgical Diseases of The Thyroid GlandDocument15 pagesSurgery 1.04 Surgical Diseases of The Thyroid GlandjayaeroneNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
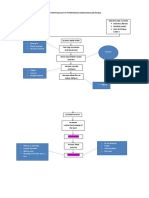
- Pathophysiology of Hypertensive Cardiovascular Disease: Chest Pain Muscle Weakness Shortness of BreathDocument2 pagesPathophysiology of Hypertensive Cardiovascular Disease: Chest Pain Muscle Weakness Shortness of BreathCyril Jane Caanyagan AcutNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Task 1. Read and Translate The Words:: Unit 8. Nutrition and ObesityDocument3 pagesTask 1. Read and Translate The Words:: Unit 8. Nutrition and ObesityKomron JonNo ratings yet
- PE - Physical FitnessDocument5 pagesPE - Physical FitnessHenriana PagkaliwanganNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Wardlaws Perspectives in Nutrition 10th Edition Byrd Bredbenner Solutions ManualDocument26 pagesWardlaws Perspectives in Nutrition 10th Edition Byrd Bredbenner Solutions ManualMeganBensonmepc100% (31)
- Assessment of Mold and Yeast in Some Bakery Products of Lahore, Pakistan Based On LM and SEMDocument8 pagesAssessment of Mold and Yeast in Some Bakery Products of Lahore, Pakistan Based On LM and SEMHiệp Lê QuangNo ratings yet
- CoenzymesDocument60 pagesCoenzymesraddagNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Nutrition and Dietetics Midterm Exam October 2018Document14 pagesNutrition and Dietetics Midterm Exam October 2018Daniel Laoaten100% (2)
- Nutrition Plan For PCOS PCODDocument3 pagesNutrition Plan For PCOS PCODshikta sanyalNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Lifegear 97370Document36 pagesLifegear 97370mrmachNo ratings yet
- The Role of High Sugar Consumption On Diabetes Development Among Adults Living in The United States Research PaperDocument12 pagesThe Role of High Sugar Consumption On Diabetes Development Among Adults Living in The United States Research Paperapi-301801285No ratings yet
- Executive Summary: Tri Queen Shake Feasibility StudyDocument54 pagesExecutive Summary: Tri Queen Shake Feasibility StudyDM Lucero IlaNo ratings yet
- MSM Sulfur MSM - Methylsulfonylmethane PDFDocument6 pagesMSM Sulfur MSM - Methylsulfonylmethane PDFmarkuswolf11100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Managing Encopresis in The Pediatric Setting: The DSM-5 Autism Criteria: A Social Rather - .Document5 pagesManaging Encopresis in The Pediatric Setting: The DSM-5 Autism Criteria: A Social Rather - .Yurizna Almira Nst IINo ratings yet
- ERFLDocument8 pagesERFLAitor StoutNo ratings yet
- NUTRIDocument20 pagesNUTRIJinnijinniNo ratings yet
- Convenience Food: Putting Health and The Environment On The MenuDocument4 pagesConvenience Food: Putting Health and The Environment On The MenuSwapnil LilkeNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Template For Care Plan AssignmentDocument8 pagesTemplate For Care Plan AssignmentAnn OgoloNo ratings yet
- Angga Pratama Haloho - 2003511035 - Abstract Assigment - Class ADocument3 pagesAngga Pratama Haloho - 2003511035 - Abstract Assigment - Class AChristmas14 ManjorangFMIPANo ratings yet
- Abs. Booty. Total Body.: Starter GuideDocument8 pagesAbs. Booty. Total Body.: Starter GuidedoneitwellNo ratings yet
- Enteral Nutrition - Yudhi AdriantoDocument41 pagesEnteral Nutrition - Yudhi AdriantoAri SusandiNo ratings yet
- Ecobiol Aqua - A Unique and Highly Effective Single Strain ProbioticDocument5 pagesEcobiol Aqua - A Unique and Highly Effective Single Strain ProbioticInternational Aquafeed magazineNo ratings yet
- Anti Diabetic HerbsDocument25 pagesAnti Diabetic HerbsSmritaPradhan PNo ratings yet
- Nursing Assessment FormDocument8 pagesNursing Assessment FormMaila Carl M. MorantteNo ratings yet
- Care of The NewbornDocument5 pagesCare of The Newbornbuzz Q100% (2)
- Curs 3 Lecture Nutrition and Bacteria CultivationDocument74 pagesCurs 3 Lecture Nutrition and Bacteria CultivationHåíthãm KhãtïßNo ratings yet
- Vyntus-CPX-Canopy BR EN PDFDocument4 pagesVyntus-CPX-Canopy BR EN PDFLajoskaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- I ObjectivesDocument6 pagesI ObjectivesMARITESS COLLADONo ratings yet