You might also like
- Lec Post OpDocument15 pagesLec Post OpAilyne A. CleofeNo ratings yet
- Post Operative ReportDocument14 pagesPost Operative ReportAilyne A. CleofeNo ratings yet
- Osteoporosis Basics: by Paige Bierma and Chris Woolston What Is Osteoporosis?Document6 pagesOsteoporosis Basics: by Paige Bierma and Chris Woolston What Is Osteoporosis?Ailyne A. CleofeNo ratings yet
- Mi and AnginaDocument5 pagesMi and AnginaAilyne A. Cleofe100% (1)
- Introduction To PharmacologyDocument21 pagesIntroduction To Pharmacologyderic100% (12)
- Preventing Falls and Fractures: by Beth Witrogen and Chris Woolston, M.S. How Can I Prevent Fractures?Document3 pagesPreventing Falls and Fractures: by Beth Witrogen and Chris Woolston, M.S. How Can I Prevent Fractures?Ailyne A. Cleofe100% (1)
- Pharmacology ReviewerDocument13 pagesPharmacology ReviewerAbril C. Tiraña100% (1)
- ScoliosisDocument2 pagesScoliosisAilyne A. CleofeNo ratings yet
- Skin PrepDocument13 pagesSkin PrepEricsonMitraNo ratings yet
- Lecture - Chronically IllDocument14 pagesLecture - Chronically IllAilyne A. Cleofe100% (2)
- Cleft Lip and PalateDocument34 pagesCleft Lip and Palateapi-1950064167% (3)
- GOUTDocument3 pagesGOUTAilyne A. CleofeNo ratings yet
- Appendectomy/ Appendicitis Case StudyDocument15 pagesAppendectomy/ Appendicitis Case StudyApril93% (30)
- Common Meds in ErDocument27 pagesCommon Meds in ErAilyne A. CleofeNo ratings yet
- Case Study Acute PancreatitisDocument62 pagesCase Study Acute PancreatitisAilyne A. CleofeNo ratings yet
- TheDocument6 pagesTheAilyne A. CleofeNo ratings yet
- Case Study in Acute PancreatitisDocument2 pagesCase Study in Acute PancreatitisAilyne A. CleofeNo ratings yet
- Acute Pancreatitis Resolved CholecystolithiasisDocument97 pagesAcute Pancreatitis Resolved Cholecystolithiasisemofreo100% (1)
- Pharmacology Case StudyDocument11 pagesPharmacology Case StudyAilyne A. CleofeNo ratings yet
- Acute Pancreatitis Resolved CholecystolithiasisDocument97 pagesAcute Pancreatitis Resolved Cholecystolithiasisemofreo100% (1)
- Adolescent LongitudinalDocument5 pagesAdolescent LongitudinalAilyne A. Cleofe100% (1)
- Acute Pancreatitis Resolved CholecystolithiasisDocument97 pagesAcute Pancreatitis Resolved Cholecystolithiasisemofreo100% (1)
- Concept and Mapping For Rheumatic Heart DiseaseDocument5 pagesConcept and Mapping For Rheumatic Heart DiseaseAilyne A. CleofeNo ratings yet
- What Is Gestational Hypertension?Document5 pagesWhat Is Gestational Hypertension?Ailyne A. CleofeNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cyclic Progesterone Therapy Patient HandoutDocument1 pageCyclic Progesterone Therapy Patient HandoutMuhammadRizalNNo ratings yet
- Pharmacological evidence of Hibiscus extractsDocument10 pagesPharmacological evidence of Hibiscus extractsAna TorrealbaNo ratings yet
- Ill Effects of Air Water and Noise PollutionDocument13 pagesIll Effects of Air Water and Noise PollutionnatashaNo ratings yet
- Apoptosis in CancerDocument14 pagesApoptosis in CancerCarina Isabel Bento Marques CoelhoNo ratings yet
- Contaminarea Cu MelaninaDocument8 pagesContaminarea Cu Melaninadiana fenichiuNo ratings yet
- S807 Mini Review v4Document37 pagesS807 Mini Review v4Daen de LeonNo ratings yet
- Knee Pain and HomoeopathyDocument4 pagesKnee Pain and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (3)
- Upper GIT 1Document18 pagesUpper GIT 1Zuhra JabeenNo ratings yet
- Ultrasound in Obstetrics and Gynaecology: ReviewDocument9 pagesUltrasound in Obstetrics and Gynaecology: ReviewGustina Maryanti MooyNo ratings yet
- Reproductive SystemDocument89 pagesReproductive SystemIbrahim Mahmoud Ali100% (1)
- Risks Vs HazardDocument1 pageRisks Vs HazardIbrahim BashaNo ratings yet
- Acute Necrotizing PancreatitisDocument37 pagesAcute Necrotizing PancreatitisVania SuSanchezNo ratings yet
- Osteoid Osteoma: CT-guided Radiofrequency Ablation: Original StudyDocument6 pagesOsteoid Osteoma: CT-guided Radiofrequency Ablation: Original StudyNurul FatimahNo ratings yet
- Infectious DiseasesDocument10 pagesInfectious DiseasesSayali KunteNo ratings yet
- Whoqol 100 PDFDocument21 pagesWhoqol 100 PDFSis SukarnoNo ratings yet
- Interview With T.C. FryDocument18 pagesInterview With T.C. Fryraweater100% (1)
- Ophthalmonics 1st EditionDocument116 pagesOphthalmonics 1st Editiondhavalb2086% (7)
- Chest - Surgical - Pathology - X-Rays (NXPowerLite)Document57 pagesChest - Surgical - Pathology - X-Rays (NXPowerLite)Drgeorge SaadNo ratings yet
- SmokingDocument29 pagesSmokingKris NNo ratings yet
- Hijama PointsDocument23 pagesHijama PointsShahbaz Ahmed100% (1)
- Placental Pathology Notes Aspen 2014 - Fritsch FinalDocument46 pagesPlacental Pathology Notes Aspen 2014 - Fritsch Finalmostachek0% (1)
- Musculoskeletal Imaging 2015Document79 pagesMusculoskeletal Imaging 2015Faiq Syukri Bin SaparudinNo ratings yet
- Urogenital Imejing: DR - Ali Imran Lubis SP - RadDocument16 pagesUrogenital Imejing: DR - Ali Imran Lubis SP - RadPutri Sari SeptirianiNo ratings yet
- Retire HappyDocument266 pagesRetire HappyEdsel Llave100% (3)
- Food Adultration ObjectiveDocument11 pagesFood Adultration ObjectiveGourav Som0% (1)
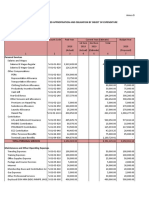
- Programmed Appropriation and Obligation by Object of ExpenditureDocument7 pagesProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoNo ratings yet
- 2017 - Tecnología CosméticaDocument54 pages2017 - Tecnología CosméticaCésar Rosado Avila ToñoNo ratings yet
- 14 Meron Mehari Kifle 2016 Knowledge and Practice of Breast Self Examination Among Female College Students in EritreaDocument6 pages14 Meron Mehari Kifle 2016 Knowledge and Practice of Breast Self Examination Among Female College Students in EritreaArick Frendi AndriyanNo ratings yet
- Adrenal Cortex Disease and PhaeochromocytomasDocument47 pagesAdrenal Cortex Disease and PhaeochromocytomasJamaluddin Ahmad A.MNo ratings yet