You might also like
- Company Instrumentation & Control Specialists, Inc Document ID No. Department/s Contractor Revision No Job Title Coring Works Effective DateDocument11 pagesCompany Instrumentation & Control Specialists, Inc Document ID No. Department/s Contractor Revision No Job Title Coring Works Effective DateJayson EscamillanNo ratings yet
- JSA-054 Crossing WorksDocument6 pagesJSA-054 Crossing WorksMajdiSahnounNo ratings yet
- Jsa For HydrotestDocument10 pagesJsa For HydrotestAnonymous CcGYhZb080% (5)
- 5.19 JSP Electrical Power InstallationDocument4 pages5.19 JSP Electrical Power InstallationDarius DsouzaNo ratings yet
- JSA-001 Earth Works & Civil WorksDocument5 pagesJSA-001 Earth Works & Civil WorksMoaatazz Nouisri50% (2)
- JSA-049 LVS Equipment & Material InstallationDocument10 pagesJSA-049 LVS Equipment & Material InstallationMoaatazz NouisriNo ratings yet
- Job Safety Analysis Sheet: Operation Concrete Batching PlantDocument2 pagesJob Safety Analysis Sheet: Operation Concrete Batching Plantzabiulla100% (7)
- House Keeping Check List: Sl. No. DescriptionDocument24 pagesHouse Keeping Check List: Sl. No. Descriptionsanjeev kumarNo ratings yet
- JSA-049 Valves & Support Installation and DismantlingDocument4 pagesJSA-049 Valves & Support Installation and DismantlingMoaatazz Nouisri75% (4)
- Etap - Relay CoordinationDocument311 pagesEtap - Relay CoordinationManohar Potnuru100% (1)
- Job Hazard Analysis (Jha) WorksheetDocument4 pagesJob Hazard Analysis (Jha) WorksheetSamer AlsumaryNo ratings yet
- GH13 Heavy Duty Body Installation Manual PDFDocument132 pagesGH13 Heavy Duty Body Installation Manual PDFPrashant Sharma100% (14)
- JSA For Rope Access Services (24-Sep-14)Document8 pagesJSA For Rope Access Services (24-Sep-14)TomasPavlovic100% (1)
- Flushingchemical Cleaning of Chilled Water PipesDocument9 pagesFlushingchemical Cleaning of Chilled Water PipesAnandu AshokanNo ratings yet
- JSA-019 Manual WeldingDocument5 pagesJSA-019 Manual WeldingMoaatazz Nouisri0% (1)
- Iso 45001Document10 pagesIso 45001sanjeev kumar0% (1)
- Risk Assessment Form: Project: Gem Residences Location: E. Rodriguez Ave. C5, Pasig CityDocument2 pagesRisk Assessment Form: Project: Gem Residences Location: E. Rodriguez Ave. C5, Pasig CityJhundel FactorNo ratings yet
- Serial Index CaterpillarDocument260 pagesSerial Index CaterpillarRamón Mangles90% (10)
- Legal Register For Constriction SiteDocument33 pagesLegal Register For Constriction Sitesanjeev kumarNo ratings yet
- Risk AssessmentDocument6 pagesRisk Assessmentkaruppusamymari100% (1)
- Jsa Painting2Document72 pagesJsa Painting2surender b100% (1)
- 10 - Cherry Picker Inspection ChecklistDocument1 page10 - Cherry Picker Inspection Checklistsanjeev kumarNo ratings yet
- 01 - Gas Cutting Set Inspection ChecklistDocument1 page01 - Gas Cutting Set Inspection Checklistsanjeev kumar100% (1)
- Safety Behavior Observation Checklist: Observe Quietly. Mark Each Observation ItemDocument1 pageSafety Behavior Observation Checklist: Observe Quietly. Mark Each Observation Itemkhrayzie bhone100% (2)
- Driving Goods VehiclesDocument336 pagesDriving Goods VehiclesAsmawi AkhirNo ratings yet
- Applied Operational Excellence for the Oil, Gas, and Process IndustriesFrom EverandApplied Operational Excellence for the Oil, Gas, and Process IndustriesRating: 4.5 out of 5 stars4.5/5 (4)
- 10 - Cherry Picker Inspection ChecklistDocument1 page10 - Cherry Picker Inspection Checklistsanjeev kumarNo ratings yet
- Tra 002Document6 pagesTra 002Bilal0% (1)
- 02 - Transformer (Testing)Document5 pages02 - Transformer (Testing)Saravanan SaraNo ratings yet
- Positif Jsa HMCFDDocument4 pagesPositif Jsa HMCFDBryant TorresNo ratings yet
- FT20 Internal Audit PlanDocument5 pagesFT20 Internal Audit Plansanjeev kumarNo ratings yet
- Water Pump JsaDocument2 pagesWater Pump JsajvmspNo ratings yet
- The Relevance of YS/UTS RatioDocument21 pagesThe Relevance of YS/UTS RatiocarrespmNo ratings yet
- BBS ChecklistDocument3 pagesBBS ChecklistTarun KakkarNo ratings yet
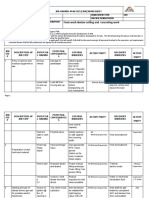
- Job Safety Analysis: 10.06.2017 Page 1 of 7Document7 pagesJob Safety Analysis: 10.06.2017 Page 1 of 7Raghava RichhuNo ratings yet
- Software Quality Assurance IntroductionDocument72 pagesSoftware Quality Assurance Introductionfmohiy100% (6)
- OHSE - ISO 45001-2018 Overview - GoldDocument73 pagesOHSE - ISO 45001-2018 Overview - Goldsanjeev kumar100% (15)
- FT39-Emergency Rescue PlanDocument25 pagesFT39-Emergency Rescue Plansanjeev kumarNo ratings yet
- Safety AuditSDocument5 pagesSafety AuditSsanjeev kumarNo ratings yet
- Total Productive Maintenance (TPM) : DescriptionDocument3 pagesTotal Productive Maintenance (TPM) : Descriptionsanjeev kumar100% (1)
- Content Analysis in The Social Sciences From Manual To Automated ApproachesDocument75 pagesContent Analysis in The Social Sciences From Manual To Automated Approachesdiablero999No ratings yet
- Pragmatic Electrical Engineering: FundamentalsDocument201 pagesPragmatic Electrical Engineering: FundamentalsaminmominNo ratings yet
- Jsa Dismantling The Wooden Framework-NewDocument3 pagesJsa Dismantling The Wooden Framework-NewHow Chin Engineering Sdn BhdNo ratings yet
- JOB Observation Checklist Safe UnsafeDocument3 pagesJOB Observation Checklist Safe UnsafeHelp Tubestar CrewNo ratings yet
- JHA Overhead Cleaning MP16Document4 pagesJHA Overhead Cleaning MP16Jay JocoNo ratings yet
- Cutting, Pulling and Rerouting of Cathodic Protection CablesDocument1 pageCutting, Pulling and Rerouting of Cathodic Protection CablesVIctor OdususiNo ratings yet
- 1 SurveyDocument5 pages1 Survey王志伟0% (1)
- JHA ISO Container Lifting Point MPI InspectionDocument7 pagesJHA ISO Container Lifting Point MPI InspectionMohamedNo ratings yet
- P12 - CHEAC - New Camp - STA - Installation of Fence - 23 Mar 2023Document3 pagesP12 - CHEAC - New Camp - STA - Installation of Fence - 23 Mar 2023imranNo ratings yet
- Hydro TestingDocument6 pagesHydro Testingchunxing yaoNo ratings yet
- HP Steam Superheater 2 Intermediate Tube Sheets Repair JSADocument1 pageHP Steam Superheater 2 Intermediate Tube Sheets Repair JSAVIctor OdususiNo ratings yet
- PLO's Attributes: Very Poor Poor Fair Good Excellent Total Marks 0 1-3 4-6 7-8 9-10Document2 pagesPLO's Attributes: Very Poor Poor Fair Good Excellent Total Marks 0 1-3 4-6 7-8 9-10Malik gNo ratings yet
- MSSB-JHA-Hot WorkDocument3 pagesMSSB-JHA-Hot WorkELDIABLO 24KNo ratings yet
- JHA - Earthing Lightning Protection & Cable Tray Instalation System - Docx - PCTLDocument8 pagesJHA - Earthing Lightning Protection & Cable Tray Instalation System - Docx - PCTLOmkar MishraNo ratings yet
- CAAF-309-AWRG-1.1-Maintenance Organization Approval Renewal ExtensionDocument6 pagesCAAF-309-AWRG-1.1-Maintenance Organization Approval Renewal ExtensionMubasher YousafNo ratings yet
- Job Safety Analysis Worksheet: HSE-JSA/XII/17Document1 pageJob Safety Analysis Worksheet: HSE-JSA/XII/17Bayu HidayatNo ratings yet
- JSA (Rev1 6.4.13) Set-Up Safe House Habitat.Document4 pagesJSA (Rev1 6.4.13) Set-Up Safe House Habitat.Danial AfandiNo ratings yet
- Hiring of DozerDocument9 pagesHiring of DozerDwitikrushna RoutNo ratings yet
- JHA (85T Crawler Crane & Drill Rig Machine Assembling and Inspection)Document2 pagesJHA (85T Crawler Crane & Drill Rig Machine Assembling and Inspection)Armando AballeNo ratings yet
- Day 3 Job Hazard Analysis (Handout)Document6 pagesDay 3 Job Hazard Analysis (Handout)mike camsNo ratings yet
- Civil Works For BORF SHELTER FOR PPTEP'S PRODUCTIONDocument6 pagesCivil Works For BORF SHELTER FOR PPTEP'S PRODUCTIONMohammad Irfan Kiki IsmailNo ratings yet
- JSA Install Pipe SupportDocument6 pagesJSA Install Pipe Supportem_we19No ratings yet
- JSA Installation Spool PipeDocument5 pagesJSA Installation Spool Pipeem_we19No ratings yet
- Job Safety Analysis Forms: Job/Task: Installation For Transformer Date: 9 Januari 2021Document3 pagesJob Safety Analysis Forms: Job/Task: Installation For Transformer Date: 9 Januari 2021Akhli RohmatulohNo ratings yet
- JHA For ThrustboringDocument5 pagesJHA For ThrustboringoverhauldeglobalNo ratings yet
- Arc WeldingDocument4 pagesArc WeldingJeffersonDeGuiaNo ratings yet
- Excavation Work RISK ASSESSMENTDocument8 pagesExcavation Work RISK ASSESSMENTVimal ViswanathNo ratings yet
- STA ElectricalDocument3 pagesSTA ElectricalimranNo ratings yet
- PTA-JSA-001-Mobilization Deployment of Manpower & Beginning of The JobDocument3 pagesPTA-JSA-001-Mobilization Deployment of Manpower & Beginning of The JobSaiyad RiyazaliNo ratings yet
- Grinding Work JsaDocument2 pagesGrinding Work JsaAKBAR ALINo ratings yet
- Equipment/reactor Erection Work JsaDocument3 pagesEquipment/reactor Erection Work JsaAKBAR ALINo ratings yet
- 5.19 JSP ScaffoldDocument4 pages5.19 JSP Scaffoldpoorm879No ratings yet
- 09.2014-Install Formwork, Re-Bar Setting and HousekeepingDocument8 pages09.2014-Install Formwork, Re-Bar Setting and Housekeepingاسامه محمد راضي جعفرNo ratings yet
- JSA TubingDocument9 pagesJSA TubingSubbu AbuNo ratings yet
- HIRAC - AC Cooler Blower (Daily Inspection)Document2 pagesHIRAC - AC Cooler Blower (Daily Inspection)Randy PedrozaNo ratings yet
- Proposed 2 Torre Lorenzo: Taft Avenue, ManilaDocument45 pagesProposed 2 Torre Lorenzo: Taft Avenue, ManilaMariel ColladoNo ratings yet
- Non Routine Work PolicyDocument4 pagesNon Routine Work PolicyK S KumaraNo ratings yet
- Jsa For Concreate and CivilworksDocument7 pagesJsa For Concreate and CivilworksAnna JisabaNo ratings yet
- JSA - 017# PengecoranDocument6 pagesJSA - 017# PengecoranGoldwin Ricky AritonangNo ratings yet
- 10 - Cherry Picker Inspection ChecklistDocument1 page10 - Cherry Picker Inspection Checklistsanjeev kumar100% (1)
- 08 - First Aid Box Inspection ChecklistDocument1 page08 - First Aid Box Inspection Checklistsanjeev kumarNo ratings yet
- 9 Colour Code of Lubricants Alt 1Document3 pages9 Colour Code of Lubricants Alt 1sanjeev kumarNo ratings yet
- o Ehs 08 Health & Safety Control PlanDocument1 pageo Ehs 08 Health & Safety Control Plansanjeev kumarNo ratings yet
- Rating: Company Rating A 2 B 1 C 2 D 3 E 4 F 2 G H I J KDocument2 pagesRating: Company Rating A 2 B 1 C 2 D 3 E 4 F 2 G H I J Ksanjeev kumarNo ratings yet
- Airr CPPDocument121 pagesAirr CPPsanjeev kumarNo ratings yet
- Ohsas 18001 2007Document32 pagesOhsas 18001 2007sanjeev kumarNo ratings yet
- Plant IlluminationDocument1 pagePlant Illuminationsanjeev kumarNo ratings yet
- Root Causes and CAPADocument27 pagesRoot Causes and CAPAsanjeev kumarNo ratings yet
- Floor PlanDocument1 pageFloor Plansanjeev kumarNo ratings yet
- TML Sop HT Switch BoardDocument4 pagesTML Sop HT Switch Boardsanjeev kumarNo ratings yet
- Sr. No Equipment Name Activity 17-Sep-17Document32 pagesSr. No Equipment Name Activity 17-Sep-17sanjeev kumarNo ratings yet
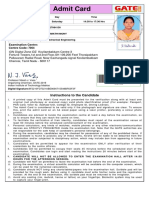
- Admit Card: Examination Centre: Centre CodeDocument1 pageAdmit Card: Examination Centre: Centre CodekrishnaNo ratings yet
- Advant Controller 4050series eDocument124 pagesAdvant Controller 4050series eABVSAINo ratings yet
- Kalkhoff Users ManualDocument148 pagesKalkhoff Users Manualanonms_accNo ratings yet
- Arco Solar Inc.: Case Analysis OnDocument12 pagesArco Solar Inc.: Case Analysis OnAnish RajNo ratings yet
- Status of ECSS E-30 - Space Engineering Handbooks On CDROM: Structural Materials Handbook, Insert Design Handbook and Adhesive Bonding HandbookDocument1 pageStatus of ECSS E-30 - Space Engineering Handbooks On CDROM: Structural Materials Handbook, Insert Design Handbook and Adhesive Bonding HandbookNetrom09No ratings yet
- Railway-4 Permanent Way & Alignment (Lecture-4)Document17 pagesRailway-4 Permanent Way & Alignment (Lecture-4)OBIDUR RAHMAN 1701085No ratings yet
- D-1967 (Clean) Quilting Machine ManualDocument33 pagesD-1967 (Clean) Quilting Machine Manualvalter craccoNo ratings yet
- Sap Accrual EngineDocument2 pagesSap Accrual Enginerohit12345aNo ratings yet
- CCR Equipment ListDocument1 pageCCR Equipment Listbehzad parsiNo ratings yet
- Taking Your Pump System Efficiency To New Heights: CU 352 Multi-Pump ControllerDocument4 pagesTaking Your Pump System Efficiency To New Heights: CU 352 Multi-Pump Controllersushant moreyNo ratings yet
- Global Deduplication Array Administration Guide: DD OS 5.0Document70 pagesGlobal Deduplication Array Administration Guide: DD OS 5.0Rajesh KumarNo ratings yet
- C/C++ Programming Language NotesDocument68 pagesC/C++ Programming Language Notesctf challengeNo ratings yet
- Global Edge Interview ExperienceDocument2 pagesGlobal Edge Interview Experienceshafi hasmaniNo ratings yet
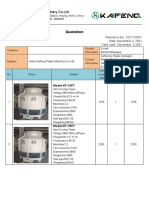
- KAIFENG Quotation For 150T Cooling TowerDocument13 pagesKAIFENG Quotation For 150T Cooling TowerEslam A. FahmyNo ratings yet
- SearchBot Results For Touchstone 1Document6 pagesSearchBot Results For Touchstone 1CNo ratings yet
- SAP BW Basic Configuration SettingsDocument29 pagesSAP BW Basic Configuration SettingsSIKANDARNo ratings yet
- 100124119Document175 pages100124119mkeiwuaNo ratings yet
- Patrick C Hall@yahoo - com-TruthfinderReportDocument13 pagesPatrick C Hall@yahoo - com-TruthfinderReportsmithsmithsmithsmithsmithNo ratings yet
- BK Report and ProjectDocument55 pagesBK Report and ProjecttesfuNo ratings yet
- Parts List: 8108.010 MagnumDocument16 pagesParts List: 8108.010 MagnumRoque LlamoccaNo ratings yet
- ABB - AppNotes - 2.2 - 1HC0138868 EN AADocument8 pagesABB - AppNotes - 2.2 - 1HC0138868 EN AADeoudrafNo ratings yet
- PQ070XF02SZH: Features Outline DimensionsDocument4 pagesPQ070XF02SZH: Features Outline DimensionsJulio Cesar CastilloNo ratings yet