You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 18MUH2023 - Additional Campaign InformationDocument10 pages18MUH2023 - Additional Campaign InformationIbrahim SiddigNo ratings yet
- TOEFL IELTS Preparation by Abdulhadi Jfri PDFDocument22 pagesTOEFL IELTS Preparation by Abdulhadi Jfri PDFIbrahim SiddigNo ratings yet
- 91598662Document53 pages91598662Ibrahim SiddigNo ratings yet
- Who Unicef-Anaemiastatement PDFDocument2 pagesWho Unicef-Anaemiastatement PDFAsa Ngah AsyaNo ratings yet
- Who Unicef-Anaemiastatement PDFDocument2 pagesWho Unicef-Anaemiastatement PDFAsa Ngah AsyaNo ratings yet
- Tipus 3Document4 pagesTipus 3Gita AmaliaNo ratings yet
- Cell 02 PDFDocument13 pagesCell 02 PDFIbrahim SiddigNo ratings yet
- Official Guide PTEA Teacher NotesDocument249 pagesOfficial Guide PTEA Teacher NotesIqbal singh95% (20)
- What Are CellsHS PDFDocument12 pagesWhat Are CellsHS PDFIbrahim SiddigNo ratings yet
- CommonlaboratorytestsDocument54 pagesCommonlaboratorytestsIbrahim SiddigNo ratings yet
- Fact Sheet Iron Deficiency Anemia PDFDocument2 pagesFact Sheet Iron Deficiency Anemia PDFIbrahim SiddigNo ratings yet
- CommonlaboratorytestsDocument54 pagesCommonlaboratorytestsIbrahim SiddigNo ratings yet
- Tipus 3Document4 pagesTipus 3Gita AmaliaNo ratings yet
- Gram Staining Tips PDFDocument2 pagesGram Staining Tips PDFIbrahim SiddigNo ratings yet
- MLAB 2361 Clinical II Immunohematology Assignment Activity 6: ABO Discrepancies Case StudiesDocument7 pagesMLAB 2361 Clinical II Immunohematology Assignment Activity 6: ABO Discrepancies Case Studiespikachu0% (1)
- Bblab 8 - 9 DAT - Elution PDFDocument15 pagesBblab 8 - 9 DAT - Elution PDFIbrahim SiddigNo ratings yet
- Safari - Oct 10, 2018 at 6:25 PM PDFDocument1 pageSafari - Oct 10, 2018 at 6:25 PM PDFIbrahim SiddigNo ratings yet
- English4 PDFDocument2 pagesEnglish4 PDFIbrahim SiddigNo ratings yet
- Approach To NB With ThrombocytopeniaDocument7 pagesApproach To NB With ThrombocytopeniaSim M ChangNo ratings yet
- TOEFL IELTS Preparation by Abdulhadi Jfri PDFDocument22 pagesTOEFL IELTS Preparation by Abdulhadi Jfri PDFIbrahim SiddigNo ratings yet
- D0023989 PDFDocument7 pagesD0023989 PDFIbrahim SiddigNo ratings yet
- Elution Techniques for Identifying Blood AntibodiesDocument4 pagesElution Techniques for Identifying Blood AntibodiesIbrahim Siddig100% (1)
- English4 PDFDocument2 pagesEnglish4 PDFIbrahim SiddigNo ratings yet
- Aso (Antistreptolysin O) PDFDocument3 pagesAso (Antistreptolysin O) PDFIbrahim SiddigNo ratings yet
- Approach To NB With ThrombocytopeniaDocument7 pagesApproach To NB With ThrombocytopeniaSim M ChangNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Prenatal Management of AnencephalyDocument5 pagesPrenatal Management of AnencephalyarifsandroNo ratings yet
- Notes T3 C19Document6 pagesNotes T3 C19Jin Yee TanNo ratings yet
- Complications in PregnancyDocument81 pagesComplications in PregnancyTia TahniaNo ratings yet
- Medical Termination of PregnancyDocument8 pagesMedical Termination of PregnancyNikhil BijuNo ratings yet
- Down SyndromeDocument20 pagesDown SyndromeChristine Damayanti LumbangaolNo ratings yet
- Prenatal Screening and Diagnostic TestingDocument39 pagesPrenatal Screening and Diagnostic TestingakashNo ratings yet
- Gapuz Reviewer PDFDocument144 pagesGapuz Reviewer PDFAngela Gwynette OngjocoNo ratings yet
- Inborne Error of Amino Acid MetabolismDocument44 pagesInborne Error of Amino Acid MetabolismPrincewill SeiyefaNo ratings yet
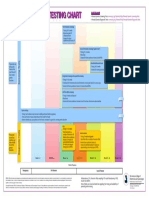
- Prenatal Genetic Testing ChartDocument1 pagePrenatal Genetic Testing ChartMorningDewNo ratings yet
- 3 - Structure of DNA, RNA, GenesDocument206 pages3 - Structure of DNA, RNA, GenesJustina VillageNo ratings yet
- Assessment of Fetal Growth and DevelopmentDocument30 pagesAssessment of Fetal Growth and DevelopmentWild Rose100% (2)
- Test AceptDocument16 pagesTest Acepttaty jatyNo ratings yet
- Genetic counseling and self testicular examDocument1 pageGenetic counseling and self testicular examRosemarie R. ReyesNo ratings yet
- 1141048.s41431 021 01026 1Document521 pages1141048.s41431 021 01026 1Laki AdziovskiNo ratings yet
- gtg60 Cervicalcerclage PDFDocument21 pagesgtg60 Cervicalcerclage PDFLijoeliyas100% (1)
- GeneticsDocument4 pagesGeneticsAngelica AycardoNo ratings yet
- 2) Training ManualDocument74 pages2) Training ManualSudhanshu PandeyNo ratings yet
- Nursing Practice II 2010Document16 pagesNursing Practice II 2010Anonymous NnC87DtzQNo ratings yet
- Prenatal Screening: Abes. Miranda. Samoranos. Tomas. RodrinDocument46 pagesPrenatal Screening: Abes. Miranda. Samoranos. Tomas. RodrinKim MyNo ratings yet
- Care of Mother and Child at Risk or With Problems - Acute and Chronic (Lecture)Document97 pagesCare of Mother and Child at Risk or With Problems - Acute and Chronic (Lecture)Mariah Alexis EncinaNo ratings yet
- Midwifery Evolution, Concepts and TheoriesDocument92 pagesMidwifery Evolution, Concepts and TheoriesRoxanne Jane S. Graycochea100% (1)
- CaseFiles FamilyMed Notes 5Document150 pagesCaseFiles FamilyMed Notes 5vesv86% (7)
- Jurnal Amniocentesis 4Document11 pagesJurnal Amniocentesis 4Wely JambiNo ratings yet
- Ob 3Document14 pagesOb 3Princess LotusNo ratings yet
- Amniocentesis - 5Document2 pagesAmniocentesis - 5HayatunNufusNamiraPasaribuNo ratings yet
- M Vanguardia-McnpDocument11 pagesM Vanguardia-Mcnpmark OrpillaNo ratings yet
- Biliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesDocument8 pagesBiliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesMaia Saivi OmegaNo ratings yet
- Prenatal Diagnosis PDFDocument747 pagesPrenatal Diagnosis PDFFlavius Yo0% (1)
- Identifying Clients at RiskDocument5 pagesIdentifying Clients at RiskMaryela Maceda GalozoNo ratings yet
- Risk Factors for High-Risk PregnanciesDocument8 pagesRisk Factors for High-Risk PregnanciesLRDR UCMEDNo ratings yet