You might also like
- Students' Book Audio Scripts: Gold Experience B2Document22 pagesStudents' Book Audio Scripts: Gold Experience B2Luanne33% (3)
- Ade 10Document28 pagesAde 10VenusBanquil100% (6)
- Conceptual Framework SampleDocument2 pagesConceptual Framework SampleReYa Buenaventura100% (1)
- The Physics of Zombies: Madore's Rules of Zombie Cohesion, Zombie Cells and Super Cells, Zombie Black Holes, Zombie Cell Stress-Fission and Zombie QuirksDocument19 pagesThe Physics of Zombies: Madore's Rules of Zombie Cohesion, Zombie Cells and Super Cells, Zombie Black Holes, Zombie Cell Stress-Fission and Zombie QuirksThe Madore Brothers100% (1)
- Effectofimplementingtrainingprogramfor PDFDocument13 pagesEffectofimplementingtrainingprogramfor PDFmochkurniawanNo ratings yet
- BJSTR MS Id 006919Document22 pagesBJSTR MS Id 006919Anz JoyNo ratings yet
- Vap 1Document6 pagesVap 1abdulNo ratings yet
- Prevention of VAP Use For Bundle Approach 10.1016@j.ajic.2016.04.237Document4 pagesPrevention of VAP Use For Bundle Approach 10.1016@j.ajic.2016.04.237sarintiNo ratings yet
- Impact Vap Bundle 2017Document6 pagesImpact Vap Bundle 2017Elisya KharuniawatiNo ratings yet
- Jurnal Kritis ICU Bundle Vap PneumoniaDocument6 pagesJurnal Kritis ICU Bundle Vap PneumoniaAdzkia PintaNo ratings yet
- البحث السادس PDFDocument32 pagesالبحث السادس PDFايمان عمرانNo ratings yet
- Vap 2Document8 pagesVap 2ahsan mohammedNo ratings yet
- Ventilator AssociatedDocument10 pagesVentilator Associatedtoothfairy2780No ratings yet
- VAP PreventionDocument8 pagesVAP PreventionJbl2328No ratings yet
- Ginny An Analysis of Knowledge Attitude and Practices Regarding Standard Precautions of Infection Control and Impact of Knowledge and Attitude of ICU Nurses On Self-Reported Practices of InfDocument7 pagesGinny An Analysis of Knowledge Attitude and Practices Regarding Standard Precautions of Infection Control and Impact of Knowledge and Attitude of ICU Nurses On Self-Reported Practices of InfMANISHA FMSNo ratings yet
- Improving Care of Patients On Non Invasive Ventilation (NIV) in The General WardsDocument7 pagesImproving Care of Patients On Non Invasive Ventilation (NIV) in The General WardsrefanNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka Annexure - Ii Proforma For Registration of Subject For DissertationDocument17 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka Annexure - Ii Proforma For Registration of Subject For DissertationyashramawatNo ratings yet
- Ventilator Associated Pneumonia in ChildrenDocument7 pagesVentilator Associated Pneumonia in ChildrendarlingcarvajalduqueNo ratings yet
- PneumoniaDocument12 pagesPneumoniaadolfrc9200No ratings yet
- A Care Bundle Approach For Prevention of Ventilator-AssociatedDocument7 pagesA Care Bundle Approach For Prevention of Ventilator-AssociatedRestu Kusuma NingtyasNo ratings yet
- VAP in ICU ReviewDocument8 pagesVAP in ICU ReviewAdam KurniaNo ratings yet
- HSR2 5 E649Document9 pagesHSR2 5 E649Samsul BahriNo ratings yet
- Prevention of Ventilator-Associated Pneumonia in Intensive Care Units: An International Online SurveyDocument8 pagesPrevention of Ventilator-Associated Pneumonia in Intensive Care Units: An International Online SurveymochkurniawanNo ratings yet
- Ventilator-Associated Pneumonia in Adults in Developing Countries: A Systematic ReviewDocument8 pagesVentilator-Associated Pneumonia in Adults in Developing Countries: A Systematic Reviewfrisca susdiNo ratings yet
- Compliance With Universal Precautions in A Medical Practice With A High Rate of HIV InfectionDocument6 pagesCompliance With Universal Precautions in A Medical Practice With A High Rate of HIV InfectionDirga Rasyidin LNo ratings yet
- 5 Nursing Strategies To Prevent Ventilator-Associated PneumoniaDocument5 pages5 Nursing Strategies To Prevent Ventilator-Associated PneumoniaPaulo Henrique SoaresNo ratings yet
- Ventilator Acquired Pneumonia - EditeDocument5 pagesVentilator Acquired Pneumonia - EditegggNo ratings yet
- MKV 046Document5 pagesMKV 046ardhenaNo ratings yet
- Ventilator-Associated Pneumonia Prevention: We Still Have A Long Way To Go!Document2 pagesVentilator-Associated Pneumonia Prevention: We Still Have A Long Way To Go!AzmachamberAzmacareNo ratings yet
- 747-Article Text-1365-1-10-20200430Document6 pages747-Article Text-1365-1-10-20200430Yogita DhurandharNo ratings yet
- New Guidelines For NeumoniaDocument7 pagesNew Guidelines For NeumoniacarlosNo ratings yet
- IndianJMedRes1396814-2632712 071847Document8 pagesIndianJMedRes1396814-2632712 071847christian hansNo ratings yet
- JCDR 10 SC06Document6 pagesJCDR 10 SC06YANNo ratings yet
- Research Paper On Ventilator Associated PneumoniaDocument8 pagesResearch Paper On Ventilator Associated PneumoniakwbfbzundNo ratings yet
- Compliance of Ventilator Associated Pneumonia Care Bundle by Staff Nurses in Critical Care UnitsDocument7 pagesCompliance of Ventilator Associated Pneumonia Care Bundle by Staff Nurses in Critical Care UnitsMalarvizhi SureshNo ratings yet
- Synopsis FormatDocument13 pagesSynopsis FormatYemane Fish83% (6)
- 3 DC 3Document8 pages3 DC 3astutikNo ratings yet
- Mcguckin 2004Document4 pagesMcguckin 2004noviaNo ratings yet
- Knowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalDocument4 pagesKnowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalAnonymous TzvMOnNo ratings yet
- Knowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalDocument4 pagesKnowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalAnonymous TzvMOnNo ratings yet
- Contributing Factors in Increasing Health Care Associated Infection (Hai's) in Phlebitis CasesDocument8 pagesContributing Factors in Increasing Health Care Associated Infection (Hai's) in Phlebitis CasesJenny MaulidyaNo ratings yet
- VAP 2 (Kejadian VAP Eropa)Document8 pagesVAP 2 (Kejadian VAP Eropa)tami ariyasraNo ratings yet
- Ventilator AssociatedDocument18 pagesVentilator AssociatedAndry Wahyudi AgusNo ratings yet
- Special Issue 1 3Document129 pagesSpecial Issue 1 3Amit PasiNo ratings yet
- 05 N017 2931Document13 pages05 N017 2931anju negalurNo ratings yet
- Neumonia Asosiada A VentiladorDocument11 pagesNeumonia Asosiada A VentiladorYnomata RusamellNo ratings yet
- 5867 19344 1 PBDocument10 pages5867 19344 1 PBjerayneNo ratings yet
- VAP PreventionDocument8 pagesVAP PreventionstarykNo ratings yet
- Tybd 20 138 PDFDocument10 pagesTybd 20 138 PDFElfina NataliaNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive Biologymnn164No ratings yet
- Effectiveness of Infection Control Standers On Practice Among Health Care Personnel Working in MCH Centers at Quena GovernorateDocument10 pagesEffectiveness of Infection Control Standers On Practice Among Health Care Personnel Working in MCH Centers at Quena GovernorateIOSRjournalNo ratings yet
- Pressure Ulcer PreventionDocument11 pagesPressure Ulcer PreventionChi ChangNo ratings yet
- Ventilator-Associated Pneumonia: Intensive Care Tutorial382Document6 pagesVentilator-Associated Pneumonia: Intensive Care Tutorial382mariskaNo ratings yet
- Preventing VAPDocument8 pagesPreventing VAPyankesNo ratings yet
- Park 2016Document6 pagesPark 2016Puspa Fitriyana DewiNo ratings yet
- Shea Vap 2014Document22 pagesShea Vap 2014Sally Mohy El-DinNo ratings yet
- Recommendations and Guidelines For The Treatment of Pneumonia in TaiwanDocument28 pagesRecommendations and Guidelines For The Treatment of Pneumonia in TaiwanMaymay DamayNo ratings yet
- Aislamientos Pacientes Con Fibrosis Quistica ICHE03Document48 pagesAislamientos Pacientes Con Fibrosis Quistica ICHE03haedugaNo ratings yet
- Strategies To Prevent Ventilator-Associated Pneumonia in Acute Care Hospitals: 2014 UpdateDocument23 pagesStrategies To Prevent Ventilator-Associated Pneumonia in Acute Care Hospitals: 2014 UpdateMarina MagalhãesNo ratings yet
- Cost Minimization of A Telehomecare Prog PDFDocument10 pagesCost Minimization of A Telehomecare Prog PDFRirin AptNo ratings yet
- 232 FullDocument14 pages232 FullCarlos OliveiraNo ratings yet
- Cambridge University Press, The Society For Healthcare Epidemiology of America Infection Control and Hospital EpidemiologyDocument23 pagesCambridge University Press, The Society For Healthcare Epidemiology of America Infection Control and Hospital EpidemiologyChaesar Abdil BarNo ratings yet
- Real Issues for COVID-19 Vaccine Immunization & Pregnancy, Breastfeeding MothersFrom EverandReal Issues for COVID-19 Vaccine Immunization & Pregnancy, Breastfeeding MothersNo ratings yet
- Blind Spots Video Discussion GuideDocument13 pagesBlind Spots Video Discussion GuidemochkurniawanNo ratings yet
- Promoting Self ManagementDocument11 pagesPromoting Self ManagementmochkurniawanNo ratings yet
- IMPACTDocument20 pagesIMPACTmochkurniawanNo ratings yet
- The Rise and Rise of Medtech in AsiaDocument12 pagesThe Rise and Rise of Medtech in AsiamochkurniawanNo ratings yet
- Session 01.5 Induced Hypothermia-The Nursing CareDocument13 pagesSession 01.5 Induced Hypothermia-The Nursing CaremochkurniawanNo ratings yet
- Opleidingsprogramma ENG - MarnixDocument81 pagesOpleidingsprogramma ENG - MarnixmochkurniawanNo ratings yet
- Endotracheal Tube ETT Insertion IntubationDocument3 pagesEndotracheal Tube ETT Insertion IntubationmochkurniawanNo ratings yet
- Neonatal Exposure To DEHPDocument24 pagesNeonatal Exposure To DEHPmochkurniawanNo ratings yet
- System: Total Solution For Value-Based Healthcare PurchasingDocument17 pagesSystem: Total Solution For Value-Based Healthcare PurchasingmochkurniawanNo ratings yet
- Medical Devices MPI Insights and Rankings 2017Document15 pagesMedical Devices MPI Insights and Rankings 2017mochkurniawanNo ratings yet
- Duodopa Intestinal Gel ENG SMPC - 09001be68007fc9a PDFDocument16 pagesDuodopa Intestinal Gel ENG SMPC - 09001be68007fc9a PDFmochkurniawanNo ratings yet
- Jan 2014 Nadine Nakazawa RNDocument70 pagesJan 2014 Nadine Nakazawa RNmochkurniawanNo ratings yet
- Endotracheal Tube Cuffs:: Design and FunctionDocument8 pagesEndotracheal Tube Cuffs:: Design and FunctionmochkurniawanNo ratings yet
- Indonesia Country Report June 2015Document23 pagesIndonesia Country Report June 2015mochkurniawanNo ratings yet
- Tracheostomy Management: 1. Overview and AnatomyDocument16 pagesTracheostomy Management: 1. Overview and AnatomymochkurniawanNo ratings yet
- Haemodialysis Access by Inferior Vena Cava Catheterisation: Cientific EttersDocument7 pagesHaemodialysis Access by Inferior Vena Cava Catheterisation: Cientific EttersmochkurniawanNo ratings yet
- V3 User Manual (MP-UI0V3) Rev2Document92 pagesV3 User Manual (MP-UI0V3) Rev2Gara PedrazaNo ratings yet
- Assignment - The Doctor Is in OrganizerDocument6 pagesAssignment - The Doctor Is in OrganizerAva MittoneNo ratings yet
- What Is The Role of An Infection Control NurseDocument7 pagesWhat Is The Role of An Infection Control NurseDENNIS N. MUÑOZNo ratings yet
- VirologyDocument9 pagesVirologyAnisha SarmaNo ratings yet
- Nurse Hooman-QuestionsDocument39 pagesNurse Hooman-QuestionsSophia Gella FredilesNo ratings yet
- Etiology of Acute Fever in COVID-19 Era SUS PDFDocument26 pagesEtiology of Acute Fever in COVID-19 Era SUS PDFIda Bagus Aditya NugrahaNo ratings yet
- CEFRADINEDocument2 pagesCEFRADINEAngelica Cassandra VillenaNo ratings yet
- NLE Test Taking StrategiesDocument31 pagesNLE Test Taking StrategiesAr-jay JubaneNo ratings yet
- Tuberculosis SlidesDocument18 pagesTuberculosis SlidesmedeviNo ratings yet
- Health Teaching Plan-St BarbaraDocument2 pagesHealth Teaching Plan-St BarbaraJune DumdumayaNo ratings yet
- Chapter 1: Diphtheria: I. Disease DescriptionDocument10 pagesChapter 1: Diphtheria: I. Disease DescriptionTina MorleyNo ratings yet
- Biosecurity For Successful PoultryDocument51 pagesBiosecurity For Successful PoultryGrowel Agrovet Private Limited.100% (1)
- And Important Diseases of Cattle: OmmonDocument6 pagesAnd Important Diseases of Cattle: OmmonANIL SEMWALNo ratings yet
- Dapsone Lyme DiseaseDocument53 pagesDapsone Lyme DiseasecemalsagmenNo ratings yet
- Basic Food Safety Handbook / Manual For Food Manufacturers, Processors and PackersDocument45 pagesBasic Food Safety Handbook / Manual For Food Manufacturers, Processors and PackersHarish100% (1)
- Union Christian College School of Health Sciences Microbiology and Parasitology Ignacio, Cheassy Jem B. BSN-1Document4 pagesUnion Christian College School of Health Sciences Microbiology and Parasitology Ignacio, Cheassy Jem B. BSN-1Kim CacanindinNo ratings yet
- HEALTH QUARTER II - Module 1Document27 pagesHEALTH QUARTER II - Module 1Clarence CoronacionNo ratings yet
- Total 15 10 15 LawDocument84 pagesTotal 15 10 15 LawMallikarjuna SharmaNo ratings yet
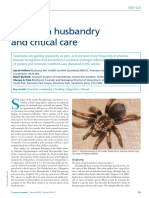
- Tarantula Husbandry and Critical Care Pellett2015Document8 pagesTarantula Husbandry and Critical Care Pellett2015jefferson luiz da silvaNo ratings yet
- Covid-19 Isolation Protocol - enDocument9 pagesCovid-19 Isolation Protocol - enRazvan FeodotNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanBtob meloNo ratings yet
- Cefazolin InjectionDocument15 pagesCefazolin InjectionYaleswari Hayu PertiwiNo ratings yet
- The Mathematics Behind ContagionDocument6 pagesThe Mathematics Behind Contagionkoonertex50% (2)
- How Much Have We Advanced?: English Pedagogical Module 2Document32 pagesHow Much Have We Advanced?: English Pedagogical Module 2MARIANA100% (2)
- PPP-BURNS 118slDocument30 pagesPPP-BURNS 118slCath BrilNo ratings yet
- Care and Support Needs of People Living With Hiv and AidsDocument13 pagesCare and Support Needs of People Living With Hiv and AidsSalihu MustaphaNo ratings yet
- IFU 1110004905 Fastep DEN-W23M(2滴buffer)(C-T1-T2线)CE 英文说明书 Polymed地址(彩色A4双面双胶)1张Document2 pagesIFU 1110004905 Fastep DEN-W23M(2滴buffer)(C-T1-T2线)CE 英文说明书 Polymed地址(彩色A4双面双胶)1张BPG ServiceNo ratings yet