You might also like
- The Poisoned Needle PDFDocument220 pagesThe Poisoned Needle PDFJulianna Ferrero75% (4)
- Vaccine Exemption FormsDocument4 pagesVaccine Exemption Formswqerq34234234233250% (6)
- Immunization in Children: Mary Beth F. Tanco, MD, FPPS Active Consultant Institute of Pediatrics and Child HealthDocument92 pagesImmunization in Children: Mary Beth F. Tanco, MD, FPPS Active Consultant Institute of Pediatrics and Child HealthPolychase Magaoay100% (1)
- Measles Virus Case StudyDocument12 pagesMeasles Virus Case StudyDan Dan ManaoisNo ratings yet
- MMR 2 Vaccine InsertDocument11 pagesMMR 2 Vaccine InsertJonNo ratings yet
- Immunization LectureDocument32 pagesImmunization LectureMekdes ZewdeNo ratings yet
- ImmunizationDocument40 pagesImmunizationJasmin PastoresNo ratings yet
- Vaccines PART 1Document57 pagesVaccines PART 1shahbaz100% (1)
- Multiple Choice QuestionsDocument7 pagesMultiple Choice QuestionsDr-Sanjay Singhania100% (3)
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDocument3 pagesMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
- Polio Eradication: Pulse Polio Programme: A.Prabhakaran M.SC (N), Tutor, VMACON, SalemDocument13 pagesPolio Eradication: Pulse Polio Programme: A.Prabhakaran M.SC (N), Tutor, VMACON, SalemPrabhakaran Aranganathan100% (3)
- Rabivax-S: Public Assessment ReportDocument8 pagesRabivax-S: Public Assessment ReportElsafani FaddiasyaNo ratings yet
- PriorixDocument23 pagesPriorixjaikp56No ratings yet
- Vet Pharm ReportDocument4 pagesVet Pharm ReportTusvendran PillaiNo ratings yet
- BCG Vaccine: Salk's Polio Vaccine "Inactivated Polio Vaccine" IPV InjectableDocument6 pagesBCG Vaccine: Salk's Polio Vaccine "Inactivated Polio Vaccine" IPV InjectableHandre PutraNo ratings yet
- Summary of Product Characteristics: Composition Per Dose (0.5 ML) : Component I ContainsDocument9 pagesSummary of Product Characteristics: Composition Per Dose (0.5 ML) : Component I ContainsGayathiri GovindarajuNo ratings yet
- COVAXIN Product InfoDocument7 pagesCOVAXIN Product InfoJoseph Raymund BautistaNo ratings yet
- IntracelluarPaper 1997Document4 pagesIntracelluarPaper 1997HJayNo ratings yet
- Immunizatuon ChissDocument51 pagesImmunizatuon ChissMariam AntonyNo ratings yet
- Vaccination: Passive ImmunityDocument12 pagesVaccination: Passive ImmunityuouoNo ratings yet
- Host Defenses To Infection: Tarek Amin DR Amira GamalDocument44 pagesHost Defenses To Infection: Tarek Amin DR Amira GamalWira SundokoNo ratings yet
- MMR VaccineDocument7 pagesMMR VaccineNaasah Saeed Hamdan Khameis AldhanhaniNo ratings yet
- M M Rvaxpro ProspectDocument57 pagesM M Rvaxpro ProspectNicoleta CiobotarNo ratings yet
- TbactDocument7 pagesTbactVinay KumarNo ratings yet
- ImmunizationDocument42 pagesImmunizationBahaa ShaabanNo ratings yet
- Summary Product Charecteristics: Rabies Vaccine For Human Use, (Vero-Cell) Freeze-Dried (Speeda Vaccine)Document4 pagesSummary Product Charecteristics: Rabies Vaccine For Human Use, (Vero-Cell) Freeze-Dried (Speeda Vaccine)Ryll Dela CruzNo ratings yet
- Rabies PreventionDocument40 pagesRabies PreventionPranab MajumdarNo ratings yet
- Infanrix Ipv Pi AuDocument16 pagesInfanrix Ipv Pi Ausamm1982No ratings yet
- Community WrittenDocument23 pagesCommunity WrittenImPrint CenterNo ratings yet
- Vaccines and Vaccination: Avian Immune SystemDocument3 pagesVaccines and Vaccination: Avian Immune SystemراجيرحمةربهNo ratings yet
- WHO - RabiesDocument5 pagesWHO - RabiesSatish Kumar DashNo ratings yet
- Abhay ArabDocument2 pagesAbhay ArabPrabin PaulNo ratings yet
- 184 VaccinationDocument14 pages184 VaccinationPrachi KharatmalNo ratings yet
- 13 Summary of Product Characteristics Labelling Package LeafletDocument20 pages13 Summary of Product Characteristics Labelling Package LeafletEnrique Carranza100% (1)
- Canine VaccinesDocument5 pagesCanine VaccinesSunil Mohan100% (1)
- Adult Immunization: Aduna, Naomi Bless S. Sy, Diana PDocument28 pagesAdult Immunization: Aduna, Naomi Bless S. Sy, Diana PNao AdunaNo ratings yet
- Pfizer BioNTech and Comirnaty Product Information For HCPDocument20 pagesPfizer BioNTech and Comirnaty Product Information For HCPJuan PaoloNo ratings yet
- Imovax Polio Larutan Injeksi 0,5 ML (Pre-Filled Syringe)Document1 pageImovax Polio Larutan Injeksi 0,5 ML (Pre-Filled Syringe)kemalahmadNo ratings yet
- Holding Company For Biological Products & Vaccines: DR: Mostafa Mohamady General Manager of VaccinesDocument65 pagesHolding Company For Biological Products & Vaccines: DR: Mostafa Mohamady General Manager of Vaccineskoky123456789No ratings yet
- Drugs That Affect The Immune System CompressedDocument176 pagesDrugs That Affect The Immune System CompressedSauda UddinNo ratings yet
- DrugDocument4 pagesDrugAugene ToribioNo ratings yet
- Tuberculosis 2Document13 pagesTuberculosis 2Asad MahmoodNo ratings yet
- T Bact OintmentDocument8 pagesT Bact OintmentAditya RajNo ratings yet
- EUA-Moderna Covid-19 Vaccine, Health Care Provider Fact Sheet, Approved Version Date 01/07/2021, BPOM, ID EREG10040912100174, EREG10040912100175Document15 pagesEUA-Moderna Covid-19 Vaccine, Health Care Provider Fact Sheet, Approved Version Date 01/07/2021, BPOM, ID EREG10040912100174, EREG10040912100175nicholas nickNo ratings yet
- Article 338Document6 pagesArticle 338danishNo ratings yet
- S 46 Mladenka TuberculosisDocument10 pagesS 46 Mladenka TuberculosisCarlo MaxiaNo ratings yet
- Antimycobacterial Drug StudyDocument5 pagesAntimycobacterial Drug StudyKathNo ratings yet
- ImmunizationDocument8 pagesImmunizationIsaac TanNo ratings yet
- Index PHPDocument11 pagesIndex PHPAndro IgnacioNo ratings yet
- Anti-Viral ChemotherapyDocument39 pagesAnti-Viral Chemotherapyjolan.freedomNo ratings yet
- Rabies and Intradermal Rabies Vaccination: Alan C. Jackson, MDDocument32 pagesRabies and Intradermal Rabies Vaccination: Alan C. Jackson, MDLemuel GuevarraNo ratings yet
- Vero RabDocument5 pagesVero RabMimiNo ratings yet
- Guideline For Animal Bite Management FAQ-2021Document10 pagesGuideline For Animal Bite Management FAQ-2021apurva pareekNo ratings yet
- Immunization in Public Health NutritionDocument30 pagesImmunization in Public Health NutritionUqba MishalNo ratings yet
- Tricat Trio InsertDocument2 pagesTricat Trio InsertSumanta MannaNo ratings yet
- Reg 174 Information For Uk Healthcare ProfessionalsDocument11 pagesReg 174 Information For Uk Healthcare ProfessionalsEDUARDO MachadoNo ratings yet
- Immunization LectureDocument37 pagesImmunization Lecturemy Lord JesusNo ratings yet
- CHN Immunization NotesDocument9 pagesCHN Immunization NotesJustin AncogNo ratings yet
- 0 BatchDocument34 pages0 BatchRahul MehtaNo ratings yet
- Expanded Program On ImmunizationDocument15 pagesExpanded Program On ImmunizationReygie MarsadaNo ratings yet
- Information For Healthcare ProfessionalsDocument10 pagesInformation For Healthcare ProfessionalsgaliaNo ratings yet
- Synflorix: Product MonographDocument40 pagesSynflorix: Product Monographabba,drNo ratings yet
- Covid Vaccines - Part IDocument5 pagesCovid Vaccines - Part IAdrian AdinaNo ratings yet
- COV IgMDocument40 pagesCOV IgMguido escobar moyaNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- Vaccination: How Millions of Lives Have Been Saved - Perhaps YoursFrom EverandVaccination: How Millions of Lives Have Been Saved - Perhaps YoursNo ratings yet
- Meila1 - Espiritu - Aimee CristineDocument5 pagesMeila1 - Espiritu - Aimee CristineCharles AnthonyNo ratings yet
- Meil Act2 Grp#1 Espiritu, AimeecristineDocument1 pageMeil Act2 Grp#1 Espiritu, AimeecristineCharles AnthonyNo ratings yet
- Espiritu, Charles Anthony C.Document8 pagesEspiritu, Charles Anthony C.Charles AnthonyNo ratings yet
- Stacking of VaccinesDocument1 pageStacking of VaccinesCharles AnthonyNo ratings yet
- CLIL Unit 5 BiologyDocument2 pagesCLIL Unit 5 BiologyDaniela PeterováNo ratings yet
- CertificateDocument1 pageCertificatechinni kumarNo ratings yet
- Vaccine Manufacturers IndiaDocument6 pagesVaccine Manufacturers Indiayash shahNo ratings yet
- 1 Student Summary Sheet 2022Document2 pages1 Student Summary Sheet 2022williamchung1222No ratings yet
- Vaccine Prices in LebanonDocument14 pagesVaccine Prices in LebanonJamilNo ratings yet
- Vaccination Certificate CornejoDocument1 pageVaccination Certificate CornejoGelo JvrNo ratings yet
- EPIDocument5 pagesEPIMarquenash Cruz ViñasNo ratings yet
- KA VaccinationDocument9 pagesKA VaccinationVictor GaborNo ratings yet
- WHO Measles Outbreak Training Module 4Document32 pagesWHO Measles Outbreak Training Module 4JalalNo ratings yet
- Hongkong Boostrix Diftetkok Boostrix - Polio Engerix - B Hyper-Tet Infanrix-Ipv+Hib MMR Ii VarivaxDocument7 pagesHongkong Boostrix Diftetkok Boostrix - Polio Engerix - B Hyper-Tet Infanrix-Ipv+Hib MMR Ii Varivaxapotik medicareNo ratings yet
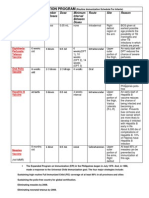
- NO. Diseases Vaccine Type Doses Dosage Site Brand Names: Route Interval Age Given (First Dose)Document3 pagesNO. Diseases Vaccine Type Doses Dosage Site Brand Names: Route Interval Age Given (First Dose)Breezy ReveloNo ratings yet
- Name: Background Information:: Part 1: PBS Nova-Making VaccinesDocument3 pagesName: Background Information:: Part 1: PBS Nova-Making VaccinesNoelNo ratings yet
- Disease Summary of Common SymptomsDocument1 pageDisease Summary of Common SymptomsJeffrey CohenNo ratings yet
- Whooping Cough Pertussis PDFDocument2 pagesWhooping Cough Pertussis PDFFikri RamadhanNo ratings yet
- Immunization FormsDocument6 pagesImmunization FormsNadya IrsalinaNo ratings yet
- Yellow Fever Vaccination CertificateDocument1 pageYellow Fever Vaccination Certificatekishore kumarNo ratings yet
- Doh ProgramsDocument14 pagesDoh ProgramsSweetyfe GabatanNo ratings yet
- Profiling Infant Olivia & FranzDocument2 pagesProfiling Infant Olivia & FranzShane Frances SaborridoNo ratings yet
- Global Manual Revised 12102015Document124 pagesGlobal Manual Revised 12102015Ishak Abdul GafarNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsBhavani reddyNo ratings yet
- Bonza Fake NewsDocument8 pagesBonza Fake NewsAJ Louise IbanezNo ratings yet
- 2022 To 2024 Workplan National Advisory Committee On Immunization (NACI) - Canada - CaDocument9 pages2022 To 2024 Workplan National Advisory Committee On Immunization (NACI) - Canada - CakelvinkinergyNo ratings yet
- Module 5Document14 pagesModule 5Riyan WahyudoNo ratings yet
- March, To It Now Being The Vast Majority of Our Sequenced CasesDocument6 pagesMarch, To It Now Being The Vast Majority of Our Sequenced Cases01 LudviaNo ratings yet