You might also like
- NDocument85 pagesNralichramNo ratings yet
- Guias ESC para Insuficiencia Cardiaca CronicaDocument128 pagesGuias ESC para Insuficiencia Cardiaca CronicaKarla HernandezNo ratings yet
- Afriwardi: Bagian Fisiologi Fakultas Kedokteran Universitas Andalas PadangDocument35 pagesAfriwardi: Bagian Fisiologi Fakultas Kedokteran Universitas Andalas PadangralichramNo ratings yet
- Afriwardi: Bagian Fisiologi Fakultas Kedokteran Universitas Andalas PadangDocument35 pagesAfriwardi: Bagian Fisiologi Fakultas Kedokteran Universitas Andalas PadangralichramNo ratings yet
- SHHDocument50 pagesSHHralichramNo ratings yet
- 1.5.3.1 - Perkembangan Janin Intrauterin Dan Gangguan Yang Mungkin TimbulDocument54 pages1.5.3.1 - Perkembangan Janin Intrauterin Dan Gangguan Yang Mungkin TimbulMuhammad Fatkhi100% (1)
- 1.5.3.1 - Perkembangan Janin Intrauterin Dan Gangguan Yang Mungkin TimbulDocument54 pages1.5.3.1 - Perkembangan Janin Intrauterin Dan Gangguan Yang Mungkin TimbulMuhammad Fatkhi100% (1)
- ULYA UTI FASRINI, DR., M.BiomedDocument47 pagesULYA UTI FASRINI, DR., M.BiomedralichramNo ratings yet
- Analysis of The Food Record: BreakfastDocument3 pagesAnalysis of The Food Record: BreakfastralichramNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- AnatomyDocument265 pagesAnatomyOsama100% (3)
- Brain Understanding Interpretation of CT and MriDocument67 pagesBrain Understanding Interpretation of CT and MriStefan StefNo ratings yet
- Lusensi Periapikal Panoramik-BF-1 Juli 2020Document19 pagesLusensi Periapikal Panoramik-BF-1 Juli 2020Roberto HutapeaNo ratings yet
- BiologyDocument80 pagesBiologyAmp100% (6)
- Chapter 1 Lesson 2 Training Exercises That Increase Mobility EDITED 1 1Document19 pagesChapter 1 Lesson 2 Training Exercises That Increase Mobility EDITED 1 1Dawn JoyNo ratings yet
- .Tf. Iken. : T. JunuznizDocument11 pages.Tf. Iken. : T. JunuznizCristopher Jimenez OrozcoNo ratings yet
- BloodDocument24 pagesBloodapi-310193189No ratings yet
- Transport in HumansDocument1 pageTransport in Humansapi-3714421100% (1)
- Medical AstrologyDocument2 pagesMedical Astrologyabhi16No ratings yet
- Acute Phase ProteinsDocument3 pagesAcute Phase ProteinswaihenyaNo ratings yet
- Legal MedicLegal MediciineDocument1 pageLegal MedicLegal MediciineJuan S. EnricoNo ratings yet
- SP 21Document1 pageSP 21ray72roNo ratings yet
- Blood Cell Morphology TutorialDocument176 pagesBlood Cell Morphology TutorialCharles Jebb Belonio JuanitasNo ratings yet
- 11 Biology Notes ch22 Chemical Coordination and Integration PDFDocument6 pages11 Biology Notes ch22 Chemical Coordination and Integration PDFAarav VarshneyNo ratings yet
- Malpresentations and MalpositionsDocument14 pagesMalpresentations and MalpositionsAsteway MesfinNo ratings yet
- Gi PhysiologyDocument21 pagesGi PhysiologyNoreen Orro BernalNo ratings yet
- Immunoglobulin A (Iga)Document1 pageImmunoglobulin A (Iga)Lione MilanNo ratings yet
- CARDIOVASCULAR ANATOMY AND PHYSIOLOGY TestDocument6 pagesCARDIOVASCULAR ANATOMY AND PHYSIOLOGY TestDevilsnareNo ratings yet
- Wound Healing: Ziv Peled, M.DDocument8 pagesWound Healing: Ziv Peled, M.Dapi-26007957No ratings yet
- Autopsy Who Peforms The Autopsy?: Aut-+ Opsis Sight, Appearance - More at OpticDocument5 pagesAutopsy Who Peforms The Autopsy?: Aut-+ Opsis Sight, Appearance - More at Opticmiguel gaquitNo ratings yet
- Life Flows Because of You..Document40 pagesLife Flows Because of You..Klemen JamnikNo ratings yet
- BIO201L Lab 5 TissuesDocument12 pagesBIO201L Lab 5 Tissuesmyra Thiong'oNo ratings yet
- Case Study of A Patient With Ischemic CardiomyopathyDocument33 pagesCase Study of A Patient With Ischemic Cardiomyopathyromeo rivera80% (5)
- Lab. Act. #7 - Nervous TissueDocument6 pagesLab. Act. #7 - Nervous TissueDan OdviarNo ratings yet
- Basic Human Anatomy AND Physiology: Emmanuel Z. Pagala M.DDocument136 pagesBasic Human Anatomy AND Physiology: Emmanuel Z. Pagala M.DDARLENE SUETOSNo ratings yet
- Quiz 3Document3 pagesQuiz 3Vannie MonderoNo ratings yet
- Lecture2 GranulopoiesisDocument9 pagesLecture2 GranulopoiesisAfifa Prima GittaNo ratings yet
- Test Yourself MCQ andDocument2 pagesTest Yourself MCQ andSanjeewa de AlwisNo ratings yet
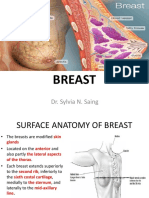
- Breast: Dr. Sylvia N. SaingDocument26 pagesBreast: Dr. Sylvia N. SaingRichard 151289100% (1)
- DPP - Anatomy of Flowering PlantsDocument10 pagesDPP - Anatomy of Flowering PlantsRitika GochhaitNo ratings yet