You might also like
- Individual Health Application FormDocument2 pagesIndividual Health Application FormRalph Wamae0% (1)
- FormatDocument3 pagesFormatchiragNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsMaria JessaNo ratings yet
- Medical ForDocument8 pagesMedical FormarandugebraNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsJaj EscNo ratings yet
- The Candidate Must Complete Section A of The Form and Submit It To The Med Al Fficer at T e Time of ExaminationDocument4 pagesThe Candidate Must Complete Section A of The Form and Submit It To The Med Al Fficer at T e Time of ExaminationJabdi LobahNo ratings yet
- Medical Declaration Form: Family History of The ApplicantDocument3 pagesMedical Declaration Form: Family History of The ApplicantJae WaiNo ratings yet
- ICICI Prudential Life Insurance Co LTD - Attachment - 6Document2 pagesICICI Prudential Life Insurance Co LTD - Attachment - 6vermalabNo ratings yet
- General Questions NO YESDocument5 pagesGeneral Questions NO YESChristian James PACILANNo ratings yet
- Medical Examination Form - Juvenile: Part 1: Statement To The Medical ExaminerDocument4 pagesMedical Examination Form - Juvenile: Part 1: Statement To The Medical ExaminerMohd Rafie HashimNo ratings yet
- Medical Examination Form: Part 1: Statement To The Medical ExaminerDocument4 pagesMedical Examination Form: Part 1: Statement To The Medical ExaminerMohd Rafie HashimNo ratings yet
- Liver Disease Questionnaire For Proposed Insured/OwnerDocument2 pagesLiver Disease Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Medical English Presentation2Document17 pagesMedical English Presentation2N KNo ratings yet
- Declaration Good Health Form PDFDocument2 pagesDeclaration Good Health Form PDFMurali SiddarthNo ratings yet
- Medical Examination For Teaching PermitDocument4 pagesMedical Examination For Teaching PermitEllina JamesNo ratings yet
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- Medical Examination - Wee Chye KimDocument4 pagesMedical Examination - Wee Chye KimGeminiCrescentNo ratings yet
- 3 Health PDFDocument2 pages3 Health PDFAndré DomanskiNo ratings yet
- DiabetesDocument2 pagesDiabetessudhanshugst123No ratings yet
- Medical Examination - Chan Way CheuDocument4 pagesMedical Examination - Chan Way CheuGeminiCrescentNo ratings yet
- Elem Sec Health CardsDocument17 pagesElem Sec Health CardsMary Grace CalipesNo ratings yet
- Health Questionnaire TemplateDocument2 pagesHealth Questionnaire TemplateBaxwal AxmedNo ratings yet
- MFC PDFDocument5 pagesMFC PDFdipmipNo ratings yet
- 3 Health PDFDocument2 pages3 Health PDFpierlisurNo ratings yet
- Raksha New Pre-Authorization FormDocument1 pageRaksha New Pre-Authorization Formjigerpanchal0% (1)
- Medical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsDocument4 pagesMedical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsAnnisa DiendaNo ratings yet
- LP K EnglishDocument3 pagesLP K Englishivander sudarnotoNo ratings yet
- New-Patient-Forms-All-2020 GoodDocument8 pagesNew-Patient-Forms-All-2020 GoodCheryl WanNo ratings yet
- Health Questionnaire For Online Version - Retail Revised VersionDocument4 pagesHealth Questionnaire For Online Version - Retail Revised VersionTrushaba B. JadejaNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- Libro ComplementarioDocument155 pagesLibro ComplementarioKowe xDNo ratings yet
- Declaration of Good Heath: Ddmmy YYYDocument2 pagesDeclaration of Good Heath: Ddmmy YYYindu chauhanNo ratings yet
- DR - Allam Books 2014 General CardiologyDocument113 pagesDR - Allam Books 2014 General Cardiologymuchalaith100% (1)
- DR Langford1Document8 pagesDR Langford1Spencer JacksonNo ratings yet
- Diabetes20171011 112709Document2 pagesDiabetes20171011 112709ROYNo ratings yet
- Individual Health Proposal FormDocument1 pageIndividual Health Proposal Formwaleed majeedNo ratings yet
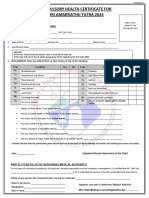
- Annexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Document1 pageAnnexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Shrasti SoniNo ratings yet
- GPMRDocument5 pagesGPMRwisdom hameloNo ratings yet
- HD FormatDocument4 pagesHD FormatSaravana KumarNo ratings yet
- English CHCDocument1 pageEnglish CHCBhupi AgrawalNo ratings yet
- Lia-Pre-Authorisation-Form - 20220117 2Document3 pagesLia-Pre-Authorisation-Form - 20220117 2starspigotNo ratings yet
- Form Pemfis Dokter (Subcon Saipem)Document3 pagesForm Pemfis Dokter (Subcon Saipem)Humas PemasaranNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificatelekacaNo ratings yet
- GHS Health Declaration Form PDFDocument2 pagesGHS Health Declaration Form PDFFattah AfawNo ratings yet
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNo ratings yet
- Your Health PlanDocument9 pagesYour Health PlanMaggie FornaroNo ratings yet
- Multitable New Patient FormDocument8 pagesMultitable New Patient Forme-MedTools100% (9)
- Health Certificate To Work in Confined SpaceDocument6 pagesHealth Certificate To Work in Confined SpacenmmarhelNo ratings yet
- Medical Fitness Self DeclarationDocument2 pagesMedical Fitness Self Declarationrajeshbabu.palamettaNo ratings yet
- IELTS Academic Training Reading Practice Test #10. An Example Exam for You to Practise in Your Spare TimeFrom EverandIELTS Academic Training Reading Practice Test #10. An Example Exam for You to Practise in Your Spare TimeRating: 5 out of 5 stars5/5 (1)
- Certificate of HealthDocument2 pagesCertificate of HealthmohamedydNo ratings yet
- Report of Medical History: PhoneDocument3 pagesReport of Medical History: PhoneLeroy Jethro Gibbs NicosiaNo ratings yet
- Medical FormDocument3 pagesMedical FormPrincess Mae DesaculaNo ratings yet
- Consent Form - Pfizer-Biontech Covid-19 VaccineDocument2 pagesConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaNo ratings yet
- Juvenile - FMR - PDF For MINORDocument2 pagesJuvenile - FMR - PDF For MINORHemant JhaNo ratings yet
- Respiratory Disorders Questionnaire Including Asthma, Bronchitis, Emphysema, EtcDocument3 pagesRespiratory Disorders Questionnaire Including Asthma, Bronchitis, Emphysema, EtcSunil TyagiNo ratings yet
- Adult NP PaperworkDocument5 pagesAdult NP Paperworksomethingelse913No ratings yet
- Vsim - Edited Clinical WorksheetsDocument8 pagesVsim - Edited Clinical WorksheetsTedra FloydNo ratings yet
- Medical ReportDocument3 pagesMedical ReportSachitra Nirman MalwatteNo ratings yet
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- Royal Australian College of General Practitioners AMC Bridging CoursesDocument6 pagesRoyal Australian College of General Practitioners AMC Bridging CoursescarthingsNo ratings yet
- Advanced Practice Nursing in The United StatesDocument6 pagesAdvanced Practice Nursing in The United StatesrhinoNo ratings yet
- Torri. Multicultural Social Policy and Communityparticipation in Health - New Opportunities Andchallenges For Indigenous People PDFDocument23 pagesTorri. Multicultural Social Policy and Communityparticipation in Health - New Opportunities Andchallenges For Indigenous People PDFanon_731469955No ratings yet
- ICTM 111 (Report)Document17 pagesICTM 111 (Report)David James RotamulaNo ratings yet
- MMJ PhysicianCertificationFormDocument1 pageMMJ PhysicianCertificationFormBrian GoguenNo ratings yet
- MANIPULATIONDocument336 pagesMANIPULATIONGhica Costin100% (1)
- The Concept of Family Medicine in KosovoDocument25 pagesThe Concept of Family Medicine in KosovoLleshi DukagjinNo ratings yet
- Nugraha Mauluddin CV UpdateDocument4 pagesNugraha Mauluddin CV UpdateNugraha MauluddinNo ratings yet
- Patient Rights & ResponsibilitiesDocument4 pagesPatient Rights & ResponsibilitiesCarlos Miguel AndalNo ratings yet
- Essentials of Internal MedicineDocument832 pagesEssentials of Internal MedicineEmanuelMC100% (75)
- Illustrated Book of Pediatrics 2ndDocument975 pagesIllustrated Book of Pediatrics 2ndCarla Tapia Norambuena100% (2)
- Foundations For Assisting in Home Care 1520419723Document349 pagesFoundations For Assisting in Home Care 1520419723amasrurNo ratings yet
- SEPDocument6 pagesSEPapoc lordNo ratings yet
- Notice: Registration Revocations, Restrictions, Denials, Reinstatements: Oviedo Discount PharmacyDocument7 pagesNotice: Registration Revocations, Restrictions, Denials, Reinstatements: Oviedo Discount PharmacyJustia.com100% (1)
- Telemedicine A Need For Ethical and Legal Guidelines in South AfricaDocument5 pagesTelemedicine A Need For Ethical and Legal Guidelines in South AfricaAna MironNo ratings yet
- Manila and or Michaelmar Shipping ServicesDocument2 pagesManila and or Michaelmar Shipping ServicesMariam PetillaNo ratings yet
- J&J Quest Isb CynosureDocument7 pagesJ&J Quest Isb CynosureHimanshu BhatiaNo ratings yet
- Doi&rig&pra&gui&et&med&4th PDFDocument441 pagesDoi&rig&pra&gui&et&med&4th PDFSajid Rahman75% (4)
- The Practice of Medicine: Atty. Judy Anne Yuki Yulo, RN, MDDocument31 pagesThe Practice of Medicine: Atty. Judy Anne Yuki Yulo, RN, MDarellano lawschool100% (2)
- Effect of COVID-19 On Doctor-Patient Relationship: Original Research ArticleDocument7 pagesEffect of COVID-19 On Doctor-Patient Relationship: Original Research ArticleMarlisa LionoNo ratings yet
- Bhore Committee 1946Document32 pagesBhore Committee 1946saritatelma100% (1)
- Pharmaceutical Benefits Under State Medical Assistance Programs, 1989Document359 pagesPharmaceutical Benefits Under State Medical Assistance Programs, 1989National Pharmaceutical Council100% (4)
- Activity 2 FinalDocument19 pagesActivity 2 FinalJunaiza Adrayan MariNo ratings yet
- APIs and API MarketplaceDocument14 pagesAPIs and API MarketplaceSiddharth SethNo ratings yet
- HospitalsDocument29 pagesHospitalsAkash PawarNo ratings yet
- Pharmacy and Therapeutics CommitteeDocument28 pagesPharmacy and Therapeutics CommitteeHaseeba KhanNo ratings yet
- Physicians Committee For Responsible MedicineDocument10 pagesPhysicians Committee For Responsible MedicinePeter M. HeimlichNo ratings yet
- dt0919 EzineDocument74 pagesdt0919 EzineOskiNo ratings yet
- Advanced Philosophical Theory Foundations in Nursing: By: Marie John C. Jardiolin RNDocument30 pagesAdvanced Philosophical Theory Foundations in Nursing: By: Marie John C. Jardiolin RNmyronmjj100% (3)
- Status Maritime Versus Doctolero-Case DigestDocument1 pageStatus Maritime Versus Doctolero-Case DigestAnskee TejamNo ratings yet