You might also like
- 27 30 Month Visit ReportDocument2 pages27 30 Month Visit ReportOlga CîrsteaNo ratings yet
- Neonatal ChartDocument2 pagesNeonatal ChartJohn SelvamNo ratings yet
- (PEDIA) History ChecklistDocument7 pages(PEDIA) History ChecklistReggie Lyn BaricanNo ratings yet
- Updated Health FormsDocument3 pagesUpdated Health Formskevin9392No ratings yet
- Physician's Well Child Exam Form 6 MonthsDocument3 pagesPhysician's Well Child Exam Form 6 MonthsJanelleNo ratings yet
- Clinic HMV Guidelines 2018Document6 pagesClinic HMV Guidelines 2018Ross HagenNo ratings yet
- O&G History TakingDocument5 pagesO&G History TakingAishwarya SivakumarNo ratings yet
- Physician's Well Child Exam Form 4 MonthsDocument3 pagesPhysician's Well Child Exam Form 4 MonthsJanelleNo ratings yet
- MDWF 2040 Carter 13Document6 pagesMDWF 2040 Carter 13api-366292665No ratings yet
- Rellance: Laikshmlovaa PDST, Dasanaputa Holl Tanna LnreDocument16 pagesRellance: Laikshmlovaa PDST, Dasanaputa Holl Tanna LnreSanthosh RNo ratings yet
- 2 Months Well Child CheckDocument3 pages2 Months Well Child CheckJanelleNo ratings yet
- PHA Individual Health Profile & Assessment Form As of Oct.09, 2017Document8 pagesPHA Individual Health Profile & Assessment Form As of Oct.09, 2017Eden VblagasyNo ratings yet
- Health Assessment Record: State of Connecticut Department of EducationDocument3 pagesHealth Assessment Record: State of Connecticut Department of EducationChettamilsNo ratings yet
- Wa0002.Document5 pagesWa0002.s8903082No ratings yet
- CDR Report Form: National Fatality Review Case Reporting SystemDocument24 pagesCDR Report Form: National Fatality Review Case Reporting SystemJesse M. MassieNo ratings yet
- Abdominal Pain With Uterine CrampsDocument8 pagesAbdominal Pain With Uterine CrampsMohamadhizam M. PangcatanNo ratings yet
- Anc AssessmentDocument6 pagesAnc AssessmentRakshitha D PNo ratings yet
- Ante Natal Assessment FormatDocument4 pagesAnte Natal Assessment FormatJames BondNo ratings yet
- Child Health Assessment PDFDocument1 pageChild Health Assessment PDFসু কন্যাNo ratings yet
- Pediatric Assessment ToolDocument3 pagesPediatric Assessment ToolKrystel BatinoNo ratings yet
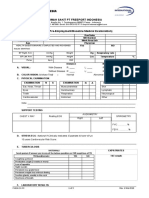
- Pre Employment Medical Examination Form - RS - pt.FIDocument3 pagesPre Employment Medical Examination Form - RS - pt.FINooB GAMING100% (1)
- Obs Gyn ClerkingDocument5 pagesObs Gyn ClerkingdonaldooiNo ratings yet
- Neny Guidelines 2022 Prenatal PerinatalDocument10 pagesNeny Guidelines 2022 Prenatal Perinatalzainab al-aliNo ratings yet
- Rle CompreDocument132 pagesRle CompremayangernszNo ratings yet
- One Month Well Child Visit: History Physical ExaminationDocument2 pagesOne Month Well Child Visit: History Physical ExaminationMae Rose GillespieNo ratings yet
- Employment Registration Requirements For Cdpap: You Will Need The Following DocumentationDocument2 pagesEmployment Registration Requirements For Cdpap: You Will Need The Following DocumentationAkbar ShakoorNo ratings yet
- H&P Cheat SheetDocument3 pagesH&P Cheat SheetWilliam YangNo ratings yet
- Pregnancy Wheel: Evaluate at ANC VisitDocument2 pagesPregnancy Wheel: Evaluate at ANC VisitChristille Grace Basa MuchuelasNo ratings yet
- Profiling F SHORTDocument8 pagesProfiling F SHORTjonjon arrabiNo ratings yet
- Pediatric NursingDocument3 pagesPediatric NursingAllisson BeckersNo ratings yet
- I. Identifying Info: Vii. Birth HX AntenatalDocument5 pagesI. Identifying Info: Vii. Birth HX AntenatalSean Dominique Cruz MaghinayNo ratings yet
- SA04 Medical Examination Report PDFDocument4 pagesSA04 Medical Examination Report PDFSOU FEI Ang0% (1)
- Endorsement SheetDocument2 pagesEndorsement SheetdaliaNo ratings yet
- Postpartum Care Plan New BornDocument10 pagesPostpartum Care Plan New BornUche Edwards-ShahidNo ratings yet
- Physical Form 2018Document2 pagesPhysical Form 2018api-247134277No ratings yet
- Obstetric CaseDocument6 pagesObstetric CaseRanjitha ArulNo ratings yet
- VuvvlesheeDocument3 pagesVuvvlesheeNEIL GUTIERREZNo ratings yet
- 2nd Preceptorials FinalDocument14 pages2nd Preceptorials FinalGabriel MillaNo ratings yet
- Child Health BookDocument24 pagesChild Health BookSylvester NyarkoNo ratings yet
- Patient Worksheet - Postpartum 1-PatientDocument1 pagePatient Worksheet - Postpartum 1-PatientJerry G100% (1)
- Department of Pediatrics-3Document8 pagesDepartment of Pediatrics-3harie82No ratings yet
- E/M Audit Form: Chart #Document2 pagesE/M Audit Form: Chart #Anthony El HageNo ratings yet
- 1 Pedia BundleDocument7 pages1 Pedia BundleJescel-Anne Janea MagatNo ratings yet
- CHARGE Association ChecklistDocument4 pagesCHARGE Association ChecklistSuzanneNo ratings yet
- General Information:: Sta. Ana Hospital Department of Rehabilitation Medicine Physical Therapy SectionDocument13 pagesGeneral Information:: Sta. Ana Hospital Department of Rehabilitation Medicine Physical Therapy SectionOlenFuerteNo ratings yet
- Subjective Data Objective Data: Alert Oriented Level of Comprehension Concentration MemoryDocument3 pagesSubjective Data Objective Data: Alert Oriented Level of Comprehension Concentration MemoryclrssNo ratings yet
- Comments On Regulating LDTDocument2 pagesComments On Regulating LDTfdablogNo ratings yet
- UK Biologics Checklist May 2014Document2 pagesUK Biologics Checklist May 2014Dr Sneha's Skin and Allergy Clinic IndiaNo ratings yet
- Medical and Physical Exam FormDocument2 pagesMedical and Physical Exam FormkhohannahfaithNo ratings yet
- NEW PE FORM Bangayan Vhynee SDocument4 pagesNEW PE FORM Bangayan Vhynee SVhynee BangayanNo ratings yet
- Flowchart Management of Neonatal JaundiceDocument2 pagesFlowchart Management of Neonatal JaundiceSalvera ArnoldyNo ratings yet
- NBZ Qobgy V01 092020Document3 pagesNBZ Qobgy V01 092020chong xue erNo ratings yet
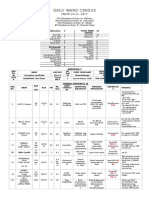
- DAILY CENSUS 10-11 Mar 2017Document4 pagesDAILY CENSUS 10-11 Mar 2017Zandra Lyn AlundayNo ratings yet
- Resident Review Form FCG FinalDocument1 pageResident Review Form FCG Finalbernie hewsonNo ratings yet
- Pediatric NursingDocument6 pagesPediatric NursingAllisson BeckersNo ratings yet
- Cerebral PalsyDocument27 pagesCerebral PalsyJohn Paul Parungao CrisostomoNo ratings yet
- School District Health Assessment FormDocument2 pagesSchool District Health Assessment FormAnuvratha NarayananNo ratings yet
- Nursing Department: Bicol University Tabaco Campus Tabaco CityDocument3 pagesNursing Department: Bicol University Tabaco Campus Tabaco CityCelline Isabelle ReyesNo ratings yet
- FINAL Cervical CADocument14 pagesFINAL Cervical CAroselo alagaseNo ratings yet
- 2023 EAACI - Guidelines - Diagnosis - IgE-mediated - Food - AllergyDocument56 pages2023 EAACI - Guidelines - Diagnosis - IgE-mediated - Food - AllergyOlga CîrsteaNo ratings yet
- 2022 Risk Assessment Tool To Identify Children Aged 2-59 Months Risk For Death From CAPDocument12 pages2022 Risk Assessment Tool To Identify Children Aged 2-59 Months Risk For Death From CAPOlga CîrsteaNo ratings yet
- 2020 Assessment of Missed Opportunities For Vaccination in Burkina Faso Using The WHO Revised MOV StrategyDocument21 pages2020 Assessment of Missed Opportunities For Vaccination in Burkina Faso Using The WHO Revised MOV StrategyOlga CîrsteaNo ratings yet
- 2023 Identifying Risk of Death in Children Hospitalized With Community-Acquired PneumoniaDocument9 pages2023 Identifying Risk of Death in Children Hospitalized With Community-Acquired PneumoniaOlga CîrsteaNo ratings yet
- 2022 A Retrospective Chart Review of Pediatric Complicated Community-Acquired PneumoniaDocument20 pages2022 A Retrospective Chart Review of Pediatric Complicated Community-Acquired PneumoniaOlga CîrsteaNo ratings yet
- Сhronic pancreatitis: Lykhatska G.VDocument42 pagesСhronic pancreatitis: Lykhatska G.VOlga CîrsteaNo ratings yet
- Stein R Et Al Paediatric Infections EUR UROL 67 2015 546 558 14826Document13 pagesStein R Et Al Paediatric Infections EUR UROL 67 2015 546 558 14826Olga CîrsteaNo ratings yet
- Child Health Check-UpHBDocument92 pagesChild Health Check-UpHBOlga CîrsteaNo ratings yet
- Necrotizing Pneumonia - An Emerging Problem in ChildrenDocument19 pagesNecrotizing Pneumonia - An Emerging Problem in ChildrenOlga CîrsteaNo ratings yet
- Connecting Home Visiting and The Medical Home SlidesDocument60 pagesConnecting Home Visiting and The Medical Home SlidesOlga CîrsteaNo ratings yet
- Health Professionals Guide To Coping at NightDocument19 pagesHealth Professionals Guide To Coping at NightOlga CîrsteaNo ratings yet
- Conversations For The Health Visiting Team: Key PointsDocument2 pagesConversations For The Health Visiting Team: Key PointsOlga CîrsteaNo ratings yet
- Guidelines EngDocument96 pagesGuidelines EngOlga CîrsteaNo ratings yet
- Visual System Assessment in Infants, Children, and Young Adults by PediatriciansDocument5 pagesVisual System Assessment in Infants, Children, and Young Adults by PediatriciansOlga CîrsteaNo ratings yet
- !!! Home and Community Visiting For Children, Young People and Families 2016 AustraliaDocument16 pages!!! Home and Community Visiting For Children, Young People and Families 2016 AustraliaOlga CîrsteaNo ratings yet
- Health Care-Acquired Viral Respiratory DiseasesDocument18 pagesHealth Care-Acquired Viral Respiratory DiseasesOlga CîrsteaNo ratings yet
- ERS Handbook of Paediatric Respiratory Medicine - E. Eber, F MidullaDocument750 pagesERS Handbook of Paediatric Respiratory Medicine - E. Eber, F MidullaOlga CîrsteaNo ratings yet
- LabCorpTestingProtocol6 08Document4 pagesLabCorpTestingProtocol6 08Olga CîrsteaNo ratings yet
- Systematic Review - Effective Management Strategies For Lactose Intolerance 2010Document11 pagesSystematic Review - Effective Management Strategies For Lactose Intolerance 2010Olga CîrsteaNo ratings yet
- Statistics and Data CollectionDocument11 pagesStatistics and Data CollectionRichimon LicerioNo ratings yet
- Sistem Informasi Pencatatan Data Pelanggan Pada Telkomsel Grapari Banda AcehDocument6 pagesSistem Informasi Pencatatan Data Pelanggan Pada Telkomsel Grapari Banda AcehJurnal JTIK (Jurnal Teknologi Informasi dan Komunikasi)No ratings yet
- The Brain in Your Pocket Evidence - That - SDocument8 pagesThe Brain in Your Pocket Evidence - That - Sanwaarft123No ratings yet
- Checklist-Telephone - Mobile ExpenseDocument2 pagesChecklist-Telephone - Mobile ExpenseMichelle Domanacal UrsabiaNo ratings yet
- 35.ravi Gupta Writs (CLE)Document22 pages35.ravi Gupta Writs (CLE)Ravi GuptaNo ratings yet
- Hitachi Zx330 3 Series Hydraulic ExcavatorDocument15 pagesHitachi Zx330 3 Series Hydraulic ExcavatorAgung ArdhanaNo ratings yet
- Chapter 3 ContDocument12 pagesChapter 3 ContVenus Frias-AntonioNo ratings yet
- How To Make Papaya SoapDocument10 pagesHow To Make Papaya SoapEmz GamboaNo ratings yet
- Distortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaDocument11 pagesDistortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaHibernoSlavNo ratings yet
- Bang Thong Ke Phep NamDocument16 pagesBang Thong Ke Phep NamTiến Tươi TỉnhNo ratings yet
- Install NotesDocument6 pagesInstall NotesSchweinsteiger NguyễnNo ratings yet
- Chapter 1Document38 pagesChapter 1Kurt dela Torre100% (1)
- Individual Ability in SoftwareDocument9 pagesIndividual Ability in Softwaredhana0809100% (4)
- SSP 861603 - EN - Tire Pressure Monitoring SystemsDocument42 pagesSSP 861603 - EN - Tire Pressure Monitoring Systemsa.diedrichsNo ratings yet
- 2020 LBG q1 Ims Pillar 3 DisclosuresDocument8 pages2020 LBG q1 Ims Pillar 3 DisclosuressaxobobNo ratings yet
- Enga10 Speaking Test3Document2 pagesEnga10 Speaking Test3luana serraNo ratings yet
- Resume For Singapore Spass Civil EngineerDocument8 pagesResume For Singapore Spass Civil EngineerArul SD100% (1)
- Title Toolbox 1 ADocument2 pagesTitle Toolbox 1 AGet LiveHelpNo ratings yet
- Agmt - Spa Schedule HDocument20 pagesAgmt - Spa Schedule Hapi-340431954No ratings yet
- Sticker BookDocument66 pagesSticker BookIvan SutlovicNo ratings yet
- The Lion and The Boar Story EnglishDocument2 pagesThe Lion and The Boar Story EnglishKemal AmarullahNo ratings yet
- Openstack Deployment Ops Guide PDFDocument197 pagesOpenstack Deployment Ops Guide PDFBinank PatelNo ratings yet
- Title: Speech of Corazon C. Aquino Before The US Congress: 3 Hours)Document3 pagesTitle: Speech of Corazon C. Aquino Before The US Congress: 3 Hours)Verna TrillanaNo ratings yet
- OCTOBER 2016: Nur Amira Nadia Binti Azizi 2018404898 BA1185FDocument4 pagesOCTOBER 2016: Nur Amira Nadia Binti Azizi 2018404898 BA1185FNur Amira NadiaNo ratings yet
- Jazz Guitar Soloing Etude F Blues 3 To 9 ArpsDocument1 pageJazz Guitar Soloing Etude F Blues 3 To 9 ArpsLeonardoPiresNo ratings yet
- Sample Paper For Professional Ethics in Accounting and FinanceDocument6 pagesSample Paper For Professional Ethics in Accounting and FinanceWinnieOngNo ratings yet
- Method Statement Free Download: How To Do Installation of Suspended False CeilingsDocument3 pagesMethod Statement Free Download: How To Do Installation of Suspended False Ceilingsmozartjr22100% (1)
- Deferred Tax QsDocument4 pagesDeferred Tax QsDaood AbdullahNo ratings yet
- Enzyme Kinetics Principles and MethodsDocument268 pagesEnzyme Kinetics Principles and MethodsCarlos Carinelli100% (4)
- WWW Creativebloq Com Infographic Tools 2131971Document20 pagesWWW Creativebloq Com Infographic Tools 2131971Martin_Arrieta_GNo ratings yet