You might also like
- 472 1466 1 PB - 2Document6 pages472 1466 1 PB - 2Nazlia LarashitaNo ratings yet
- Advantage of Modified MRI Protocol For HDocument148 pagesAdvantage of Modified MRI Protocol For HasasakopNo ratings yet
- Epilepsy Comorbidity in Children With Cerebral Palsy 2472 0895 1000e117Document2 pagesEpilepsy Comorbidity in Children With Cerebral Palsy 2472 0895 1000e117Ocha24 TupamahuNo ratings yet
- Epilepsy in Children With Cerebral PalsyDocument6 pagesEpilepsy in Children With Cerebral PalsyTiara Renita LestariNo ratings yet
- Etiology and Outcome of Non Traumatic Coma in Children Admitted To Pediatric Intensive Care UnitDocument6 pagesEtiology and Outcome of Non Traumatic Coma in Children Admitted To Pediatric Intensive Care Unitcohimif914No ratings yet
- 1456 FullDocument7 pages1456 Fulldrmanishmahajan79No ratings yet
- Hipo Glice MiaDocument7 pagesHipo Glice MiaRosita Aguirre FloresNo ratings yet
- Risk FactorDocument2 pagesRisk FactorHamtaroHedwigNo ratings yet
- Clinical Outcomes of Neonatal Hypoxic Ischemic Encephalopathy Evaluated With Diffusion-Weighted Magnetic Resonance ImagingDocument6 pagesClinical Outcomes of Neonatal Hypoxic Ischemic Encephalopathy Evaluated With Diffusion-Weighted Magnetic Resonance ImagingDrsandy SandyNo ratings yet
- Congenital Hypotonia Is There An AlgorithmDocument4 pagesCongenital Hypotonia Is There An AlgorithmEvelyn HerreraNo ratings yet
- 1 s2.0 S0920121123000244 MainDocument9 pages1 s2.0 S0920121123000244 MainilonaskorinNo ratings yet
- Posterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsDocument7 pagesPosterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsJasper CubiasNo ratings yet
- Acute Disseminated Encephalomyelitis in Chicken Pox: Case ReportDocument2 pagesAcute Disseminated Encephalomyelitis in Chicken Pox: Case ReportCorneliu VladNo ratings yet
- ArticleDocument7 pagesArticleLinda RahayueNo ratings yet
- Motor and Sensory Dysfunctions in Children With Mental Retardation and EpilepsyDocument8 pagesMotor and Sensory Dysfunctions in Children With Mental Retardation and EpilepsyNhu ChristianyNo ratings yet
- Ijcn 7 001Document5 pagesIjcn 7 001Adinda Ratna PuspitaNo ratings yet
- 1 s2.0 S1059131115000035 MainDocument4 pages1 s2.0 S1059131115000035 MainRebeca HernandezNo ratings yet
- Heterotopia PV GruposDocument12 pagesHeterotopia PV GruposJuan D. HoyosNo ratings yet
- Archneuro 55 199 PDFDocument6 pagesArchneuro 55 199 PDFAdam MochtarNo ratings yet
- Bab I Pendahuluan: Persistent Vegetative State in Head InjuryDocument17 pagesBab I Pendahuluan: Persistent Vegetative State in Head InjuryNindy Novela RitongaNo ratings yet
- Abstract Booklet 2010Document50 pagesAbstract Booklet 2010Danijela VukicevicNo ratings yet
- TPNE Niños y AdolescentesDocument7 pagesTPNE Niños y AdolescentesNelson AlvarengaNo ratings yet
- Agyria-PachygyriaDocument6 pagesAgyria-PachygyriaNeha OberoiNo ratings yet
- 2014 Does EEG Contribute To Examining Children With ADHDDocument3 pages2014 Does EEG Contribute To Examining Children With ADHDPiotr BuczkowiczNo ratings yet
- Quiz EpilepsiaDocument5 pagesQuiz EpilepsiaLisselotte CarolinaNo ratings yet
- Periodic Lateralized Epileptiform Discharges: Aetiology and Association With EEG SeizuresDocument2 pagesPeriodic Lateralized Epileptiform Discharges: Aetiology and Association With EEG SeizuresChandra DarusmanNo ratings yet
- Burns 2008Document12 pagesBurns 2008Monesh-BhaskaranNo ratings yet
- Acute Disseminated Encephalomyelitis in Children: ObjectiveDocument9 pagesAcute Disseminated Encephalomyelitis in Children: ObjectivecarlaNo ratings yet
- Clinical Characteristics and Prognostic Factors of Children With Anti-N-Methyl-D-Aspartate Receptor EncephalitisDocument9 pagesClinical Characteristics and Prognostic Factors of Children With Anti-N-Methyl-D-Aspartate Receptor EncephalitisSara IsabelNo ratings yet
- Visual Evoked Potentials in Guillain-Barré Syndrome: MethodsDocument6 pagesVisual Evoked Potentials in Guillain-Barré Syndrome: MethodsYulianti PurnamasariNo ratings yet
- Autism and EpilepsyDocument5 pagesAutism and Epilepsyclarajimena25No ratings yet
- An EEG Study of The Neurodevelopmental H PDFDocument1 pageAn EEG Study of The Neurodevelopmental H PDFemilio9fernandez9gatNo ratings yet
- Childhood Anti-NMDA Receptor Encephalitis: Original ArticleDocument6 pagesChildhood Anti-NMDA Receptor Encephalitis: Original Articlehemir1902No ratings yet
- An Extended Way To Predict Neonatal Hypoxic Ischemic EncephalopathyDocument2 pagesAn Extended Way To Predict Neonatal Hypoxic Ischemic EncephalopathyMarissa B LukbanNo ratings yet
- Appi Neuropsych 18010005Document6 pagesAppi Neuropsych 18010005sarahNo ratings yet
- Etiology, Clinical Profile and Outcome of First Episode of Seizure in ChildrenDocument5 pagesEtiology, Clinical Profile and Outcome of First Episode of Seizure in ChildrenUlan SariNo ratings yet
- Seizure-Related Factors and Non-Verbal Intelligence in Children With Epilepsy A Population-Based Study From Western NorwayDocument9 pagesSeizure-Related Factors and Non-Verbal Intelligence in Children With Epilepsy A Population-Based Study From Western NorwayIsta Fatimah Kurnia RahmiNo ratings yet
- Untitled 4Document1 pageUntitled 4Giga HasabiNo ratings yet
- Clinico-Epidemiological ProfileDocument7 pagesClinico-Epidemiological ProfilephylienNo ratings yet
- Encef Peds PDFDocument11 pagesEncef Peds PDFNicolas TovarNo ratings yet
- Ref Ref 2Document5 pagesRef Ref 2melly adityaNo ratings yet
- Epileptic Encephalopathies SYNGAP1Document7 pagesEpileptic Encephalopathies SYNGAP1Saya OtonashiNo ratings yet
- By I. Bradinova, S. Shopova and E. SimeonovDocument20 pagesBy I. Bradinova, S. Shopova and E. SimeonovNoor Hijriyati ShofianaNo ratings yet
- Anti-N-methyl-D-aspartate Receptor (NMDAR) Encephalitis: A Series of Ten Cases From A University Hospital in MalaysiaDocument6 pagesAnti-N-methyl-D-aspartate Receptor (NMDAR) Encephalitis: A Series of Ten Cases From A University Hospital in MalaysiaAbhishek KayalNo ratings yet
- Infectious Dan Autoantibody Associated EncephalitisDocument13 pagesInfectious Dan Autoantibody Associated EncephalitisAyudiah ParamitaNo ratings yet
- Discoveries 08 110Document19 pagesDiscoveries 08 110Riki AntoNo ratings yet
- Acn3 8 138Document15 pagesAcn3 8 138ilonaskorinNo ratings yet
- E731 FullDocument11 pagesE731 FullLia NadaNo ratings yet
- Thesis On Neonatal SeizuresDocument4 pagesThesis On Neonatal SeizuresSomeoneWriteMyPaperForMeWichitaFalls100% (2)
- Utility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFDocument26 pagesUtility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFMaverick 18No ratings yet
- 10 11648 J CNN 20200402 12Document4 pages10 11648 J CNN 20200402 12inunNo ratings yet
- Epilepsy and Electroencephalogram Evolution in YWHAG Gene MutationDocument8 pagesEpilepsy and Electroencephalogram Evolution in YWHAG Gene MutationGiselle Costa Daniel HonoratoNo ratings yet
- Parinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronDocument6 pagesParinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronJessica HerreraNo ratings yet
- Psychogenic Non-Epileptic Seizures: ArticleDocument3 pagesPsychogenic Non-Epileptic Seizures: ArticleNico NicoNo ratings yet
- Enterovirus D68Document43 pagesEnterovirus D68wawa chenNo ratings yet
- Mukhopadhyay 2010Document4 pagesMukhopadhyay 2010Sayak ChowdhuryNo ratings yet
- Clinical and Etiological Profile of Acute Febrile Encephalopathy in Eastern NepalDocument3 pagesClinical and Etiological Profile of Acute Febrile Encephalopathy in Eastern NepalNeha OberoiNo ratings yet
- Staring Spells V Epilepsy PDFDocument4 pagesStaring Spells V Epilepsy PDFverdantlawNo ratings yet
- Terapi S.EDocument5 pagesTerapi S.EnafamaulidinaNo ratings yet
- Neonatal Seizures: Current Management and Future ChallengesFrom EverandNeonatal Seizures: Current Management and Future ChallengesLakshmi NagarajanRating: 4 out of 5 stars4/5 (2)
- Hasil Olah Data Dari SPSS Bu AriDocument4 pagesHasil Olah Data Dari SPSS Bu AriSeptianaNo ratings yet
- Garuda 1406490Document17 pagesGaruda 1406490SeptianaNo ratings yet
- Jadwal Kamis 21 Jan 2021 Jam 09.00 - 12.00Document3 pagesJadwal Kamis 21 Jan 2021 Jam 09.00 - 12.00SeptianaNo ratings yet
- Terdaftar Di Bank: # NIM Nama BiayaDocument3 pagesTerdaftar Di Bank: # NIM Nama BiayaSeptianaNo ratings yet
- Europeanjournalofpaediatricneurology S SDocument1 pageEuropeanjournalofpaediatricneurology S SSeptianaNo ratings yet
- The Quality of ChildrenDocument5 pagesThe Quality of ChildrenSeptianaNo ratings yet
- Neonatal Jaundice and Increased Risk ofDocument8 pagesNeonatal Jaundice and Increased Risk ofSeptianaNo ratings yet
- Associations Between Parental Psychological Well-Being and PDFDocument6 pagesAssociations Between Parental Psychological Well-Being and PDFSeptianaNo ratings yet
- Social Competence Low Birth WeightDocument6 pagesSocial Competence Low Birth WeightSeptianaNo ratings yet
- Associations Between Parental Psychological Well-Being andDocument8 pagesAssociations Between Parental Psychological Well-Being andSeptianaNo ratings yet
- Associations Between Parental Psychological Well-Being and PDFDocument6 pagesAssociations Between Parental Psychological Well-Being and PDFSeptianaNo ratings yet
- Extensive Reading - AVK44CDocument42 pagesExtensive Reading - AVK44CNinh Nhat Thao Vy K189No ratings yet
- Chordoma Current Concepts Management and Future DirectionsDocument8 pagesChordoma Current Concepts Management and Future DirectionsChristian AdeNo ratings yet
- IE ScoliosisDocument6 pagesIE ScoliosisVanessa Yvonne GurtizaNo ratings yet
- Biology Form 4 Chapter 5 Cell DivisionDocument7 pagesBiology Form 4 Chapter 5 Cell Divisiongelgaban67% (3)
- Neurological Complications in Lumbar Spine SurgeryDocument9 pagesNeurological Complications in Lumbar Spine SurgeryMimi SyakilaNo ratings yet
- Manual On Lab Referral For Outbreak Response-Draft 2Document95 pagesManual On Lab Referral For Outbreak Response-Draft 2kbl27No ratings yet
- Risk Factors For CKDDocument2 pagesRisk Factors For CKDgigolo13No ratings yet
- Neurotrac Tens: Operators ManualDocument28 pagesNeurotrac Tens: Operators ManualShane NaidooNo ratings yet
- Eosinophilic DermatosesDocument15 pagesEosinophilic DermatosesmikelNo ratings yet
- Nursing Care Plan: Student's Name: ID: Course Name: SettingDocument3 pagesNursing Care Plan: Student's Name: ID: Course Name: SettingnjoodNo ratings yet
- Virology MCQDocument62 pagesVirology MCQGazi Shahinur Akter ShampaNo ratings yet
- Darvocet N Drug CardDocument1 pageDarvocet N Drug CardSheri490No ratings yet
- Mosquito Net SpecificationDocument12 pagesMosquito Net SpecificationManoj KumarNo ratings yet
- Cardiocare 2000 Operation ManualDocument61 pagesCardiocare 2000 Operation ManualDokter MoezNo ratings yet
- Guideline Who Preeclampsia-EclampsiaDocument48 pagesGuideline Who Preeclampsia-EclampsiaRahmania Noor AdibaNo ratings yet
- Lapsus Dr. DodyDocument36 pagesLapsus Dr. DodyPriscilla Christina NatanNo ratings yet
- QUES2-1 Stir Not The World's DoomDocument49 pagesQUES2-1 Stir Not The World's DoomNicholas LouieNo ratings yet
- Ashtanga Yoga I and II Complete OCR (Finereader - IsTA SettingsDocument192 pagesAshtanga Yoga I and II Complete OCR (Finereader - IsTA SettingsAndreea Bertea0% (1)
- Warming Center New HavenDocument3 pagesWarming Center New HavenHelen BennettNo ratings yet
- Effect of Dragon Fruit On Lipid ProfileDocument2 pagesEffect of Dragon Fruit On Lipid ProfileElindah Ayunin ArrumNo ratings yet
- Inheritance and Selective Breeding QsDocument27 pagesInheritance and Selective Breeding QspartinpoutsamouNo ratings yet
- Impaction in Dairy Animals: Ashwani KumarDocument6 pagesImpaction in Dairy Animals: Ashwani KumarGiriNo ratings yet
- Heart - Anatomy and FunctionDocument13 pagesHeart - Anatomy and FunctionAlok KumarNo ratings yet
- Riddor: Health and Safety Advice For StonemasonsDocument12 pagesRiddor: Health and Safety Advice For StonemasonsMohammed IlliasuddinNo ratings yet
- Hiperpigmentasi Paska InflamasiDocument18 pagesHiperpigmentasi Paska InflamasiNoventyChristiNo ratings yet
- Export Act 1963Document27 pagesExport Act 1963Anonymous OPix6Tyk5INo ratings yet
- Effectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyaDocument10 pagesEffectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyainventionjournalsNo ratings yet
- Immunology MCQ BY: Dr. AlgassimDocument4 pagesImmunology MCQ BY: Dr. AlgassimmohamedNo ratings yet
- Sabouraud Dextrose BrothDocument2 pagesSabouraud Dextrose Brothrdn2111No ratings yet
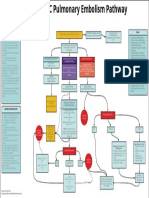
- EMCrit Lae Pulmonary FlowDocument1 pageEMCrit Lae Pulmonary FlowhmsptrNo ratings yet