You might also like
- Cetin 2016Document10 pagesCetin 2016Della Puspita SariNo ratings yet
- Serum C Reactive Protein in The Prediction of Cardiovascular Diseases: Overview of The Latest Clinical Studies and Public Health PracticeDocument18 pagesSerum C Reactive Protein in The Prediction of Cardiovascular Diseases: Overview of The Latest Clinical Studies and Public Health PracticeVirginia ZagorniiNo ratings yet
- A Comparative Study of Platelet Indices in Acute Coronary SyndromeDocument4 pagesA Comparative Study of Platelet Indices in Acute Coronary SyndromeMarcellia AngelinaNo ratings yet
- Vascular Health, Systemic Inflammation and Progressive Reduction in Kidney Function Clinical Determinants and Impact On Cardiovascular OutcomesDocument7 pagesVascular Health, Systemic Inflammation and Progressive Reduction in Kidney Function Clinical Determinants and Impact On Cardiovascular OutcomesBibi MorenoNo ratings yet
- Biomarker Discovery in Cardio-Oncology.Document8 pagesBiomarker Discovery in Cardio-Oncology.Ștefan SpînuNo ratings yet
- PIIS246802492301536XDocument13 pagesPIIS246802492301536XjosedegibesNo ratings yet
- Nef DiscRAADocument11 pagesNef DiscRAAGabriela PachecoNo ratings yet
- Endothelial Dysfunction and Cardiovascular Risk in Lupus Nephritis New Roles For Old PlayersDocument30 pagesEndothelial Dysfunction and Cardiovascular Risk in Lupus Nephritis New Roles For Old PlayersSilvia PeresNo ratings yet
- tjp0592 3969Document15 pagestjp0592 3969Sathit KrtNo ratings yet
- 1 s2.0 S0422763817300055 MainDocument20 pages1 s2.0 S0422763817300055 MainNicoleta Popa-FoteaNo ratings yet
- Journal of Nephropathology: Contrast-Induced Nephropathy A Literature ReviewDocument6 pagesJournal of Nephropathology: Contrast-Induced Nephropathy A Literature ReviewayupurnamasariiNo ratings yet
- AtheroesclerosisDocument18 pagesAtheroesclerosisGabriel IdkNo ratings yet
- 16Document8 pages16AlamgirNo ratings yet
- CVONSDocument10 pagesCVONSrahmansetiawanajaNo ratings yet
- Pathophysiology and Pharmacotherapy of AtherosclerosisDocument7 pagesPathophysiology and Pharmacotherapy of AtherosclerosisSandeep PooniaNo ratings yet
- 25rakshitha EtalDocument8 pages25rakshitha EtaleditorijmrhsNo ratings yet
- CRP 3 PDFDocument7 pagesCRP 3 PDFAdarsiya JayakumarNo ratings yet
- Synoptic Reporting of EchocardiographyDocument11 pagesSynoptic Reporting of Echocardiography林昌恩No ratings yet
- Jurnal 1Document10 pagesJurnal 1fitri juliantiNo ratings yet
- Neutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventDocument9 pagesNeutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventYohanes FirmansyahNo ratings yet
- Higado Graso No Alcoholico y Niveles de PCRDocument6 pagesHigado Graso No Alcoholico y Niveles de PCRperuliz19No ratings yet
- Primer: AtherosclerosisDocument18 pagesPrimer: AtherosclerosisLeonardoCampanelliNo ratings yet
- Sfad 101Document14 pagesSfad 101el himawatiNo ratings yet
- Cardiorenal Syndrome: SciencedirectDocument10 pagesCardiorenal Syndrome: SciencedirectDwiFitriaAnggrainiNo ratings yet
- C Reaktive ProteinDocument4 pagesC Reaktive Proteinsinggih2008No ratings yet
- ESC Heart Failure - 2022 - Di Lisi - The New HFA ICOS Risk Assessment Tool To Identify Patients With Chronic MyeloidDocument6 pagesESC Heart Failure - 2022 - Di Lisi - The New HFA ICOS Risk Assessment Tool To Identify Patients With Chronic MyeloidLissaberti AmaliahNo ratings yet
- High Sensitivity C-Reactive ProteinDocument100 pagesHigh Sensitivity C-Reactive ProteinFast ComposersNo ratings yet
- ECG Scoring For The Evaluation of Therapy Naive Cancer Patients To Predict CardiotoxicityDocument11 pagesECG Scoring For The Evaluation of Therapy Naive Cancer Patients To Predict CardiotoxicityjuanpbagurNo ratings yet
- Nihms 971496Document23 pagesNihms 971496prk prkNo ratings yet
- Xu 2020Document29 pagesXu 2020Anastasia ChristineNo ratings yet
- 2021 Special Care in Dentistry Detection of Calcified AtheromasDocument6 pages2021 Special Care in Dentistry Detection of Calcified AtheromasNATALIA SILVA ANDRADENo ratings yet
- Grant2014 PDFDocument10 pagesGrant2014 PDFRalucaNo ratings yet
- Study of CRP and LDL-HDL Ratio in AMIDocument11 pagesStudy of CRP and LDL-HDL Ratio in AMISanjeevNo ratings yet
- JCM 10 00524Document14 pagesJCM 10 00524PhysiologyNo ratings yet
- Central Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort StudyDocument10 pagesCentral Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort Studyady suciptoNo ratings yet
- ImplicationsofHemostasisDisordersinPatientswith CriticalLimbIschemia-AnIn-DepthComparisonof SelectedFactorsDocument9 pagesImplicationsofHemostasisDisordersinPatientswith CriticalLimbIschemia-AnIn-DepthComparisonof SelectedFactorsMarcellia AngelinaNo ratings yet
- MPV SciDocument6 pagesMPV SciMikael AngelooNo ratings yet
- HSCRP Level-0,5Document10 pagesHSCRP Level-0,5Nova SipahutarNo ratings yet
- La Tensión Longitudinal Global Del Ventrículo Izquierdo Predice Presiones Cardíacas Elevadas y Malos Resultados ClínicosDocument13 pagesLa Tensión Longitudinal Global Del Ventrículo Izquierdo Predice Presiones Cardíacas Elevadas y Malos Resultados ClínicosJorge FajardoNo ratings yet
- Coronary Artery Disease Literature ReviewDocument4 pagesCoronary Artery Disease Literature Reviewaflsvwoeu100% (1)
- Data Mining Technique Identifies Potential Target Proteins P - 2020 - InformaticDocument7 pagesData Mining Technique Identifies Potential Target Proteins P - 2020 - InformaticAntonio DominguezNo ratings yet
- BiomarkerDocument6 pagesBiomarkerpriyaNo ratings yet
- The Prognostic Role of The Spleen in Heart FailureDocument11 pagesThe Prognostic Role of The Spleen in Heart FailurePedro MatosNo ratings yet
- Is It Possible To Prevent Chemotherapy-InducedDocument16 pagesIs It Possible To Prevent Chemotherapy-InducedJulita MelisaNo ratings yet
- 2023_Mesenchymal Stem Cell Therapy in Acute Intracerebral Hemorrhage_ A Dose-Escalation Safety and Tolerability TrialDocument11 pages2023_Mesenchymal Stem Cell Therapy in Acute Intracerebral Hemorrhage_ A Dose-Escalation Safety and Tolerability TrialOlga Manco GuzmánNo ratings yet
- Clinchem 2013 203778 FullDocument9 pagesClinchem 2013 203778 FullHarnadi WonogiriNo ratings yet
- Non Coding RNAs Cancer Treatment and Cardiotoxicity A Triad of New HopeDocument31 pagesNon Coding RNAs Cancer Treatment and Cardiotoxicity A Triad of New Hopewedikaf807No ratings yet
- Estimation of Cardiovascular DiseaseDocument14 pagesEstimation of Cardiovascular DiseaseShree Narayan YadavNo ratings yet
- Pparγ Gene and AtherosclerosisDocument9 pagesPparγ Gene and AtherosclerosisisaNo ratings yet
- BE Project10Document18 pagesBE Project10Sanjana PolNo ratings yet
- Circulating Microvesicles in Convalescent Ischemic Stroke Patients: A Contributor To High-On-Treatment Residual Platelet Reactivity?Document7 pagesCirculating Microvesicles in Convalescent Ischemic Stroke Patients: A Contributor To High-On-Treatment Residual Platelet Reactivity?Nasdı BabayevaNo ratings yet
- Christersson2022 Article ScreeningForBiomarkersAssociatDocument11 pagesChristersson2022 Article ScreeningForBiomarkersAssociatS FznsNo ratings yet
- Research Article Plasma Fibrin Clot Properties As Determinants of Bleeding Time in Human Subjects: Association With Histidine-Rich GlycoproteinDocument11 pagesResearch Article Plasma Fibrin Clot Properties As Determinants of Bleeding Time in Human Subjects: Association With Histidine-Rich GlycoproteinAyu Nabila Kusuma PradanaNo ratings yet
- Prevenção de IraDocument21 pagesPrevenção de IrajoseNo ratings yet
- s40560-017-0223-2Document10 pagess40560-017-0223-2ERICK KUMAR BAUTISTA GOMEZNo ratings yet
- CKD Risk FactorsDocument14 pagesCKD Risk FactorsSrinivas PingaliNo ratings yet
- SANTORINIDocument7 pagesSANTORINIjoseNo ratings yet
- The Mean Platelet Volume On Admission Predicts Unfavorable Stroke Outcomes in Patients Treated With IV ThrombolysisDocument12 pagesThe Mean Platelet Volume On Admission Predicts Unfavorable Stroke Outcomes in Patients Treated With IV ThrombolysisstjackNo ratings yet
- Microcirculation in Cardiovascular DiseasesFrom EverandMicrocirculation in Cardiovascular DiseasesEnrico Agabiti-RoseiNo ratings yet
- Schramm 2014Document9 pagesSchramm 2014bayuwinotoNo ratings yet
- The Impact of Early Outcome Events On The Effect of Tranexamic Acid in Post-Partum Haemorrhage - An Exploratory Subgroup Analysis of The WOMAN TrialDocument9 pagesThe Impact of Early Outcome Events On The Effect of Tranexamic Acid in Post-Partum Haemorrhage - An Exploratory Subgroup Analysis of The WOMAN TrialbayuwinotoNo ratings yet
- Dilatation and Curettage Increases The Risk of Subsequent Preterm BirthDocument13 pagesDilatation and Curettage Increases The Risk of Subsequent Preterm BirthbayuwinotoNo ratings yet
- Sainz Et Al. A Simple Predictive Model For Complicated Operative Vaginal DeliveriesDocument12 pagesSainz Et Al. A Simple Predictive Model For Complicated Operative Vaginal DeliveriesJose Luis RChNo ratings yet
- Accuracy of standard estimated fetal weight assessment in congenital diaphragmatic herniaDocument5 pagesAccuracy of standard estimated fetal weight assessment in congenital diaphragmatic herniabayuwinotoNo ratings yet
- Proton Pump Inhibitor Therapy For Eosinophilic Esophagitis: A Paradigm ShiftDocument4 pagesProton Pump Inhibitor Therapy For Eosinophilic Esophagitis: A Paradigm ShiftbayuwinotoNo ratings yet
- Maternal Mortality: Beyond Overmedicalized SolutionsDocument3 pagesMaternal Mortality: Beyond Overmedicalized SolutionsbayuwinotoNo ratings yet
- Thyroid and Weight American Thyroid AssociationDocument1 pageThyroid and Weight American Thyroid AssociationbayuwinotoNo ratings yet
- Treatment of Vasa PreviaDocument5 pagesTreatment of Vasa PreviaDewina Dyani Rosari IINo ratings yet
- Colpocleisis: A Guide For WomenDocument2 pagesColpocleisis: A Guide For WomenbayuwinotoNo ratings yet
- Algo FibrinolyticDocument2 pagesAlgo FibrinolyticBobo SmithyNo ratings yet
- Magnesium and Type 2 Diabetes: Mario Barbagallo, Ligia J DominguezDocument7 pagesMagnesium and Type 2 Diabetes: Mario Barbagallo, Ligia J DominguezbayuwinotoNo ratings yet
- 10 1001@jama 2016 0287Document10 pages10 1001@jama 2016 0287ompardor7554No ratings yet
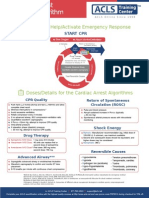
- Shout For Help/Activate Emergency Response: CPR StartDocument2 pagesShout For Help/Activate Emergency Response: CPR StartdavpierNo ratings yet
- Algo FibrinolyticDocument2 pagesAlgo FibrinolyticBobo SmithyNo ratings yet
- Proton Pump Inhibitor Therapy For Eosinophilic Esophagitis: A Paradigm ShiftDocument4 pagesProton Pump Inhibitor Therapy For Eosinophilic Esophagitis: A Paradigm ShiftbayuwinotoNo ratings yet
- Pathology and Pathophysiology of Atherothrombosis: Virchow's Triad Revisited Atsushi YDocument21 pagesPathology and Pathophysiology of Atherothrombosis: Virchow's Triad Revisited Atsushi YbayuwinotoNo ratings yet
- hsCRP Role in CardiologyDocument10 pageshsCRP Role in CardiologybayuwinotoNo ratings yet
- SEMANGKADocument8 pagesSEMANGKAbayuwinotoNo ratings yet
- RANZCO 2012 PosterDocument7 pagesRANZCO 2012 PosterGray Design GroupNo ratings yet
- Philippines Health Facility Self-Assessment Form COVID-19 IPCDocument9 pagesPhilippines Health Facility Self-Assessment Form COVID-19 IPCquesterNo ratings yet
- Ice MassageDocument2 pagesIce Massagevenkata ramakrishnaiahNo ratings yet
- Prostate Cancer PDFDocument2 pagesProstate Cancer PDFkapczukNo ratings yet
- Hereditary Spastic Paraplegia - UpToDateDocument22 pagesHereditary Spastic Paraplegia - UpToDateMatheus AraújoNo ratings yet
- Ca 19 9Document3 pagesCa 19 9डा. सत्यदेव त्यागी आर्यNo ratings yet
- Nurses Knowledge On Autism Spectrum DisordersDocument12 pagesNurses Knowledge On Autism Spectrum Disordersberrick otienoNo ratings yet
- Texas Children's Hospital 5 Annual Advanced Practice Provider ConferenceDocument64 pagesTexas Children's Hospital 5 Annual Advanced Practice Provider ConferenceEngSabbaghNo ratings yet
- LOCUS scoring sheet analysisDocument2 pagesLOCUS scoring sheet analysistakemebrickNo ratings yet
- Pathophysiology of StrokeDocument3 pagesPathophysiology of StrokeAqeel Al-Mahdaly0% (1)
- DSM-5 and Neurocognitive DisordersDocument6 pagesDSM-5 and Neurocognitive DisordersluishelNo ratings yet
- White Paper On Microbial Anti-Cancer Therapy and PDocument24 pagesWhite Paper On Microbial Anti-Cancer Therapy and PeullobaNo ratings yet
- Prioritized List of Nursing Problems (Dental Caries)Document2 pagesPrioritized List of Nursing Problems (Dental Caries)Chelsea Maisie CabralNo ratings yet
- Hormonal TherapiesDocument39 pagesHormonal TherapiesJalal EltabibNo ratings yet
- Acute Angle Closure GlaucomaDocument17 pagesAcute Angle Closure GlaucomaOvidiu RusuNo ratings yet
- 131 - Acute Vs Chronic InflammationDocument7 pages131 - Acute Vs Chronic InflammationAqib KhalidNo ratings yet
- Assign 1 - Cardiovascular System - ANSWER KEYDocument6 pagesAssign 1 - Cardiovascular System - ANSWER KEYF6imNo ratings yet
- RESEARCH 1 Fi 2Document20 pagesRESEARCH 1 Fi 2Alondra SagarioNo ratings yet
- Protocol for acute illness in SCADDDocument4 pagesProtocol for acute illness in SCADDRajiv Kabad0% (1)
- Las drogas: Life can take you higher than any kind of drugDocument2 pagesLas drogas: Life can take you higher than any kind of drugAngel RobertoNo ratings yet
- Indications, Contraindications and Monitoring of Enteral NutritionDocument13 pagesIndications, Contraindications and Monitoring of Enteral Nutritionbocah_britpopNo ratings yet
- Healthy Ways to Survive and Help Others in CrisisDocument91 pagesHealthy Ways to Survive and Help Others in CrisisfsimsdcNo ratings yet
- Hypertension in Pregnancy (Pogs-Cpg)Document55 pagesHypertension in Pregnancy (Pogs-Cpg)Philip Piolo Fuego67% (3)
- NCLEX Drug CardsDocument136 pagesNCLEX Drug CardsC Johnson100% (44)
- CBU 5th Year Exam Paper 1 2017Document13 pagesCBU 5th Year Exam Paper 1 2017Homeground entertainment100% (3)
- COPD AE (Book) (20210118) (林冠霖)Document15 pagesCOPD AE (Book) (20210118) (林冠霖)林冠霖No ratings yet
- Fdar Cabg 3nesurgicalDocument5 pagesFdar Cabg 3nesurgicalMary Margareth GonzalesNo ratings yet
- Hashimoto EncephalopathyDocument37 pagesHashimoto EncephalopathyIbrahim IbrahimNo ratings yet
- Health Assessment 9Document16 pagesHealth Assessment 9shannon c. lewisNo ratings yet
- Heart Failure BrochureDocument2 pagesHeart Failure Brochureapi-251155476No ratings yet