You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Mobilization PlanDocument5 pagesMobilization PlanMartimolearn79% (56)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Role of Consultants in Civil Engineering: Dhaval M. ParikhDocument31 pagesRole of Consultants in Civil Engineering: Dhaval M. ParikhDr DhavalNo ratings yet
- Tech Spec - IbmsDocument128 pagesTech Spec - IbmsAnonymous NcB95G6XwNo ratings yet
- Capital Project ControlDocument31 pagesCapital Project ControlwegrNo ratings yet
- Work Breakdown StructureDocument6 pagesWork Breakdown StructuresohaibNo ratings yet
- Ethics of Management PDFDocument2 pagesEthics of Management PDFRicky0% (3)
- Company Profile Jatayu Company ProfileDocument29 pagesCompany Profile Jatayu Company ProfileAyu Catra KastaraNo ratings yet
- Critical Success Factors Telecommunication Network Equipment Procurement Projects MTN NigeriaDocument42 pagesCritical Success Factors Telecommunication Network Equipment Procurement Projects MTN NigeriaMigwiJ.Mwangi100% (1)
- Information Systems Project ManagementDocument180 pagesInformation Systems Project ManagementMuriithi MurageNo ratings yet
- An Introduction To AGILEDocument43 pagesAn Introduction To AGILElaxendraNo ratings yet
- Agile MethodologyDocument9 pagesAgile MethodologyJay Smith100% (1)
- Company ProfileDocument14 pagesCompany ProfileAdamu Rabiu100% (1)
- CV Update 2014 Amtris Mechanical and Civil EngineerDocument6 pagesCV Update 2014 Amtris Mechanical and Civil EngineerAMTRISNo ratings yet
- Pm-5104-Pc-Fm-Final Project-30-12-2021 - CDocument37 pagesPm-5104-Pc-Fm-Final Project-30-12-2021 - CsunainaNo ratings yet
- Search For Dissertations About: "Building Services": 56142 Doctoral PHD Dissertations From Sweden. in English. For FreeDocument3 pagesSearch For Dissertations About: "Building Services": 56142 Doctoral PHD Dissertations From Sweden. in English. For FreeAnonymous NcB95G6XwNo ratings yet
- AUB DG III EngineeringDocument31 pagesAUB DG III EngineeringThanhquy NguyenNo ratings yet
- NMODECDocument28 pagesNMODECAnonymous NcB95G6XwNo ratings yet
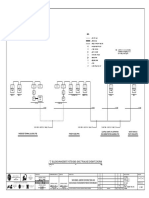
- Building Management System (BMS) Basic Trunkline Schematic Diagram 2Document3 pagesBuilding Management System (BMS) Basic Trunkline Schematic Diagram 2Anonymous NcB95G6XwNo ratings yet
- Approved Document FDocument22 pagesApproved Document FAnonymous NcB95G6XwNo ratings yet
- Powerflow 17-10 & 12-10 Range Brochure EnglishDocument2 pagesPowerflow 17-10 & 12-10 Range Brochure EnglishAnonymous NcB95G6XwNo ratings yet
- The e Book On Ip by DR - Manjula SandirigamaDocument93 pagesThe e Book On Ip by DR - Manjula SandirigamaAnonymous NcB95G6Xw100% (1)
- Oregon State Hospital Excellence ReportDocument104 pagesOregon State Hospital Excellence ReportStatesman JournalNo ratings yet
- Program Management StudyDocument19 pagesProgram Management Studynavinchopra1986No ratings yet
- The Risk Ranking of Projects A MethodologyDocument7 pagesThe Risk Ranking of Projects A MethodologyErganNo ratings yet
- Senior Construction Manager in Chicago IL Resume Charlene RifferDocument2 pagesSenior Construction Manager in Chicago IL Resume Charlene RifferCharleneRifferNo ratings yet
- A Description of The Background of The Project. 1.1 Manufacturing of Fabric Inspection MachineDocument15 pagesA Description of The Background of The Project. 1.1 Manufacturing of Fabric Inspection MachineBertrandMezatioNo ratings yet
- Supply Chain, LecturesDocument124 pagesSupply Chain, LecturesАдамNo ratings yet
- Airbus Group - Internship Within Engineering - Process ImprovementDocument6 pagesAirbus Group - Internship Within Engineering - Process ImprovementmontymilkyNo ratings yet
- University of Engineering & Management, Jaipur: Group-ADocument4 pagesUniversity of Engineering & Management, Jaipur: Group-ASupriyo BiswasNo ratings yet
- Gujarat University-T.y.bca SyllabusDocument19 pagesGujarat University-T.y.bca SyllabusSouvik BasuNo ratings yet
- Management Term Paper SampleDocument8 pagesManagement Term Paper Samplefdnmffvkg100% (1)
- Software Quality Assurance Research Paper PDFDocument4 pagesSoftware Quality Assurance Research Paper PDFegya6qzc100% (1)
- Batch 2017 6th Semester CSEDocument36 pagesBatch 2017 6th Semester CSEAzeem KhanNo ratings yet
- Guidelines For The Submission of Funding RequestsDocument12 pagesGuidelines For The Submission of Funding RequestsjnakakandeNo ratings yet
- Tasmanian Government Project Management Guidelines V7 0 July 2011 2Document196 pagesTasmanian Government Project Management Guidelines V7 0 July 2011 2Rachid HCNo ratings yet
- CV Carina Mendez CubaDocument2 pagesCV Carina Mendez CubaCarina MendezNo ratings yet
- Project Plan 3Document10 pagesProject Plan 3effectivNo ratings yet
- Cleaning of Billing DatabaseDocument5 pagesCleaning of Billing DatabaseOlusuyi Olurotimi FredrickNo ratings yet