You might also like
- Note Taking Methods for Effective ReadingDocument1 pageNote Taking Methods for Effective ReadingSenja FajarNo ratings yet
- 5 Chapter2 Clinical&Med - Term 09 MahasiswaDocument12 pages5 Chapter2 Clinical&Med - Term 09 MahasiswaSenja FajarNo ratings yet
- Analysing TopicsDocument1 pageAnalysing TopicsSenja FajarNo ratings yet
- Differences in academic writing styles across languagesDocument3 pagesDifferences in academic writing styles across languagesSenja FajarNo ratings yet
- Academic Writing-EIN 1Document24 pagesAcademic Writing-EIN 1Senja FajarNo ratings yet
- SG D GastrointestinalDocument22 pagesSG D GastrointestinalSenja FajarNo ratings yet
- English for Nurses GuidebookDocument18 pagesEnglish for Nurses GuidebookainigucciiNo ratings yet
- EIN1 SGD6 The Endocrine and Metabolic SystemDocument39 pagesEIN1 SGD6 The Endocrine and Metabolic SystemSenja FajarNo ratings yet
- Living Room Trauma DebateDocument3 pagesLiving Room Trauma DebateSenja FajarNo ratings yet
- Cardiovascular System PaperDocument18 pagesCardiovascular System PaperAyu Tria KartikaNo ratings yet
- Gatrointestinal SystemDocument15 pagesGatrointestinal SystemSenja FajarNo ratings yet
- EIN1 SGD4 Gastrointestinal SystemDocument18 pagesEIN1 SGD4 Gastrointestinal SystemSenja FajarNo ratings yet
- Oh My HoneyDocument1 pageOh My HoneySenja FajarNo ratings yet
- EIN1 SGD2 Nervous SystemDocument14 pagesEIN1 SGD2 Nervous SystemSenja FajarNo ratings yet
- Alimentary System, Is Responsible For Breaking Down Complex Food Into SimpleDocument2 pagesAlimentary System, Is Responsible For Breaking Down Complex Food Into SimpleSenja FajarNo ratings yet
- I Love You SayaDocument1 pageI Love You SayaSenja FajarNo ratings yet
- Ein1 Sgd3 Genitourinary SystemDocument22 pagesEin1 Sgd3 Genitourinary SystemSenja FajarNo ratings yet
- Oh My AllahDocument1 pageOh My AllahSenja FajarNo ratings yet
- EIN Kelompok 1 A3Document17 pagesEIN Kelompok 1 A3Senja FajarNo ratings yet
- Oh My HoneyDocument1 pageOh My HoneySenja FajarNo ratings yet
- Kardio Kel.2Document84 pagesKardio Kel.2Senja FajarNo ratings yet
- Pencernaan Gastritis Kel 5Document24 pagesPencernaan Gastritis Kel 5Senja FajarNo ratings yet
- Terjemahan Complications of Prolonged BedrestDocument7 pagesTerjemahan Complications of Prolonged BedrestSenja FajarNo ratings yet
- Chrons Dan Colitis UlceratifDocument38 pagesChrons Dan Colitis UlceratifSenja FajarNo ratings yet
- Dr335@medschl - Cam.ac - Uk: I Want To Ask For The Questionnaire DocumentDocument2 pagesDr335@medschl - Cam.ac - Uk: I Want To Ask For The Questionnaire DocumentSenja FajarNo ratings yet
- Biodata Pemain MoonlightDocument1 pageBiodata Pemain MoonlightSenja FajarNo ratings yet
- Quotes For NurseDocument4 pagesQuotes For NurseSenja FajarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Spark Zoology XI XII Eng 1Document16 pagesSpark Zoology XI XII Eng 1dfdsfsdefsdNo ratings yet
- Digestive - Histoworld ReferenceDocument12 pagesDigestive - Histoworld ReferenceKarl Torres Uganiza RmtNo ratings yet
- Malnutrition in Liver Cirrhosis: The Influence of Protein and SodiumDocument11 pagesMalnutrition in Liver Cirrhosis: The Influence of Protein and SodiumBadillo Buuren WillymanNo ratings yet
- DetoxificationDocument20 pagesDetoxificationapi-301746262100% (2)
- Final 2021 Benefit Year Final HHS Risk Adjustment Model CoefficientsDocument26 pagesFinal 2021 Benefit Year Final HHS Risk Adjustment Model CoefficientsJ CHANGNo ratings yet
- Pharmacology of Silymarin: F. Fraschini, G. Demartini and D. EspostiDocument15 pagesPharmacology of Silymarin: F. Fraschini, G. Demartini and D. EspostiVennyNo ratings yet
- ILC 2022 Abstract Book 08.06.2022Document1,104 pagesILC 2022 Abstract Book 08.06.2022Helena AlvesNo ratings yet
- Physiology of HyperbilirubinemiaDocument6 pagesPhysiology of HyperbilirubinemiaAdiel OjedaNo ratings yet
- Ascites Diagnosis and ManagementDocument8 pagesAscites Diagnosis and ManagementumasdeviNo ratings yet
- Understanding Hepatic Encephalopathy (HE) Symptoms, Causes and TreatmentDocument3 pagesUnderstanding Hepatic Encephalopathy (HE) Symptoms, Causes and TreatmentSuhas KandeNo ratings yet
- 1 s2.0 S1357303923000816 MainDocument6 pages1 s2.0 S1357303923000816 MaincamiloNo ratings yet
- Liver Cirrhosis Case PresentationDocument146 pagesLiver Cirrhosis Case Presentationjennachristy0395% (21)
- Norcet Notes PDFDocument4 pagesNorcet Notes PDFmonishaNo ratings yet
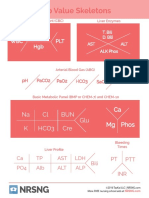
- Lab Value Skeletons: Ca MG Phos Na CL BUN K Hco3 Cre GluDocument1 pageLab Value Skeletons: Ca MG Phos Na CL BUN K Hco3 Cre GluGloryJaneNo ratings yet
- Therapeutic Diet To Control Different Types of DiseasesDocument79 pagesTherapeutic Diet To Control Different Types of DiseasesSouvik TewariNo ratings yet
- Gastroenterology Evaluation TemplateDocument2 pagesGastroenterology Evaluation Templatee-MedTools86% (7)
- 8 Biliary System, PSPD, 2013Document21 pages8 Biliary System, PSPD, 2013Cox AbeeNo ratings yet
- JaundiceDocument3 pagesJaundiceNyaoNyao MarcellanaNo ratings yet
- Lab ValuesDocument58 pagesLab ValuesAndy GoldstoneNo ratings yet
- Mahogany Seeds For Health BenefitsDocument14 pagesMahogany Seeds For Health BenefitsGreg PalmaNo ratings yet
- J Cellular Molecular Medi - 2014 - Liu - The Multiple Functional Roles of Mesenchymal Stem Cells in Participating inDocument10 pagesJ Cellular Molecular Medi - 2014 - Liu - The Multiple Functional Roles of Mesenchymal Stem Cells in Participating indr. RiyanNo ratings yet
- GIT MnemonicsDocument20 pagesGIT MnemonicsAhmed AbdelgelilNo ratings yet
- The Champion Text Book On Embalming 1908Document712 pagesThe Champion Text Book On Embalming 1908Ocean100% (3)
- Vijayalakshmi STM JournalDocument7 pagesVijayalakshmi STM JournalDharma RajanNo ratings yet
- Pathophysiology - CholedocholithiasisDocument1 pagePathophysiology - CholedocholithiasisMark OrculloNo ratings yet
- Liver Healing Recipes EbookDocument74 pagesLiver Healing Recipes EbookDarja Mežan100% (2)
- Biliary Tract DiseasesDocument13 pagesBiliary Tract DiseasesYara YousefNo ratings yet
- Blue Orange Creative Diabetes Presentation PDFDocument33 pagesBlue Orange Creative Diabetes Presentation PDFMohammad Omar BacaramanNo ratings yet
- The Carbon Tetrachloride Model in Mice: D Scholten, J Trebicka, C Liedtke and R WeiskirchenDocument8 pagesThe Carbon Tetrachloride Model in Mice: D Scholten, J Trebicka, C Liedtke and R WeiskirchenFaisalNo ratings yet
- Approach to Hepatomegaly, Splenomegaly and Hepatosplenomegaly in ChildrenDocument43 pagesApproach to Hepatomegaly, Splenomegaly and Hepatosplenomegaly in ChildrenLee Jun Xiong100% (2)