You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Immunization Knowledge, Attitude and Practice Among Mothers of Children From 0 To 5 YearsDocument77 pagesImmunization Knowledge, Attitude and Practice Among Mothers of Children From 0 To 5 YearsUlil Amri PramadaniNo ratings yet
- Knowledge, Attitude and Practices of Rural Mothers With Children Under Five Years of Age About Vaccination A Non Experimental StudyDocument9 pagesKnowledge, Attitude and Practices of Rural Mothers With Children Under Five Years of Age About Vaccination A Non Experimental StudyUlil Amri PramadaniNo ratings yet
- Assessment of Knowledge, Attitudes and Practices of Mothers in Jos North Regarding ImmunizationDocument9 pagesAssessment of Knowledge, Attitudes and Practices of Mothers in Jos North Regarding ImmunizationUlil Amri Pramadani100% (1)
- Bab 3 Case ReportDocument11 pagesBab 3 Case ReportUlil Amri PramadaniNo ratings yet
- Makalah Masalah Nyeri Pada Pasien TerminalDocument22 pagesMakalah Masalah Nyeri Pada Pasien TerminalSamuel U K HangguwaliNo ratings yet
- Barangay Mantuyong Bherts (Inventory of 1 Dose For Covid-19 Vaccination)Document1 pageBarangay Mantuyong Bherts (Inventory of 1 Dose For Covid-19 Vaccination)Barangay CentroNo ratings yet
- Whooping Cough (Pertussis) InformationDocument2 pagesWhooping Cough (Pertussis) InformationtombstoneepitaphNo ratings yet
- Paediatric and Paediatric Nursing IDocument541 pagesPaediatric and Paediatric Nursing ILUAMFULA RHC100% (1)
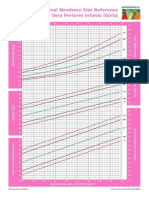
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- Conflicts of Interest - Undermine Children's HealthDocument42 pagesConflicts of Interest - Undermine Children's HealthSeth Alexander WoodNo ratings yet
- Scope of This Nursing Test I Is Parallel To The NP1 NLE CoverageDocument15 pagesScope of This Nursing Test I Is Parallel To The NP1 NLE CoverageHanah Kanashiro AlcoverNo ratings yet
- DM-MCH Prospectus July 201903apr2019094311 PGIMERDocument21 pagesDM-MCH Prospectus July 201903apr2019094311 PGIMERsgNo ratings yet
- OSCE in Pediatrics, 2011Document267 pagesOSCE in Pediatrics, 2011floare de colt0% (1)
- اللقاحاتDocument4 pagesاللقاحاتيمني مطنوخNo ratings yet
- Total Burn Care 5Th Edition David N Herndon All ChapterDocument67 pagesTotal Burn Care 5Th Edition David N Herndon All Chapterrichard.thomas647100% (9)
- Best Breastfeeding Positions by StageDocument3 pagesBest Breastfeeding Positions by StageAngelie Estilo Sarabia PacienteNo ratings yet
- Travel VaccinationsDocument3 pagesTravel VaccinationsOlive Health Travel ClinicNo ratings yet
- Certification: Office of The Municipal Health OfficerDocument15 pagesCertification: Office of The Municipal Health OfficerSample BakeshopNo ratings yet
- Grade School Parents Consent LetterDocument2 pagesGrade School Parents Consent LetterDario Basilio SaminNo ratings yet
- Updated Vaccination Card KNHSDocument4 pagesUpdated Vaccination Card KNHSlemar aribalNo ratings yet
- Lingual Frenotomy (Neonatal, Peds)Document4 pagesLingual Frenotomy (Neonatal, Peds)sittaNo ratings yet
- 5 Idol Ko Si Nanay Module 5Document48 pages5 Idol Ko Si Nanay Module 5Mash JumahariNo ratings yet
- CHN Courseplan GNMDocument6 pagesCHN Courseplan GNMChanchal ChauhanNo ratings yet
- Benefits of Virtual Pediatric CareDocument11 pagesBenefits of Virtual Pediatric CareWale teletotsNo ratings yet
- Byron Shire Council Notices: Subscribe To Council's Electronic Newsletters at WWW - Byron.nsw - Gov.au/newslettersDocument2 pagesByron Shire Council Notices: Subscribe To Council's Electronic Newsletters at WWW - Byron.nsw - Gov.au/newslettersByron Echo PublicationsNo ratings yet
- Adobe Scan Feb 18, 2023Document3 pagesAdobe Scan Feb 18, 2023Aura MeiNo ratings yet
- Laringomalacia - Nursing CareDocument9 pagesLaringomalacia - Nursing CareRirin Muthia ZukhraNo ratings yet
- RusDocument42 pagesRusОльга КалмыковаNo ratings yet
- School Based Immunization-FinalDocument22 pagesSchool Based Immunization-FinalMohammed T. Abdul Razak100% (2)
- Job Opportunities: Sr. No. Name of Hospital / Institution Post Name Specialty Name No. of PostsDocument11 pagesJob Opportunities: Sr. No. Name of Hospital / Institution Post Name Specialty Name No. of PostsAli AwanNo ratings yet
- Teratology (GA&E)Document23 pagesTeratology (GA&E)Suren BobNo ratings yet
- Trends in Pediatric and Pediatric NursingDocument4 pagesTrends in Pediatric and Pediatric NursingMary Menu0% (1)
- Guideline Rheumatic Disease in Children PDFDocument432 pagesGuideline Rheumatic Disease in Children PDFMada DobosNo ratings yet
- indonesia/PROFIL KESEHATAN 2018 1 PDFDocument2 pagesindonesia/PROFIL KESEHATAN 2018 1 PDFMudita DewiNo ratings yet