You might also like
- Brodsky 2004Document14 pagesBrodsky 2004Ervan SuryaNo ratings yet
- Pengetahuan IvfDocument20 pagesPengetahuan IvfErvan SuryaNo ratings yet
- Rekapan ErvanDocument18 pagesRekapan ErvanErvan SuryaNo ratings yet
- Grob Man 2018Document11 pagesGrob Man 2018Ervan SuryaNo ratings yet
- Qqsusunan Acara Pelatihanfff Metodologi Penelitian Perkumpulan Pecvvrinatologi Indonesia (Perinasia) Hari Pertamavv Waktu Topik NarasumberDocument1 pageQqsusunan Acara Pelatihanfff Metodologi Penelitian Perkumpulan Pecvvrinatologi Indonesia (Perinasia) Hari Pertamavv Waktu Topik NarasumberErvan SuryaNo ratings yet
- Lou Trad Is 1999Document5 pagesLou Trad Is 1999Ervan SuryaNo ratings yet
- 1 Maturasi Germinal VesicleDocument8 pages1 Maturasi Germinal VesicleErvan SuryaNo ratings yet
- Workbook 1Document4 pagesWorkbook 1Ervan SuryaNo ratings yet
- The Time Interval Between HCG Priming and Oocyte Retrieval in ART Program: A Meta-AnalysisDocument10 pagesThe Time Interval Between HCG Priming and Oocyte Retrieval in ART Program: A Meta-AnalysisErvan SuryaNo ratings yet
- Qqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertamavv Waktu Topik NarasumberDocument1 pageQqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertamavv Waktu Topik NarasumberErvan SuryaNo ratings yet
- The Relationship Between Cumulus Cell-Oocyte Coupling, Oocyte Meiotic Maturation, and Cumulus ExpansionDocument5 pagesThe Relationship Between Cumulus Cell-Oocyte Coupling, Oocyte Meiotic Maturation, and Cumulus ExpansionErvan SuryaNo ratings yet
- PerinasiaDocument1 pagePerinasiaErvan SuryaNo ratings yet
- Qqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertamavv Waktu Topik NarasumberDocument1 pageQqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertamavv Waktu Topik NarasumberErvan SuryaNo ratings yet
- Qqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertama Waktu Topik NarasumberDocument1 pageQqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertama Waktu Topik NarasumberErvan SuryaNo ratings yet
- Qqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertama Waktu Topik NarasumberDocument1 pageQqsusunan Acara Pelatihan Metodologi Penelitian Perkumpulan Perinatologi Indonesia (Perinasia) Hari Pertama Waktu Topik NarasumberErvan SuryaNo ratings yet
- PerinasiaDocument1 pagePerinasiaErvan SuryaNo ratings yet
- Documedunt 1Document1 pageDocumedunt 1Ervan SuryaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Risk Factors for Low Birth Weight in MalaysiaDocument5 pagesRisk Factors for Low Birth Weight in Malaysiaerine5995No ratings yet
- Should the Philippines Support Contraceptive Use to Save Lives and Support FamiliesDocument1 pageShould the Philippines Support Contraceptive Use to Save Lives and Support FamiliesApril Myles AlmalvezNo ratings yet
- Pregnancy Assessment Health History ROSDocument34 pagesPregnancy Assessment Health History ROSteuuuuNo ratings yet
- Real Sex: A Safe Sex Guide For TeensDocument9 pagesReal Sex: A Safe Sex Guide For TeensLilly CrumpNo ratings yet
- Preterm Labor: Dr. Cecille Rapal-GamboaDocument20 pagesPreterm Labor: Dr. Cecille Rapal-GamboaKatNo ratings yet
- The Long Acting Reversible Contraceptive (LARC) GuidelineDocument20 pagesThe Long Acting Reversible Contraceptive (LARC) GuidelineYinlerLeeNo ratings yet
- Hydrosalpinx Surgery Improves IVF OutcomesDocument8 pagesHydrosalpinx Surgery Improves IVF OutcomesWitono GunawanNo ratings yet
- Hormone Therapy Effects on Bone DensityDocument3 pagesHormone Therapy Effects on Bone DensitysmitNo ratings yet
- 2018-BJOG An International Journal of Obstetrics & GynaecologyDocument40 pages2018-BJOG An International Journal of Obstetrics & GynaecologyBagusHibridaNo ratings yet
- Permanent Family PlanningDocument24 pagesPermanent Family Planningsurajchavan231116No ratings yet
- Gynae BOOK NEWDocument23 pagesGynae BOOK NEWMuhtasim HaqueNo ratings yet
- Management of The Third Stage of LaborDocument12 pagesManagement of The Third Stage of Laborayu_pieterNo ratings yet
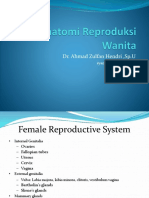
- Anatomi Reproduksi WanitaDocument23 pagesAnatomi Reproduksi WanitaocepNo ratings yet
- Nursing Care of Induction and Augmentation of LaborDocument17 pagesNursing Care of Induction and Augmentation of LaborZyrene RiveraNo ratings yet
- Partograph: A Graphical Record Of Labor Progress And ConditionsDocument49 pagesPartograph: A Graphical Record Of Labor Progress And Conditionsdr jai gurungNo ratings yet
- Pelvic Floor and Ovarian TumorsDocument117 pagesPelvic Floor and Ovarian TumorsTarek TarekNo ratings yet
- Adult Nursing & FeedingDocument48 pagesAdult Nursing & Feedingpicasso -da-vince71% (7)
- Menstrual Disorders DefinitionDocument4 pagesMenstrual Disorders DefinitionabraryeniNo ratings yet
- Female Pelvic Anatomy GuideDocument60 pagesFemale Pelvic Anatomy Guidekatherine nunnNo ratings yet
- UpToDate - Precipitous Birth Not Occurring On A Labor and Delivery UnitDocument31 pagesUpToDate - Precipitous Birth Not Occurring On A Labor and Delivery UnitH. FoeNo ratings yet
- Baby Shower TabooDocument4 pagesBaby Shower Taboosarahslist100% (9)
- CP102B FinalsDocument6 pagesCP102B FinalsAldrin Riel BoyanoNo ratings yet
- Congenital Malformations of The Genital Tract andDocument19 pagesCongenital Malformations of The Genital Tract andabhinay_1712100% (1)
- Jay ObDocument6 pagesJay ObJenxNo ratings yet
- Anatomy and Physiology of the Male and Female Reproductive SystemsDocument55 pagesAnatomy and Physiology of the Male and Female Reproductive SystemsJeffrey Roy Adlawan LopezNo ratings yet
- Turner's SyndromeDocument38 pagesTurner's SyndromeCerry PratiwiNo ratings yet
- Klompok 3 (Stage of Breastfeeding)Document14 pagesKlompok 3 (Stage of Breastfeeding)zulkarnainNo ratings yet
- Bimanual Vaginal Examination - OSCE Guide - Geeky MedicsDocument6 pagesBimanual Vaginal Examination - OSCE Guide - Geeky MedicsJahangir AlamNo ratings yet
- Placenta Previa Case StudyDocument59 pagesPlacenta Previa Case StudySiergs Smith GervacioNo ratings yet
- Ectopic Pregnancy: DR .Urmila KarkiDocument27 pagesEctopic Pregnancy: DR .Urmila KarkiBasudev chNo ratings yet