You might also like
- Aha Acls Prep Packet 2020Document69 pagesAha Acls Prep Packet 2020VP The Hacker100% (2)
- Photo QuizDocument21 pagesPhoto Quizabas_maytham1021100% (3)
- Lovenox (Enoxaparin) 80mgDocument1 pageLovenox (Enoxaparin) 80mgAdrianne BazoNo ratings yet
- ClexaneDocument2 pagesClexaneianecunar100% (2)
- DIS HeparinDocument4 pagesDIS HeparinRebecca ChenNo ratings yet
- Stop Anticoagulation Neuraxial AnesthesiaDocument3 pagesStop Anticoagulation Neuraxial AnesthesiaGihan NakhlehNo ratings yet
- Glasgow Coma ScaleDocument2 pagesGlasgow Coma Scalejean thereseNo ratings yet
- Medication Instructions Prior To SurgeryDocument11 pagesMedication Instructions Prior To Surgeryhohj100% (1)
- Republic of The Philippines Puerto Princesa City: Palawan State UniversityDocument2 pagesRepublic of The Philippines Puerto Princesa City: Palawan State UniversityRosemarie EustaquioNo ratings yet
- Enoxaparin Is Indicated For The Prevention of Ischemic Complications in Unstable Angina and in Non-Q-Wave Myocardial InfarctionDocument2 pagesEnoxaparin Is Indicated For The Prevention of Ischemic Complications in Unstable Angina and in Non-Q-Wave Myocardial Infarctionkharla suriagaNo ratings yet
- Enoxaparin FDADocument40 pagesEnoxaparin FDAImam Nur Alif Khusnudin100% (2)
- Drug StudiesDocument14 pagesDrug StudiesKen BaxNo ratings yet
- Critical Care Handbook 2013 PDFDocument118 pagesCritical Care Handbook 2013 PDFpracesar3871No ratings yet
- PIIS019096228 ZDocument2 pagesPIIS019096228 ZSake Cinema21No ratings yet
- Jcad 6 8 23Document6 pagesJcad 6 8 23Hadi FirmansyahNo ratings yet
- (2017) BELOUSOVA, Irena E. Mycosis Fungoides Manifesting As Giant Cell Lichenoid DermatitisDocument3 pages(2017) BELOUSOVA, Irena E. Mycosis Fungoides Manifesting As Giant Cell Lichenoid DermatitisCassandra VérasNo ratings yet
- 1 Example14Document2 pages1 Example14Rudolf KiraljNo ratings yet
- Letter to the Editor on MRI Diagnosis of Diabetic Foot InfectionsDocument1 pageLetter to the Editor on MRI Diagnosis of Diabetic Foot InfectionsKita KuatNo ratings yet
- De Novo Histoid Leprosy With Borderline Tuberculoi PDFDocument5 pagesDe Novo Histoid Leprosy With Borderline Tuberculoi PDFNelsi Mellisa DewiNo ratings yet
- British Medical Journal article examines new hypothesis for venous ulceration causesDocument2 pagesBritish Medical Journal article examines new hypothesis for venous ulceration causesJohn CaldasNo ratings yet
- Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS) SyndromeDocument7 pagesDrug Reaction With Eosinophilia and Systemic Symptoms (DRESS) SyndromeJeannette VillegasNo ratings yet
- CeaaDocument3 pagesCeaaAlfi RahmatikaNo ratings yet
- Jurnal P.acnesDocument4 pagesJurnal P.acnesFazlicha SyaradilaNo ratings yet
- Document on skin changes associated with hypothyroidismDocument3 pagesDocument on skin changes associated with hypothyroidismKrystal VallesNo ratings yet
- Benn Et Al. 2021Document8 pagesBenn Et Al. 2021Diego CisnNo ratings yet
- International Journal of Dermatology and VenereologyDocument3 pagesInternational Journal of Dermatology and VenereologyCuiting FengNo ratings yet
- Purpura Fulminans: A Cutaneous Marker of Disseminated Intravascular CoagulationDocument1 pagePurpura Fulminans: A Cutaneous Marker of Disseminated Intravascular Coagulationvaleee92No ratings yet
- Archderm 1971 04000210094019Document5 pagesArchderm 1971 04000210094019Harold FernandezNo ratings yet
- Nifedipine-Lnduced Erythema Multiforme: Sarah) - Barker, Charles Bayliff, Mccormack and DilworthDocument3 pagesNifedipine-Lnduced Erythema Multiforme: Sarah) - Barker, Charles Bayliff, Mccormack and DilworthIrma NoviantiNo ratings yet
- Acne Urticata and Chronic Myelogenous LeukemiaDocument4 pagesAcne Urticata and Chronic Myelogenous LeukemiaGo McFlyNo ratings yet
- Circumscribed Nevoid Angiokeratoma Report of Three New CasesDocument6 pagesCircumscribed Nevoid Angiokeratoma Report of Three New CasesAthenaeum Scientific PublishersNo ratings yet
- A Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and ColchicineDocument4 pagesA Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and Colchicinekahkashanahmed065No ratings yet
- Caz de Toxoplasmoza CutanataDocument7 pagesCaz de Toxoplasmoza Cutanatacatalina criceaNo ratings yet
- HBOT Helps Heal Hydroxyurea Leg Ulcer in Polycythemia PatientDocument2 pagesHBOT Helps Heal Hydroxyurea Leg Ulcer in Polycythemia PatientrajeevdeoNo ratings yet
- BR J Dermatol - 2022 - Dissemond - Inflammatory Skin Diseases and WoundsDocument11 pagesBR J Dermatol - 2022 - Dissemond - Inflammatory Skin Diseases and Woundsวสุชล ชัยชาญNo ratings yet
- UntitledDocument3 pagesUntitledShintaNo ratings yet
- Interstitial Granulomatous Dermatitis: A Rare Case Report of Dermatological Manifestation of Rheumatoid ArthritisDocument6 pagesInterstitial Granulomatous Dermatitis: A Rare Case Report of Dermatological Manifestation of Rheumatoid ArthritisFurgu TenzinNo ratings yet
- Lip Angioedema Swellimng and HSV Following HA InjDocument2 pagesLip Angioedema Swellimng and HSV Following HA InjOmar NagrashNo ratings yet
- Digital Vein ThrombosisDocument4 pagesDigital Vein ThrombosishestyNo ratings yet
- Jarrams 1966Document2 pagesJarrams 1966Luiz Felipe CruzNo ratings yet
- JournalDocument5 pagesJournalgabbynengNo ratings yet
- A Rare Case of Evans Syndrome Associated With Underlying Dermatomyositis Without Generalized Subcutaneous Edema A Case ReportDocument5 pagesA Rare Case of Evans Syndrome Associated With Underlying Dermatomyositis Without Generalized Subcutaneous Edema A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Recurrent Leg Ulcers in A Young Man With HyperhomoDocument4 pagesRecurrent Leg Ulcers in A Young Man With HyperhomoalfonsoNo ratings yet
- Case ReportDocument6 pagesCase ReportSalma KarimahNo ratings yet
- Urticarial Vasculitis Associated With Essential THDocument3 pagesUrticarial Vasculitis Associated With Essential THgugicevdzoceNo ratings yet
- Herpes X IsquemiaDocument2 pagesHerpes X IsquemiaBruna ReolonNo ratings yet
- Doshi 2009Document4 pagesDoshi 2009Salsa BilaNo ratings yet
- Cde 0006 0119Document5 pagesCde 0006 0119Mati AjaNo ratings yet
- Metastatic vulvar carcinoma mimicking genital herpesDocument3 pagesMetastatic vulvar carcinoma mimicking genital herpesSteve EdwardNo ratings yet
- Miyoshi 1998Document7 pagesMiyoshi 1998dad dzd adaNo ratings yet
- 15: Peripheral Vascular Disease: Patient Evaluation The Vascular DiseasesDocument15 pages15: Peripheral Vascular Disease: Patient Evaluation The Vascular DiseasespoddataNo ratings yet
- Kimura Disease Case Report and Literature ReviewDocument5 pagesKimura Disease Case Report and Literature ReviewriyanysidikNo ratings yet
- Medicine: DRESS Syndrome With Thrombotic Microangiopathy Revealing A Noonan SyndromeDocument5 pagesMedicine: DRESS Syndrome With Thrombotic Microangiopathy Revealing A Noonan SyndromeMatteo CoenNo ratings yet
- Transient Eosinophilic Nodulomatosis A Report of Two CasesDocument6 pagesTransient Eosinophilic Nodulomatosis A Report of Two CasesAthenaeum Scientific PublishersNo ratings yet
- Dapsone Hypersensitivity Syndrome in A Leprosy Patient: Case StudyDocument5 pagesDapsone Hypersensitivity Syndrome in A Leprosy Patient: Case StudyridhaNo ratings yet
- Case ReportDocument5 pagesCase Reportyudhi kurniawanNo ratings yet
- Malignant Syphilis As The Presenting Complaint of Advanced HIVDocument4 pagesMalignant Syphilis As The Presenting Complaint of Advanced HIVManuel López FuentesNo ratings yet
- Drug Reaction With Eosinophilia and Systemic Symptoms (Dress)Document8 pagesDrug Reaction With Eosinophilia and Systemic Symptoms (Dress)Okki Masitah Syahfitri NasutionNo ratings yet
- Pancytopenia in Cytophagic Histiocytic PanniculitisDocument3 pagesPancytopenia in Cytophagic Histiocytic PanniculitisAdvanced Research PublicationsNo ratings yet
- Erythroderma: How To Know If It Is Drug Induced?Document2 pagesErythroderma: How To Know If It Is Drug Induced?Juharny Eka SackbaniNo ratings yet
- Hemophilic Arthropathy JaaosDocument12 pagesHemophilic Arthropathy JaaosErnesto GariNo ratings yet
- Acute Generalized Exanthematous Pustulosis (AGEPDocument37 pagesAcute Generalized Exanthematous Pustulosis (AGEPJUAN CARLOSNo ratings yet
- HIV Hemicorea CNS Histoplasmosis 2016Document3 pagesHIV Hemicorea CNS Histoplasmosis 2016Juan Salazar PajaresNo ratings yet
- Weber Medicine & Clinical Case Reports ISSN:2449-1624: © Author(s) 2017. CC Attribution 3.0 LicenseDocument5 pagesWeber Medicine & Clinical Case Reports ISSN:2449-1624: © Author(s) 2017. CC Attribution 3.0 LicenseErika Majin MorenoNo ratings yet
- 1 Example10Document1 page1 Example10Rudolf KiraljNo ratings yet
- Krull 1985Document8 pagesKrull 1985Heba VerebceanNo ratings yet
- Cutaneous Polyarteritis Nodosa in A Child FollowinDocument2 pagesCutaneous Polyarteritis Nodosa in A Child FollowinandresrogersNo ratings yet
- MelanosisDocument3 pagesMelanosisGonzalo DlccNo ratings yet
- Prurigo Nodularis of HydeDocument12 pagesPrurigo Nodularis of HydeAugusto MonjardimNo ratings yet
- Nonbullous Pemphigoid: Prodrome of Bullous Pemphigoid or A Distinct Pemphigoid Variant?Document7 pagesNonbullous Pemphigoid: Prodrome of Bullous Pemphigoid or A Distinct Pemphigoid Variant?FatimaNo ratings yet
- Nursing Care Plan for Infection and Bleeding PrecautionsDocument6 pagesNursing Care Plan for Infection and Bleeding Precautionshayascent hilarioNo ratings yet
- Bartter SyndromeDocument6 pagesBartter SyndromeIKM MayorNo ratings yet
- STOPP Oleh Dr. LiliDocument3 pagesSTOPP Oleh Dr. LiliIKM MayorNo ratings yet
- NorepinephrineDocument9 pagesNorepinephrineDimitris KaragkiozidisNo ratings yet
- 1 SM PDFDocument8 pages1 SM PDFIKM MayorNo ratings yet
- Algorithm For The Diagnosis of NAFLD and NASH in Patients With Prediabetes or T2DM in Clinical PracticeDocument1 pageAlgorithm For The Diagnosis of NAFLD and NASH in Patients With Prediabetes or T2DM in Clinical PracticeIKM MayorNo ratings yet
- I Ghani 2017Document4 pagesI Ghani 2017IKM MayorNo ratings yet
- Sindrom Gradenigo Pada OMSK Tipe Bahaya - YurniDocument15 pagesSindrom Gradenigo Pada OMSK Tipe Bahaya - YurniIKM MayorNo ratings yet
- Brain EdemaDocument27 pagesBrain EdemaarininisaulNo ratings yet
- 16 - 255berita Terkini-Perawatan Dan Penyembuhan Luka KronikDocument10 pages16 - 255berita Terkini-Perawatan Dan Penyembuhan Luka KronikIKM MayorNo ratings yet
- Ch10 WilcoxonDocument10 pagesCh10 WilcoxonSen DiNo ratings yet
- Brain EdemaDocument27 pagesBrain EdemaarininisaulNo ratings yet
- Journal Pone 0193046 PDFDocument14 pagesJournal Pone 0193046 PDFIKM MayorNo ratings yet
- ID Faktor Risiko Kejadian Stunting Pada AnaDocument8 pagesID Faktor Risiko Kejadian Stunting Pada AnaAnonymous pYR4s37H6No ratings yet
- Healthy Mother, Healthy Baby Questionnaire: DemographicsDocument10 pagesHealthy Mother, Healthy Baby Questionnaire: DemographicsIKM MayorNo ratings yet
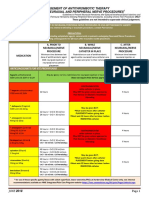
- Anticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectableDocument4 pagesAnticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectablepaulaNo ratings yet
- GBS Management, Medications and Nursing ConsiderationsDocument4 pagesGBS Management, Medications and Nursing Considerationssouledg3100% (1)
- Preoperative Evaluation Guide for Anesthesia and SurgeryDocument18 pagesPreoperative Evaluation Guide for Anesthesia and SurgeryanantosbiNo ratings yet
- Postpartum Health AssessmentDocument11 pagesPostpartum Health Assessmentapi-546355462No ratings yet
- Protamine SulphateDocument1 pageProtamine SulphateAndre PoeyNo ratings yet
- High Alert MedicationDocument46 pagesHigh Alert MedicationDewi Wara ShintaNo ratings yet
- Models For SuccessDocument48 pagesModels For Successirinuca12No ratings yet
- Crozer Manual - Second EditionDocument219 pagesCrozer Manual - Second EditionsgangamanNo ratings yet
- Hippokratia 11 013 PDFDocument9 pagesHippokratia 11 013 PDFGraham Allen ShowNo ratings yet
- Pro TaminaDocument2 pagesPro TaminaArcenciel26No ratings yet
- Xodo Document - Periprocedural - Anticoagulation - GuidelineDocument16 pagesXodo Document - Periprocedural - Anticoagulation - Guidelinebrigde_xNo ratings yet
- DVT Prophylaxis Safety ContraindicatDocument1 pageDVT Prophylaxis Safety Contraindicata1b14No ratings yet
- 01 Enoxaparin Pediatric ProtocolDocument2 pages01 Enoxaparin Pediatric ProtocolAmer WasimNo ratings yet
- Enoxaparin Sodium Manufacturer - Teena LabsDocument3 pagesEnoxaparin Sodium Manufacturer - Teena Labsteena labsNo ratings yet
- LovenoxDocument1 pageLovenoxAdrianne BazoNo ratings yet
- Enoxaparin Info SheetDocument7 pagesEnoxaparin Info SheetjafarkassimNo ratings yet
- VTE Prophylaxis GuidelinesDocument1 pageVTE Prophylaxis GuidelinesSylvia Ruth Alisa Nababan100% (1)
- Enoxaparin Guideline for Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin Guideline for Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Clinical Trial Details (PDF Generation Date:-Sun, 21 Feb 2021 06:02:40 GMT)Document9 pagesClinical Trial Details (PDF Generation Date:-Sun, 21 Feb 2021 06:02:40 GMT)ANILNo ratings yet