You might also like
- Study Guide PMHNP Must Know Exam Topics Cheat Sheet: by ViaDocument3 pagesStudy Guide PMHNP Must Know Exam Topics Cheat Sheet: by ViaDodo Eggo100% (4)
- 10 Cognitive DisordersDocument16 pages10 Cognitive DisordersFarrah MaeNo ratings yet
- PMHNP Ancc ReviewDocument4 pagesPMHNP Ancc ReviewEllie Mehr75% (4)
- K P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionDocument36 pagesK P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionArama CristiNo ratings yet
- n597 Psychiatric Soap Note 2Document7 pagesn597 Psychiatric Soap Note 2api-532870494No ratings yet
- Notes For PMHNP CertificationDocument23 pagesNotes For PMHNP CertificationKristine Frost92% (13)
- DSM-IV Criteria MnemonicsDocument4 pagesDSM-IV Criteria Mnemonicsleonyap100% (1)
- USMLE Mnemonics PsychDocument4 pagesUSMLE Mnemonics Psychzhzizhzi100% (3)
- Psych Meds Review MaterialDocument2 pagesPsych Meds Review MaterialMary Romaine Dela Pasion100% (7)
- Psychiatry HX TakingDocument4 pagesPsychiatry HX TakingP KasikrishnarajaNo ratings yet
- Lab Monitoring For Psychiatric Medications: Reference TableDocument1 pageLab Monitoring For Psychiatric Medications: Reference TableTimothy Turscak100% (1)
- Psychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Document28 pagesPsychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Noman ButtNo ratings yet
- Initial Psychiatric FormDocument4 pagesInitial Psychiatric Formfocus16hoursgmailcomNo ratings yet
- PMHNP Case Study - EditedDocument7 pagesPMHNP Case Study - EditedSoumyadeep BoseNo ratings yet
- Psychiatric Interview (Autosaved)Document22 pagesPsychiatric Interview (Autosaved)Jana Victor100% (1)
- Clerkship - Psychiatric History and MseDocument24 pagesClerkship - Psychiatric History and MsefahmiNo ratings yet
- Stahl's 1st Ed Child & AdolDocument388 pagesStahl's 1st Ed Child & AdolfpNo ratings yet
- PsychopharmacologyDocument64 pagesPsychopharmacologyGaurav Tandon100% (2)
- Psychiatry PharmacologyDocument2 pagesPsychiatry PharmacologyMegatFitriAziz100% (4)
- Disorders Duration/Onset Symptoms/Manifestations Treatment: Childhood DDocument7 pagesDisorders Duration/Onset Symptoms/Manifestations Treatment: Childhood DActeen Myoseen100% (1)
- Handy Summary Chart Comparing The Main Medications For DepressionDocument2 pagesHandy Summary Chart Comparing The Main Medications For Depressionrowanpurdy100% (4)
- Janice Krug PMHNP ResumeDocument3 pagesJanice Krug PMHNP Resumeapi-416722296No ratings yet
- Psychiatry Note BookDocument37 pagesPsychiatry Note BookMustafa Kamal BangashNo ratings yet
- Antidepressant Therapy Algorithm PDFDocument12 pagesAntidepressant Therapy Algorithm PDFiwul kiwul KriwulNo ratings yet
- Psychiatry High Yield NotesDocument6 pagesPsychiatry High Yield Notesgregry2100% (2)
- Psychiatry: Mental State ExaminationDocument3 pagesPsychiatry: Mental State ExaminationSok-Moi Chok100% (3)
- Reviewer On PsychopharmacologyDocument28 pagesReviewer On PsychopharmacologyKristine Ann Hernandez100% (1)
- StahleDocument12 pagesStahlekhaledazima0% (2)
- Johnson and Vanderhoef PMHNP Certification Review ManualDocument451 pagesJohnson and Vanderhoef PMHNP Certification Review ManualSoojung Nam92% (13)
- Psychiatric Interview Kap ExtDocument61 pagesPsychiatric Interview Kap ExtNeba YenatuNo ratings yet
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonNo ratings yet
- "Serotonin Syndrome Causes HARM": Psychiatry PharamacologyDocument9 pages"Serotonin Syndrome Causes HARM": Psychiatry Pharamacologytycobb63100% (4)
- Psychiatric Interview, MSEDocument48 pagesPsychiatric Interview, MSEComia Karla100% (1)
- Practical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryDocument29 pagesPractical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryShahinaz ShamsNo ratings yet
- Antidepressant ChartDocument7 pagesAntidepressant Chartinher1tance100% (4)
- CHT Psyc AntidepressantDocument3 pagesCHT Psyc AntidepressantRicardo Lugon ArantesNo ratings yet
- Psychiatry Rating ScalesDocument4 pagesPsychiatry Rating ScalesRafaila TonyNo ratings yet
- Psychiatric History - MSEDocument7 pagesPsychiatric History - MSEDeepbluex100% (1)
- Psychiatry Study MaterialsDocument3 pagesPsychiatry Study Materialsgnanam ambalavananNo ratings yet
- Psych Final BlueprintDocument10 pagesPsych Final BlueprintGrace LivingstonNo ratings yet
- Varun Kumar, 2017 - Getting Started in PsychiatryDocument148 pagesVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- ReferenceDocument2 pagesReferenceAaron Shokar100% (2)
- Psych Med ChartsDocument5 pagesPsych Med ChartsNursingSchoolNotes100% (5)
- Mnemonics PDFDocument10 pagesMnemonics PDFAhmed HamidNo ratings yet
- Psych History TemplateDocument4 pagesPsych History TemplateChloe GoteraNo ratings yet
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 pagesSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNo ratings yet
- BoardReviewClass PsychiatryDocument28 pagesBoardReviewClass PsychiatryyepherenowNo ratings yet
- (Divalproate, CBZ, LTG) : Anxiety DisordersDocument3 pages(Divalproate, CBZ, LTG) : Anxiety DisordersGus AbellaNo ratings yet
- Psychiatric SheetDocument80 pagesPsychiatric SheetHigazi z'EagleNo ratings yet
- Psych Drugs Cheat SheetDocument4 pagesPsych Drugs Cheat SheetSuha Abdullah100% (4)
- Psychiatric History and ExaminationDocument14 pagesPsychiatric History and ExaminationPaolo Bonifacio100% (14)
- Psychiatry NotesDocument135 pagesPsychiatry Notesmerin sunilNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
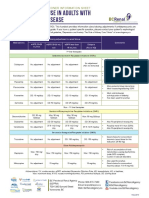
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- PSYC - Medication TemplateDocument15 pagesPSYC - Medication TemplateM Henry100% (1)
- HPI GuidelinesDocument5 pagesHPI GuidelinesHani NadiahNo ratings yet
- Child and Adolescent Psychiatry: A. Pervasive and Developmental DisordersDocument6 pagesChild and Adolescent Psychiatry: A. Pervasive and Developmental DisordersIsabel CastilloNo ratings yet
- Psychotropic Medication ReviewDocument7 pagesPsychotropic Medication ReviewAakash Shah100% (1)
- Pittsfield Public Schools New Code of Conduct, Character and SupportDocument65 pagesPittsfield Public Schools New Code of Conduct, Character and SupportThe Berkshire EagleNo ratings yet
- Developing Soft Skills and Personality Development Answer Key For Week 1 Assignment Multiple Choice QuestionsDocument5 pagesDeveloping Soft Skills and Personality Development Answer Key For Week 1 Assignment Multiple Choice QuestionsVelmurugan Thiagarajan100% (1)
- Research Paper On Barbie Doll by Marge PiercyDocument7 pagesResearch Paper On Barbie Doll by Marge Piercyafeaoebid100% (1)
- L - Aron - 1992 - From Ferenczi To Searles - PDDocument6 pagesL - Aron - 1992 - From Ferenczi To Searles - PDMario Manuel Fiorentino FerreyrosNo ratings yet
- My Practicum ExperienceDocument3 pagesMy Practicum Experienceapi-401842503100% (1)
- Cognitive Psychology Theory Process and Methodology 1st Edition McBride Test Bank DownloadDocument12 pagesCognitive Psychology Theory Process and Methodology 1st Edition McBride Test Bank DownloadRicardo Rivera100% (24)
- Development TasksDocument4 pagesDevelopment TasksgretutegeruteNo ratings yet
- ThesisDocument42 pagesThesisJhay PeeNo ratings yet
- Pakshaj ResumeDocument3 pagesPakshaj ResumeTanuj yadavNo ratings yet
- Job Advert - Clinical Psychologist080823Document2 pagesJob Advert - Clinical Psychologist080823tutorfelix777No ratings yet
- How To Be A Better NegotiatorDocument10 pagesHow To Be A Better NegotiatorBrezai Mihai-IonNo ratings yet
- FedEx CorporationDocument18 pagesFedEx Corporationshabaz17100% (1)
- The Hawthorne StudiesDocument10 pagesThe Hawthorne StudiesKancerNo ratings yet
- Teacher Student InteractionDocument2 pagesTeacher Student InteractionPretty DialloNo ratings yet
- Thesis-II - Group 5Document5 pagesThesis-II - Group 5Dianne RuizNo ratings yet
- DipressionDocument8 pagesDipressionImtiaz Hussain100% (1)
- Crime Analysis With Crime Mapping 4th Edition by Santos ISBN Test BankDocument15 pagesCrime Analysis With Crime Mapping 4th Edition by Santos ISBN Test Bankshaun100% (22)
- YaniDocument16 pagesYaniChristianWiradendiNo ratings yet
- Sexual Selection and Evolution Experiments 67Document26 pagesSexual Selection and Evolution Experiments 67joanneNo ratings yet
- STSDocument4 pagesSTSMGPagaduanNo ratings yet
- Human Resource Management in The Events PDFDocument14 pagesHuman Resource Management in The Events PDFPhuong NhungNo ratings yet
- Introduction To Artificial Intelligence Week 18Document14 pagesIntroduction To Artificial Intelligence Week 18Irene PayadNo ratings yet
- Consumer Perceptions of ServiceDocument24 pagesConsumer Perceptions of ServiceMahfuzur RahmanNo ratings yet
- SORIANO, Angelica Joan M. - NURSING CARE PLAN Activity 3. NCM 114Document9 pagesSORIANO, Angelica Joan M. - NURSING CARE PLAN Activity 3. NCM 114Angelica Joan SorianoNo ratings yet
- Group Behavior (Handout)Document3 pagesGroup Behavior (Handout)Jenyleen AgsalogNo ratings yet
- Early Marriage Analytical and Hotatory Exposition Text: A R R A N G E DDocument8 pagesEarly Marriage Analytical and Hotatory Exposition Text: A R R A N G E DciciNo ratings yet
- 3567 7418 1 PBDocument8 pages3567 7418 1 PBQuynh Anh TranNo ratings yet
- Sed 322 - Digital Weebly Portfolio Project Questions - Part IDocument3 pagesSed 322 - Digital Weebly Portfolio Project Questions - Part Iapi-279393811No ratings yet
- Agency of Depressed Adolescents Embodiment and Social RepresentationsDocument11 pagesAgency of Depressed Adolescents Embodiment and Social RepresentationsLoue HwangNo ratings yet
- Ogl 482 Module 5 Career Strategies Discussion 2Document3 pagesOgl 482 Module 5 Career Strategies Discussion 2api-556507529No ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)