Professional Documents
Culture Documents
Ajr 05 0932 PDF
Uploaded by
husadaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Ajr 05 0932 PDF
Uploaded by
husadaCopyright:
Available Formats
Merkle and A b d o m i n a l I m a g i n g • Pe r s p e c t i v e
Dale
Abdominal
MRI at 3.0 T
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
A C E N T U
R Y O F
Abdominal MRI at 3.0 T:
MEDICAL IMAGING
The Basics Revisited
Elmar M. Merkle1 OBJECTIVE. The purpose of our article is to describe the underlying physics concepts of
Brian M. Dale2 abdominal MRI at 3.0 T and their impact on signal-to-noise ratio, susceptibility artifacts, chem-
ical shift artifacts, and dielectric effects.
Merkle EM, Dale BM CONCLUSION. Abdominal MR sequence protocols optimized for 1.5-T scanners
should not be transferred to 3.0 T without substantial modification. In addition, specific patient
groups—for example, large patients with ascites—are not well suited to undergo an abdominal
MRI study at 3.0 T.
ver the past 2 years, ultrahigh- other regions of the body. It is also not clear
O field-strength whole-body 3.0-T
MR systems have been installed
in numerous institutions and are
which patient groups will benefit from an
ultrahigh-field abdominal MRI study and
which patient groups should remain on a
being increasingly used in clinics. Besides 1.5-T MR scanner. This article will illus-
market considerations—for example, stra- trate the underlying physics concepts of ab-
tegic investment to make a market state- dominal MRI at 3.0 T and their impact on
ment and to stay competitive—the main SNR, susceptibility artifacts, chemical shift
reason to purchase an ultrahigh-field MR artifacts, and dielectric effects. On the basis
system is the anticipated twofold MR sig- of these fundamental considerations, basic
nal-to-noise ratio (SNR) compared with a recommendations will be provided for
standard 1.5-T MR scanner. This gain in which patient groups will likely benefit
SNR can be kept or traded for either speed, from an ultrahigh-field MRI study and
spatial resolution, or both. Although the which patient groups should undergo a stan-
number of accessory receiving coils has dard 1.5-T abdominal MRI examination.
been limited in the past, the spectrum of
Keywords: abdominal imaging, field strength, MRI, MRI dedicated receiver coils offered by vendors 3.0 T Offers Twice the SNR:
technique, physics has increased significantly over the past 18 A Persistent Myth
months, which allows almost all standard The idea that twice the magnetic field will
DOI:10.2214/AJR.05.0932
MRI examinations to be performed on a give twice the SNR is appealing, and at first it
Received June 1, 2005; accepted after revision 3.0-T whole-body MR system. Although ul- seems correct because the intrinsic SNR in
July 20, 2005. trahigh-field MR systems have already been MRI is approximately proportional to the
shown to be advantageous for various indi- main magnetic field strength, B0 (equations 1
1Department of Radiology, Duke University Medical Center,
cations in the brain and musculoskeletal and 2) [6]. The equation for spin-echo–based
Duke North, Rm. 1417, Box 3808, Erwin Rd., Durham, NC
27710. Address correspondence to E. M. Merkle system compared with standard high-field MRI sequences is
(elmar.merkle@duke.edu). 1.5-T MR systems, only a few scientific
N PE N PA NAV
studies have been published describing the - ( 1 – e –TR ⁄ T1 )e –TE ⁄ T2
SNRSE ∝ B0 V ------------------------------- (1)
2Siemens BW
Medical Solutions, USA, Cary, NC 27519. use of 3.0-T MR systems in the chest, abdo-
CME
men, and pelvis [1–5]. Unfortunately, in- where SNRSE = signal-to-noise ratio for a spin-
This article is available for 1 CME credit. See supplemental sights gained in musculoskeletal or neu- echo pulse sequence, B0 = main magnetic field
data for this article at www.ajronline.org or visit roimaging research at 3.0 T cannot simply strength, V = voxel volume, NPE = number of
www.arrs.org for more information. be transferred to body MRI because MR se- acquired phase encode lines, NPA = number of
AJR 2006; 186:1524–1532
quence protocols and object sizes differ sig- acquired partitions, NAV = number of signals
nificantly in abdominal imaging. In addi- averaged, BW = receiver bandwidth per pixel,
0361–803X/06/1866–1524
tion, some artifacts are unique to ultrahigh- T1 = longitudinal relaxation time, and T2 =
© American Roentgen Ray Society field abdominal MRI and are not seen in transverse relaxation time.
1524 AJR:186, June 2006
Abdominal MRI at 3.0 T
The equation for gradient-echo–based MRI which would further reduce the gain in SNR at msec for kidney, 493 msec for liver), but at 3.0
sequences is ultrahigh-field-strength MRI (Fig. 1B) for T that difference shrinks to 21% (774 msec
long TE protocols. Given the optimistic as- for kidney, 641 msec for liver). For other tis-
N PE N PA N AV sin ( θ ) ( 1 – e –TR ⁄ T1 ) *
- -------------------------------------------------- e –TE ⁄ T2 (2)
SNRGRE ∝ B0 V ------------------------------- sumption that the transverse relaxation time sue pairs, the relative T1 dispersion may actu-
BW ( 1 – e – TR ⁄ T1 cos ( θ ) )
(T2) is independent of the main magnetic field ally increase at ultrahigh field strength, rather
where SNRGRE = signal-to-noise ratio for a strength and assuming only an increase of the than decreasing as shown here for kidney and
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
spoiled gradient-echo sequence and θ = flip longitudinal relaxation time (T1), equations 1 liver. In any case, this example should illus-
angle. and 2 can be used to determine the theoretic trate why the contrast between various tissues
Note that, in both equations 1 and 2, the maximum relative gain in SNR during MRI of on T1-weighted images at 3.0-T MRI cannot
term under the square root is simply the total the liver. For turbo spin-echo–based T2- be identical to the contrast seen on standard
time spent acquiring data. Therefore, SNR is weighted sequences with sequential acquisi- 1.5-T T1-weighted MRI. Fortunately, on the
proportional to the main magnetic field tion such as HASTE sequences, an increase by basis of our current experience with more
strength, the voxel volume, the square root of a factor of approximately 1.8 in SNR can than 300 abdominal cases examined at ultra-
the total sampling time, and some sequence- be obtained. For gradient-echo–based T1- high-field MRI, this has not been a relevant
specific contrast-related terms. Some of these weighted sequences such as in- and opposed- clinical problem.
factors, such as the longitudinal relaxation phase and VIBE (volume interpolated breath- A second major factor with a negative im-
time (T1), receiver bandwidth, and specific hold examination) sequences, an increase by a pact on the gain in SNR is related to the spe-
absorption rate limitations, can affect the factor of approximately 1.6–1.7 in SNR can be cific absorption rate (SAR). When the main
SNR in a somewhat complicated manner by obtained. Thus, the theoretic twofold increase magnetic field strength is doubled, the SAR,
impacting other sequence-specific parame- in SNR at 3.0 T compared with 1.5 T will not a measure for energy deposition within the
ters (e.g., TR, flip angle). generally be obtained without sequence pa- human body, increases by a factor of 4. Al-
The longitudinal relaxation time, T1, in- rameter optimization. though the energy deposited at 3.0 T is still
creases at a higher magnetic field strength, In addition to the absolute change in the T1 nonionizing, the increased SAR requires an
which causes a decrease in SNR [1, 7] (see relaxation time as a function of magnetic field increased concern for patient safety. Because
equations 1 and 2) (Fig. 1A). The transverse strength, there are also relative changes for body MRI at 3.0 T almost always runs at the
relaxation time, T2, on the other hand, seems to which the T1 relaxation time for one tissue in- upper limits of the allowed SAR deposition,
be fairly independent of the main magnetic creases at a different rate from the T1 relax- patients are more likely to experience an un-
field strength [7]. However, one recently pub- ation time of another tissue. For example, ac- comfortable sensation of warmth or heating.
lished study by de Bazelaire et al. [1] suggests cording to Bottomley et al. [7], at 1.5 T the T1 In addition, protocol adjustments are fre-
a marked decrease of the transverse relaxation relaxation time of the kidney is 32% greater quently necessary, such as an increase of the
time (T2) at higher magnetic field strengths, than the T1 relaxation time of the liver (652 TR, a decrease in the number of slices, or a
800
80
600
T2 (msec)
T1 (msec)
60
400
40
200
20
0
0 0.5 1.0 1.5 2.0 2.5 3.0 0 0.5 1.0 1.5 2.0 2.5 3.0
Field Strength (T) Field Strength (T)
A B
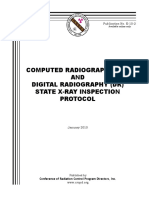
Fig. 1—Diagrammatic illustrations of relationships of relaxation times of liver tissue and main magnetic field strength (B0). Note that data of de Bazelaire et al. [1] are within
confidence interval obtained by Bottomley et al. [7] even though 3.0-T data point is outside scope of article by Bottomley et al.
A, Graph shows relationship of longitudinal relaxation time, T1, of liver tissue and main magnetic field strength. Data are shown from meta-analysis based on more than 800
study samples performed by Bottomley et al. [7] (■), together with data based on six volunteers acquired by de Bazelaire et al. [1] (▲). Note nonlinear increase of T1 of liver
tissue with main magnetic field strength. Also shown are nonlinear regression (solid line) and 95% confidence interval for data (dashed lines) as described by Bottomley et al.
B, Graph shows relationship of transverse relaxation time, T2, of liver tissue and main magnetic field strength. Data are shown from meta-analysis based on more than 250
study samples performed by Bottomley et al. [7] (▲), together with data based on six volunteers acquired by de Bazelaire et al. [1] (■). Note that no obvious relationship is
seen between T2 of liver tissue and main magnetic field strength. Also shown are mean (solid line) and 95% confidence interval (dashed lines) for data as described by
Bottomley et al.
AJR:186, June 2006 1525
Merkle and Dale
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
A B
C D
Fig. 2—Chemical shift artifacts of the first and second kinds at various magnetic field strengths in same patient, 32-year-old woman.
A, Axial gradient-echo in-phase image acquired at field strength of 1.5 T shows minimal chemical shift artifacts of the first kind along frequency-encoding axis.
B, Axial gradient-echo in-phase image acquired at field strength of 3.0 T shows marked chemical shift artifacts of the first kind along frequency-encoding axis that appear
bright toward higher part of readout gradient field (long arrow) and dark along lower part (short arrow).
C, Axial gradient-echo opposed-phase image acquired at field strength of 1.5 T shows chemical shift artifact of the second kind in all pixels along fat–water interface.
D, Axial gradient-echo opposed-phase image acquired at field strength of 3.0 T shows chemical shift artifact of the second kind, which is not significantly different from
artifact seen at standard magnetic field strength of 1.5 T (compare with C).
decrease of the flip angle. These adjustments pelvic MRI studies” when applying a proto- sulting in a difference of about 225 Hz at 1.5
are all undesirable because they increase col with similar spatial and temporal resolu- T, or a difference of about 450 Hz at 3.0 T.
scanning time, reduce anatomic coverage, al- tion at both field strengths. This difference causes a chemical shift mis-
ter contrast, or further reduce the gain in SNR registration, which is most easily seen around
at 3.0 T when compared with a standard 1.5- Chemical Shift Artifacts at 3.0 T: the kidneys (Fig. 2). The chemical shift arti-
T MRI system. Finally, much of the radiofre- A Double-Edged Sword fact of the first kind appears as a hypointense
quency transmitter and receiver technology at The chemical shift artifact of the first kind band, 1 to several pixels in width, toward the
1.5 T is relatively mature compared with the is due to a difference in the resonant fre- lower part of the readout gradient field, and as
newer technology at 3.0 T. quency between water and fat and is seen only a hyperintense band toward the higher part of
All these reasons contribute to a gain in along the frequency-encoding axis and the the readout gradient field. At a constant field
SNR that is less than the factor of 2.0 origi- slice-selection dimension [8]. This difference of view, base resolution, and receiver band-
nally expected. This may help explain why in resonant frequency is directly proportional width, the chemical shift artifact of the first
Morakkabati-Spitz et al. [4] found that, “Vi- to the main magnetic field strength and has kind will be twice as wide at 3.0 T as at stan-
sual signal to noise was rated equal for all 19 been measured as approximately 3.5 ppm, re- dard 1.5-T imaging. Usually, this enlarged ar-
1526 AJR:186, June 2006
Abdominal MRI at 3.0 T
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
A B
Fig. 3—Effect of receiver bandwidth on size of chemical shift artifacts of the first kind
at 3.0 T in 40-year-old man.
A, Axial in-phase T1-weighted gradient-echo image through kidney shows
significant chemical shift artifact (arrow) (receiver bandwidth, 210 Hz; pixel shift, 1.9;
SNR [signal-to-noise ratio]liver, 75).
B, Axial in-phase T1-weighted gradient-echo image through kidney with twice
receiver bandwidth as in A shows smaller chemical shift artifact (arrow) (receiver
bandwidth, 415 Hz; pixel shift, 1.0; SNRliver, 56). However, SNR is also decreased by
approximately 30%.
C, Axial in-phase T1-weighted gradient-echo image through kidney with four times
receiver bandwidth as in A shows markedly smaller chemical shift artifact (arrow)
(receiver bandwidth, 850 Hz; pixel shift, 0.5; SNRliver, 41). However, SNR is again
substantially decreased by another 30%.
tifact does not cause substantial problems in The chemical shift artifact of the second msec, and so on. Note that at 1.5 T, the fat
clinical body MRI at 3.0 T. However, it may kind is not limited to the frequency-encod- and water are phase-opposed at 2.2 msec
be problematic in selected cases such as the ing axis but may be seen in all pixels along and in phase at 4.4 sec (nominal values). In
search for a subcapsular renal hematoma or a fat–water interface because it is based on short, by doubling the field strength we have
an intramural aortic hematoma. In these an intravoxel phase-cancellation effect in halved the TEs for in-phase and opposed-
cases, the receiver bandwidth can be in- which fat and water exist in the same voxel phase imaging.
creased to minimize the chemical shift arti- [8]. The size of this artifact does not in- Fortunately, the increased difference in res-
fact of the first kind. Unfortunately, this crease with the main magnetic field strength onant frequency between water and fat at 3.0
comes at the expense of SNR: doubling the and is defined by the spatial resolution of T may also be advantageous because it allows
receiver bandwidth will decrease the SNR by the MR sequence (Fig. 2). However, the TE a better separation of the fat and water peak
approximately 30% (see equations 1 and needs to be adjusted because the frequency during MR spectroscopy, and a better or faster
2: 1--2- ≈ 0.7 → –30%) (Fig. 3). Another option difference is twice as large as with the stan- fat suppression using other chemical shift
is to repeat the MR pulse sequence with either dard 1.5-T MR systems, as described in the techniques as well—for example, fat satura-
chemical shift fat saturation, inversion null- section on chemical shift artifacts of the first tion and water excitation.
ing, or water excitation, which will eliminate kind. Using a 3.0-T MR system, both fat and
chemical shift artifacts effectively, allow im- water protons are in phase at 2.2, 4.4, 6.6 Susceptibility Artifacts: A Closer Look
aging at the lower bandwidth, and return the msec, and so on, and out of phase (also re- Magnetic susceptibility is the extent to
30% loss in SNR. ferred to as opposed phase) at 1.1, 3.3, 5.5 which a material becomes magnetized when
AJR:186, June 2006 1527
Merkle and Dale
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
Fig. 4—Effect of magnetic field strength on size of susceptibility artifacts in various MR sequences in vitro.
A, Photograph shows phantom setup with water-filled straw (arrow) embedded in gelatin. Three pairs of surgical clips (arrowheads) are embedded at various distances from straw.
B, HASTE image acquired at 1.5 T (TR/TE, 1,010/128; field of view, 250 mm2; slice thickness, 2.8 mm; matrix, 256 × 205; bandwidth, 490 Hz) shows typical susceptibility artifacts
caused by surgical clips.
C, HASTE image acquired at 3.0 T (1,010/128; field of view, 250 mm2; slice thickness, 2.8 mm; matrix, 256 × 205; bandwidth, 490 Hz) shows larger susceptibility artifacts caused
by surgical clips when compared with B.
D, Gradient-echo image acquired at 1.5 T (118/2.4; field of view, 280 × 210 mm2; slice thickness, 3.0 mm; matrix, 256 × 154; bandwidth, 385 Hz) shows typical susceptibility
artifacts caused by surgical clips.
E, Gradient-echo image acquired at 3.0 T (118/2.4; field of view, 280 × 210 mm2; slice thickness, 3.0 mm; matrix, 256 × 154; bandwidth, 385 Hz) shows larger susceptibility
artifacts caused by surgical clips when compared with D. Note that artifact size increases by approximately 100% in terms of volume.
A B
Fig. 5—Effect of magnetic field strength on size of metal-related susceptibility artifacts in vivo in 58-year-old man.
A, Gradient-echo opposed-phase image acquired at 1.5 T (TR/TE, 200/2.2) shows typical susceptibility artifacts caused by surgical clips (arrows).
B, Gradient-echo opposed-phase image acquired at 3.0 T (200/1.5) shows larger susceptibility artifacts (arrows) caused by surgical clips when compared with A despite
shorter TE.
1528 AJR:186, June 2006
Abdominal MRI at 3.0 T
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
A B
Fig. 6—Negative effect of magnetic field strength on size of gas-related susceptibility artifacts in vivo in 52-year-old man.
A, Gradient-echo in-phase image acquired at 1.5 T (TR/TE, 200/4.4) shows minor susceptibility artifacts (arrows) in hepatic flexure and transverse colon caused by colonic gas.
B, Gradient-echo in-phase image acquired at 3.0 T (200/4.4) shows larger susceptibility artifacts (arrows) in colon when compared with A. Note that these susceptibility
artifacts obscure colonic wall.
A B
Fig. 7—Positive effect of magnetic field strength on size of gas-related susceptibility artifacts in vivo in 65-year-old woman.
A, Gradient-echo in-phase image acquired at 1.5 T (TR/TE, 200/4.4) shows minor susceptibility artifact (arrow) in left hepatic bile duct caused by pneumobilia that may be
misinterpreted as a branch of portal venous system.
B, Gradient-echo in-phase image acquired at 3.0 T (200/4.4) shows markedly larger susceptibility artifact (arrow) in left hepatic bile duct caused by pneumobilia when
compared with A. Enlarged susceptibility artifact makes misinterpretation less likely.
placed in a magnetic field. Susceptibility ar- ventional procedures near or in the imaging This may be advantageous in selected cases
tifacts occur as the result of microscopic gra- field of view because the susceptibility of because metal-related susceptibility artifacts
dients or variations in the magnetic field metal is much higher than that of soft tissue. from surgical clips or surgical debris—for
strength that occur near the interfaces of ma- Susceptibility artifacts increase with the example, prior cholecystectomy or prior he-
terials of different magnetic susceptibility. main magnetic field strength and are approx- patic resection—may be better seen (Fig. 5).
These artifacts are usually caused by metal- imately twice as large in terms of volume at However, it is possible that enlarged suscep-
lic objects from previous surgical or inter- 3.0 T as at standard 1.5-T MRI [9] (Fig. 4). tibility artifacts may obscure important find-
AJR:186, June 2006 1529
Merkle and Dale
Fig. 8—Physical basis of radiofrequency shielding. In step A, rapidly varying
magnetic field (black arrows) induces a circulating electric field (white arrows). In
presence of a conductive medium (step B), circulating electric field leads to a
circulating current (gray arrows). In step C, circulating current acts as
electromagnet to produce magnetic field in opposite direction; and in step D,
amplitude of overall magnetic field is reduced. Note that steps B and C require a
conductive medium and that effect is stronger in more conductive medium. In
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
imaging, this effect can be noticed in patients with ascites or fetal imaging, in which
circulating currents can be established in relatively large regions of highly
conductive fluid. Resulting artifacts are generally more visible in sequences that use
a large number of radiofrequency pulses to generate contrast.
Fig. 9—Severe standing wave and conductivity artifact in 38-year-old woman with
liver cirrhosis and ascites during ultrahigh-field-strength MRI at 3.0 T.
A, Coronal HASTE image shows marked signal loss in center of image (arrows). Fluid
accumulations in peritoneal cavity enlarge abdomen and increase electrical
conductivity in field of view, causing severe artifacts.
B, Axial HASTE image again shows marked signal loss in center of image (arrows)
and represents severe standing wave and conductivity artifact.
C, Contrast-enhanced axial gradient-echo T1-weighted image acquired at same
level as B shows normal anatomy in center of field of view (arrows) and no evidence
of susceptibility artifacts.
A C
ings at 3.0-T MRI that may have been visu- vices that are considered MR safe at a field rigorously tested at 3.0 T as well before af-
alized at standard 1.5-T MRI. It must be strength of 1.5 T are not necessarily safe at fected patients can undergo an MRI exami-
clearly stated here that metal-containing de- 3.0 T [10–15]. All these devices need to be nation at this field strength.
1530 AJR:186, June 2006
Abdominal MRI at 3.0 T
Fig. 10—Severe standing (Figs. 9 and 10). In both cases, not only are
wave and conductivity the standing wave effects more pronounced
artifact in 28-year-old
pregnant woman during because of the enlarged abdomen, but greater
fetal ultrahigh-field- radiofrequency field attenuation is also
strength MRI at 3.0 T. present because of the increased amounts of
Coronal HASTE image
highly conductive amniotic or ascitic fluid.
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
shows marked signal
loss (long arrows). This
artifact is caused by Summary and General
large amount of amniotic Recommendations
fluid and increased size
of abdomen, which Body MRI at 3.0 T is still in its infancy and
increase electrical will improve substantially over the next sev-
conductivity in field of eral years. However, radiologists need to
view. Short thin arrows
mark placenta; thick know these several limitations based on the
arrows mark fetal torso. laws of physics:
(Courtesy of Jones B, First, overall, the gain in SNR at 3.0 T will
Cincinnati, OH)
be less than twofold compared with a stan-
dard 1.5-T MR system because of the ines-
capable increase of the longitudinal relax-
ation time T1. Also, the increased SAR
deposition at ultrahigh field strength often
requires protocol adjustments that can fur-
ther reduce the anticipated gain. The gain in
SNR will be higher in T2-weighted se-
Susceptibility artifacts also occur next to a result, strong signal variations across an im- quences than in T1-weighted sequences be-
gas-filled structures, such as the gas-filled age can be seen, especially brightening or dark cause longer TRs allow a more complete re-
bowel, because the susceptibility of gas is “holes” in regions away from the receive coil covery of the longitudinal magnetization,
much less than that of soft tissue (Fig. 6). caused by constructive or destructive interfer- and transverse relaxation times (T2) are
Thus, bowel wall imaging in patients with in- ence from the standing waves. These artifacts fairly independent of the main magnetic
flammatory bowel disease or patients referred become more pronounced the larger the region field strength. Thus, patients referred for MR
for MR colonography seems to be more chal- of interest is relative to the wavelength—that is, cholangiography may benefit from an ultra-
lenging at 3.0 T. However, enlarged suscepti- they are seen more in obese patients with a dis- high-field-strength MR examination.
bility artifacts due to a gas–soft-tissue inter- tended abdomen than in thin patients. Second, chemical shift artifacts of the first
face may also be helpful in detecting gas—for A rapidly changing magnetic field, like the kind are twice as large on ultrahigh-field MRI
example, intrahepatic pneumobilia or free in- radiofrequency transmit field, will induce a as on standard 1.5-T MRI. Chemical shift arti-
traperitoneal gas (Fig. 7). circulating electric field (Fig. 8). When this facts of the second kind, on the other hand, do
happens in a conductive medium, a circulat- not increase in size, although the timing is al-
Standing Wave Effects ing electric current is established. This cur- tered. Fortunately, the increased difference in
In addition to the exacerbation of artifacts rent in turn acts like an electromagnet that op- resonant frequency between water and fat at
that are seen at 1.5 T, some new artifacts also poses the changing magnetic field, reducing 3.0 T is also advantageous because it allows a
begin to appear at 3.0 T. These artifacts are re- the amplitude and dissipating the energy of better separation of the fat and water peaks dur-
lated to the higher frequency B1 transmit fields the radiofrequency field. The more conduc- ing MR spectroscopy and a better or faster fat
that are used at 3.0 T. The wavelength of the ra- tive the medium, the stronger the opposing suppression using chemical shift techniques.
diofrequency field at 128 MHz is 234 cm in free electromagnet and therefore the greater the Third, susceptibility artifacts are twice as
space, which is much larger than the field of attenuation of the radiofrequency field. In big on 3.0-T MRI. Although patients referred
view for clinical body imaging. However, water construction of the MRI suite, this principle is for a colon study may be challenging, the
(and most body tissue) has a rather high dielec- used by encasing the room in a copper con- search for gas—for example, free air or pneu-
tric constant, which reduces both the speed and ductor. Because of the high conductivity of mobilia—should be easier on 3.0-T MRI. Pa-
wavelength of electromagnetic radiation. For copper, any incoming radiofrequency waves tients with metal implants should undergo an
visible light, this effect causes a straight stick are almost completely attenuated and the MR examination at 3.0 T only if the metal-
entering water at an angle to appear bent. For magnet is shielded from external interference. containing device has been proven to be MR
MRI, this effect reduces the radiofrequency To a lesser extent, large amounts of relatively safe for this field strength.
field wavelength from 234 cm in free space to highly conductive tissues can cause similar Fourth, standing wave and conductivity ef-
about 30 cm in most human tissues—that is, shielding effects, resulting in hypointense ar- fects are usually not seen at a field strength of
water-containing tissues [16]. This size is ap- eas in the image where the radiofrequency 1.5 T. At 3.0 T, these artifacts are most pro-
proximately the size of the field of view for field is partially attenuated [16]. nounced in pregnant women in the second and
many body applications and can result in a so- These two effects combine to cause partic- third trimesters because of the large amount of
called standing wave effect (often incorrectly ularly strong artifacts for 3.0-T body MRI in amniotic fluid and the increased size of the ab-
called a “dielectric resonance” effect) [17]. As pregnant patients and in patients with ascites domen. Fetal MRI should therefore not be per-
AJR:186, June 2006 1531
Merkle and Dale
formed at 3.0 T because of these severe arti- male pelvis: preliminary experiences. Eur Radiol sessment of magnetic field interactions with a 3.0-
facts and the increased safety concerns. The 2005; 15:639–644 Tesla MR system. J Magn Reson Imaging 2002;
same holds true for patients with a large 5. Greenman RL, Shirosky JE, Mulkern RV, Rofsky 16:721–732
amount of ascites, who are also not well suited NM. Double inversion black-blood fast spin-echo 12. Shellock FG, Tkach JA, Ruggieri PM, Masaryk TJ.
for an ultrahigh-field MRI examination. imaging of the human heart: a comparison between Cardiac pacemakers, ICDs, and loop recorder: eval-
Finally, most patients can undergo an ab- 1.5 T and 3.0 T. J Magn Reson Imaging 2003; uation of translational attraction using conventional
Downloaded from www.ajronline.org by 202.80.217.171 on 11/22/16 from IP address 202.80.217.171. Copyright ARRS. For personal use only; all rights reserved
dominal MRI study at 3.0 T with a reasonable 17:648–655 (“long-bore”) and “short-bore” 1.5- and 3.0-Tesla
outcome in terms of image quality. 6. Edelstein WA, Glover GH, Hardy CJ, Redington MR systems. J Cardiovasc Magn Reson 2003;
RW. The intrinsic signal-to-noise ratio in NMR im- 5:387–397
Acknowledgments aging. Magn Reson Med 1986; 3:604–618 13. Baker KB, Nyenhuis JA, Hrdlicka G, Rezai AR,
We thank David E. Purdy and H. Cecil 7. Bottomley PA, Foster TH, Argersinger RE, Pfeifer Tkach JA, Shellock FG. Neurostimulation systems:
Charles for reviewing the manuscript and the LM. A review of normal tissue hydrogen NMR re- assessment of magnetic field interactions associ-
subsequent stimulating discussions. laxation times and relaxation mechanisms from ated with 1.5- and 3-Tesla MR systems. J Magn Re-
1–100 MHz: dependence on tissue type, NMR fre- son Imaging 2005; 21:72–77
quency, temperature, species, excision, and age. 14. Shellock FG, Gounis M, Wakhloo A. Detachable
References Med Phys 1984; 11:425–448 coil for cerebral aneurysms: in vitro evaluation of
1. de Bazelaire CM, Duhamel GD, Rofsky NM, Alsop 8. Elster AE, Burdette JH. Questions and answers in magnetic field interactions, heating, and artifacts at
DC. MR imaging relaxation times of abdominal and magnetic resonance imaging, 2nd ed. St. Louis, 3T. AJNR 2005; 26:363–366
pelvic tissues measured in vivo at 3.0 T: preliminary MO: Mosby, 2001:6, 128 15. Shellock FG, Forder JR. Drug eluting coronary
results. Radiology 2004; 230:652–659 9. Lewin JS, Duerk JL, Jain VR, Petersilge CA, Chao stent: in vitro evaluation of magnet resonance safety
2. Sosna J, Rofsky NM, Gaston SM, DeWolf WC, CP, Haaga JR. Needle localization in MR-guided at 3 Tesla. J Cardiovasc Magn Reson 2005;
Lenkinski RE. Determinations of prostate volume biopsy and aspiration: effects of field strength, se- 7:415–419
at 3-Tesla using an external phased array coil: com- quence design, and magnetic field orientation. AJR 16. Haacke EM, Brown RW, Thompson MR, Venkate-
parison to pathologic specimens. Acad Radiol 1996; 166:1337–1345 san R. Magnetic resonance imaging: physical prin-
2003; 10:846–853 10. Sommer T, Maintz D, Schmiedel A, et al. High field ciples and sequence design. New York, NY: Wiley,
3. Katz-Brull R, Rofsky NM, Lenkinski RE. Breath- MR imaging: magnetic field interactions of aneu- 1999:10, 662
hold abdominal and thoracic proton MR spectros- rysm clips, coronary artery stents and iliac artery 17. Collins CM, Liu W, Schreiber W, Yang QX, Smith
copy at 3T. Magn Reson Med 2003; 50:461–467 stents with a 3.0 Tesla MR system [in German]. MB. Central brightening due to constructive inter-
4. Morakkabati-Spitz N, Gieseke J, Kuhl C, et al. 3.0- Rofo 2004; 176:731–738 ference with, without, and despite dielectric reso-
T high-field magnetic resonance imaging of the fe- 11. Shellock FG. Biomedical implants and devices: as- nance. J Magn Reson Imaging 2005; 21:192–196
F O R YO U R I N F O R M AT I O N
This article is available for CME credit. See supplemental data for this
article at www.ajronline.org or visit www.arrs.org for more information.
1532 AJR:186, June 2006
You might also like
- Moore 2006Document5 pagesMoore 2006Aldo MartínezNo ratings yet
- IMRT: A Review and Preview: Physics in Medicine & BiologyDocument18 pagesIMRT: A Review and Preview: Physics in Medicine & BiologychatsashNo ratings yet
- Comparative Analysis of Radiation Dose and Image Quality BetweenDocument5 pagesComparative Analysis of Radiation Dose and Image Quality BetweenIshani Anushika JayakodyNo ratings yet
- Ajr Dect PDFDocument11 pagesAjr Dect PDFTom PatrickNo ratings yet
- Thyroid Scans: KeywordsDocument3 pagesThyroid Scans: KeywordsevanNo ratings yet
- Scanning Beyond Anatomic Limits of The Thorax in Chest CT - Findings, Radiation Dose, and Automatic Tube Current ModulationDocument6 pagesScanning Beyond Anatomic Limits of The Thorax in Chest CT - Findings, Radiation Dose, and Automatic Tube Current Modulationdestian ryanNo ratings yet
- Comparison of Angular and Combined Automatic Tube Current Modulation Techniques With Constant Tube Current CT of The Abdomen and PelvisDocument7 pagesComparison of Angular and Combined Automatic Tube Current Modulation Techniques With Constant Tube Current CT of The Abdomen and Pelvisdestian ryanNo ratings yet
- Build Your Own Radionic TunerDocument4 pagesBuild Your Own Radionic TunerGabriel Gonzales100% (2)
- Dual-Energy CT of The Brain and Intracranial VesselsDocument8 pagesDual-Energy CT of The Brain and Intracranial VesselsMuhammad Rafiee SukmaNo ratings yet
- Ringe Et Al 2012 Gadoxetate Disodium Enhanced Mri of The Liver Part 1 Protocol Optimization and Lesion Appearance inDocument16 pagesRinge Et Al 2012 Gadoxetate Disodium Enhanced Mri of The Liver Part 1 Protocol Optimization and Lesion Appearance indynachNo ratings yet
- Fourier Transform and PH EncDocument10 pagesFourier Transform and PH EncEdward Ventura BarrientosNo ratings yet
- CTA ExtremityDocument8 pagesCTA Extremityrio trisonaNo ratings yet
- MRI of The Peritoneum: Spectrum of AbnormalitiesDocument12 pagesMRI of The Peritoneum: Spectrum of AbnormalitiesasfwegereNo ratings yet
- Protable Ultra Sound AlokaDocument4 pagesProtable Ultra Sound AlokaAjish joNo ratings yet
- Vascular Smooth Muscle: Metabolic, Ionic, and Contractile MechanismsFrom EverandVascular Smooth Muscle: Metabolic, Ionic, and Contractile MechanismsM.F. III CrassNo ratings yet
- J Mric 2006 01 004Document12 pagesJ Mric 2006 01 004Muhammad SawalNo ratings yet
- Intro To Mathematical ConceptDocument26 pagesIntro To Mathematical ConceptSarah TolentinoNo ratings yet
- KULIAH ONKO K11-RT New FKDocument65 pagesKULIAH ONKO K11-RT New FKDickyNo ratings yet
- Karzmark 3Document11 pagesKarzmark 3f.kristell04No ratings yet
- What Is Your Diagnosis?: in Cooperation WithDocument3 pagesWhat Is Your Diagnosis?: in Cooperation WithLinda Lineros SilvaNo ratings yet
- Effects of Electromagnetic Field On The Development of Chick Embryo: An in Vivo Study - IntechOpenDocument2 pagesEffects of Electromagnetic Field On The Development of Chick Embryo: An in Vivo Study - IntechOpensokhna may seyeNo ratings yet
- An Imaging Algorithm For The Differential Diagnosis of Adrenal Adenomas and MetastasesDocument11 pagesAn Imaging Algorithm For The Differential Diagnosis of Adrenal Adenomas and MetastasesVicente Martínez SanjuanNo ratings yet
- Bateni Et Al 2013 Imaging Key Wrist Ligaments What The Surgeon Needs The Radiologist To KnowDocument7 pagesBateni Et Al 2013 Imaging Key Wrist Ligaments What The Surgeon Needs The Radiologist To KnowRadiologyNo ratings yet
- Clinical Practice in PET CT For The Management of Head and Neck Squamous Cell CancerDocument15 pagesClinical Practice in PET CT For The Management of Head and Neck Squamous Cell CancerlkitkatgirlNo ratings yet
- Body MRI Sequences: A Conceptual Framework: Applied Radiology January 2012Document7 pagesBody MRI Sequences: A Conceptual Framework: Applied Radiology January 2012Akanda RabbiNo ratings yet
- In Vivo Study of Human Skin Using Pulsed Terahertz RadiationDocument14 pagesIn Vivo Study of Human Skin Using Pulsed Terahertz RadiationRamon BaeNo ratings yet
- Sequence Optimization For MRI Acoustic NoiseDocument9 pagesSequence Optimization For MRI Acoustic NoiseArsy ZygomaticNo ratings yet
- Eye Lens Dose During CT ExamDocument7 pagesEye Lens Dose During CT ExamSamu SimamesaNo ratings yet
- Radiologist, Be Aware: Ten Pitfalls That Confound The Interpretation of Multiparametric Prostate MRIDocument12 pagesRadiologist, Be Aware: Ten Pitfalls That Confound The Interpretation of Multiparametric Prostate MRITurkiNo ratings yet
- PROPELLER Technique To Improve Image Quality of MRI of The ShoulderDocument8 pagesPROPELLER Technique To Improve Image Quality of MRI of The ShoulderDhoni AvantasiaNo ratings yet
- Electroporationfor PCDocument13 pagesElectroporationfor PCAnukhatan DavaarentsenNo ratings yet
- 217 FullDocument9 pages217 FullMiraNo ratings yet
- BulletinoftheNationalResearchCouncil 10034752Document175 pagesBulletinoftheNationalResearchCouncil 10034752Raju MundruNo ratings yet
- Classification of Common Acetabular Fractures: Radiographic and CT AppearancesDocument11 pagesClassification of Common Acetabular Fractures: Radiographic and CT AppearancesSharan SahotaNo ratings yet
- Settling Book Chapter-SELFDocument39 pagesSettling Book Chapter-SELFMD. SHOHANUR RAHMAN MITHUN ,160051087No ratings yet
- Solid Renal Masses: What The Numbers Tell Us: Stella K. Kang William C. Huang Pari V. Pandharipande Hersh ChandaranaDocument11 pagesSolid Renal Masses: What The Numbers Tell Us: Stella K. Kang William C. Huang Pari V. Pandharipande Hersh ChandaranaTạ Minh ZSNo ratings yet
- This Study Resource Was: Technological University of The PhilippinesDocument8 pagesThis Study Resource Was: Technological University of The Philippinespeter vanderNo ratings yet
- Journals Javma 246 3Document2 pagesJournals Javma 246 3Yo Nome AcuerdoNo ratings yet
- From the Midwife's Bag to the Patient's File: Public Health in Eastern and Southeastern EuropeFrom EverandFrom the Midwife's Bag to the Patient's File: Public Health in Eastern and Southeastern EuropeNo ratings yet
- Breast CancerDocument11 pagesBreast CancerAnonymous 8vwJIhUy4No ratings yet
- Christensen Et Al 2012 Characterization of The Solitary Pulmonary Nodule 18f FDG Pet Versus Nodule Enhancement CTDocument7 pagesChristensen Et Al 2012 Characterization of The Solitary Pulmonary Nodule 18f FDG Pet Versus Nodule Enhancement CTLeticia PortilloNo ratings yet
- Table of Reviewed StudiesDocument9 pagesTable of Reviewed StudiesyusficaNo ratings yet
- Ajr 09 4032Document7 pagesAjr 09 4032Roshi_11No ratings yet
- 10 1 1 457 7733 PDFDocument12 pages10 1 1 457 7733 PDFfranobeljo27No ratings yet
- Van Leeuwen Et Al 2013 Variations in Venous and Segmental Anatomy of The Liver Two and Three Dimensional MR Imaging inDocument9 pagesVan Leeuwen Et Al 2013 Variations in Venous and Segmental Anatomy of The Liver Two and Three Dimensional MR Imaging inUsateo TeoNo ratings yet
- De 01 First OrderDocument520 pagesDe 01 First OrderShashank KumarNo ratings yet
- 1987 - Precision For Coverages and Sample Size For Tolerance IntervalDocument18 pages1987 - Precision For Coverages and Sample Size For Tolerance IntervalNilkanth ChapoleNo ratings yet
- Glanda HipofizaDocument9 pagesGlanda HipofizaElena-Raluca CiolanNo ratings yet
- Ajr 163 1 8010211Document5 pagesAjr 163 1 8010211Eliana NataliaNo ratings yet
- Radiology of Chest Wall MassesDocument11 pagesRadiology of Chest Wall MassesDevina BumiNo ratings yet
- Effect of Patient Size On Radiation Dose of Abdominal MDCT With Automatic Tube Current ModulationDocument6 pagesEffect of Patient Size On Radiation Dose of Abdominal MDCT With Automatic Tube Current Modulationdestian ryanNo ratings yet
- Edical Ltrasound Ensors: Department of Biomedical Engineering Boston University, Boston, MA, USADocument38 pagesEdical Ltrasound Ensors: Department of Biomedical Engineering Boston University, Boston, MA, USAEduard CastellanosNo ratings yet
- Estimating Organ Dose in Computed Tomography Using Tube Current Modulation - A Monte Carlo SimulationDocument7 pagesEstimating Organ Dose in Computed Tomography Using Tube Current Modulation - A Monte Carlo Simulationdestian ryanNo ratings yet
- Wa0001.Document11 pagesWa0001.bhumikabasu058No ratings yet
- Aging of The Upper Lip: Part I: A Retrospective Analysis of Metric Changes in Soft Tissue On Magnetic Resonance ImagingDocument7 pagesAging of The Upper Lip: Part I: A Retrospective Analysis of Metric Changes in Soft Tissue On Magnetic Resonance ImagingJuliana BrunettoNo ratings yet
- Muskuloskeletal MR Imaging at 3.0 T: Current Status and Future PerspectivesDocument10 pagesMuskuloskeletal MR Imaging at 3.0 T: Current Status and Future PerspectivesEnrique SantiagoNo ratings yet
- Principles of Magnetic Resonance ImagingDocument11 pagesPrinciples of Magnetic Resonance ImagingAnonymous DuA3jEqUqNo ratings yet
- Uv Visible Spectrophotometric Method Development and Validation of Assay of Paracetamol Tablet Formulation 2155 9872.1000151Document9 pagesUv Visible Spectrophotometric Method Development and Validation of Assay of Paracetamol Tablet Formulation 2155 9872.1000151Delfin VqqNo ratings yet
- Naskah Publikasi (Indo)Document38 pagesNaskah Publikasi (Indo)husadaNo ratings yet
- Chest RadiographyDocument23 pagesChest Radiographyapi-3773951100% (2)
- Atlas HelpDocument8 pagesAtlas HelpHorga AdelineNo ratings yet
- Annisa, Bambang Satoto, Siti Masrochah: PendahuluanDocument4 pagesAnnisa, Bambang Satoto, Siti Masrochah: PendahuluanhusadaNo ratings yet
- Abdominal MRI at 3.0 T: The Basics Revisited: Elmar M. Merkle Brian M. DaleDocument9 pagesAbdominal MRI at 3.0 T: The Basics Revisited: Elmar M. Merkle Brian M. DalehusadaNo ratings yet
- Ajr 05 0932Document12 pagesAjr 05 0932husadaNo ratings yet
- Evaluasi Metode Penentuan Half Value LayDocument6 pagesEvaluasi Metode Penentuan Half Value LayhusadaNo ratings yet
- Annisa, Bambang Satoto, Siti Masrochah: PendahuluanDocument4 pagesAnnisa, Bambang Satoto, Siti Masrochah: PendahuluanhusadaNo ratings yet
- Annisa, Bambang Satoto, Siti Masrochah: Keyword: PDW - SPAIR, PDW - Fatsat, SNR, MRI Knee JointDocument6 pagesAnnisa, Bambang Satoto, Siti Masrochah: Keyword: PDW - SPAIR, PDW - Fatsat, SNR, MRI Knee JointhusadaNo ratings yet
- NO Kode Uraian: Rencana Anggaran Biaya Tahun 2018/2019 Stikes Awal Bros Pekanbaru Laboratorium RadiologiDocument8 pagesNO Kode Uraian: Rencana Anggaran Biaya Tahun 2018/2019 Stikes Awal Bros Pekanbaru Laboratorium RadiologihusadaNo ratings yet
- Jadwal Purchasing OrderDocument1 pageJadwal Purchasing OrderhusadaNo ratings yet
- Format Bacaan DR Verry SPJPDocument1 pageFormat Bacaan DR Verry SPJPhusadaNo ratings yet
- Electrochemistry: Voltaic Cells: Rezzan Hekmat AP Chemistry - 3 Pd. Lab Write UpDocument3 pagesElectrochemistry: Voltaic Cells: Rezzan Hekmat AP Chemistry - 3 Pd. Lab Write UpRezzan HekmatNo ratings yet
- Nptel - Ac.in Courses IIT-MADRAS Applied Thermodynamics Module 4 6 AsdcDocument4 pagesNptel - Ac.in Courses IIT-MADRAS Applied Thermodynamics Module 4 6 AsdcSanjeev PrakashNo ratings yet
- DX Evaporator Eng00013632 PDFDocument10 pagesDX Evaporator Eng00013632 PDFYaretiNo ratings yet
- Publ 5429Document2 pagesPubl 5429MahmoudNo ratings yet
- Nov 21st 2014 Friday: Products DetailsDocument1 pageNov 21st 2014 Friday: Products DetailsXuân Giang NguyễnNo ratings yet
- Nord BlocDocument220 pagesNord BlocAbdulNo ratings yet
- Observation of Quantum Corrections To Conductivity Up To Optical FrequenciesDocument8 pagesObservation of Quantum Corrections To Conductivity Up To Optical FrequenciesCarlos FazNo ratings yet
- Worksheet Phy 11Document10 pagesWorksheet Phy 11kcricketer75No ratings yet
- Cold Drawn PDFDocument1 pageCold Drawn PDFAna Emily PrentissNo ratings yet
- Tribological Behaviour of Aluminium Hybrid Metal Matrix CompositeDocument19 pagesTribological Behaviour of Aluminium Hybrid Metal Matrix CompositenisargaNo ratings yet
- IPTC-22235-MS Foams To Control Slugging Issues in Pipeline - From Lab To SimulationDocument9 pagesIPTC-22235-MS Foams To Control Slugging Issues in Pipeline - From Lab To SimulationLuky HendraningratNo ratings yet
- PDF Vibration Analysis Level 1 CompressDocument3 pagesPDF Vibration Analysis Level 1 CompressMohammad IkbalNo ratings yet
- GantryDocument7 pagesGantrysatydevsinghnegiNo ratings yet
- Imaging Techniques in Biomedical Engineering (Thermal Imaging)Document67 pagesImaging Techniques in Biomedical Engineering (Thermal Imaging)Karminder SinghNo ratings yet
- Basics of Pipe Stress Analysis A Presentation-Part 2 of 2Document6 pagesBasics of Pipe Stress Analysis A Presentation-Part 2 of 2iaftNo ratings yet
- Johnson Controls Central Plant Optimization 10 Application NoteDocument181 pagesJohnson Controls Central Plant Optimization 10 Application NotePradeep SukumaranNo ratings yet
- Incline AngleDocument17 pagesIncline AngleMuaz FadzilNo ratings yet
- Fabrication and Characteriation of P-N Junction DiodeDocument11 pagesFabrication and Characteriation of P-N Junction Diode12343567890No ratings yet
- Engine Lubrication & Cooling Systems: SectionDocument5 pagesEngine Lubrication & Cooling Systems: SectionGastonNo ratings yet
- Fiber OpticsDocument10 pagesFiber OpticsVishal Kumar ShawNo ratings yet
- (Astm Special Technical Publication - STP) John C. Monday, Timothy B. Shugart, Joseph A. Tamayo-Manual On Coating and Lining Methods For Cooling Water Systems in Power Plants-Astm Intl (1995) PDFDocument58 pages(Astm Special Technical Publication - STP) John C. Monday, Timothy B. Shugart, Joseph A. Tamayo-Manual On Coating and Lining Methods For Cooling Water Systems in Power Plants-Astm Intl (1995) PDFidigitiNo ratings yet
- 7 Review of Fundamentals - Heat and Mass TransferDocument20 pages7 Review of Fundamentals - Heat and Mass TransferPRASAD326100% (2)
- Training Manual TM2500Document499 pagesTraining Manual TM2500lunadogger90% (29)
- Lab Report Air ParticleDocument11 pagesLab Report Air ParticleSalmah AbasNo ratings yet
- ME463 Plate3 CapulDocument9 pagesME463 Plate3 CapulJuvy Lyka CapulNo ratings yet
- 01-Mi-Dti Cut Sheet 0715Document2 pages01-Mi-Dti Cut Sheet 0715Marvin EstradaNo ratings yet
- ASTM C990-01a Specification For Joints For Concrete Pipe, Manholes, and Precast Box Sections Using Preformed Flexible Joint Sealants.Document4 pagesASTM C990-01a Specification For Joints For Concrete Pipe, Manholes, and Precast Box Sections Using Preformed Flexible Joint Sealants.Liu ZhenguoNo ratings yet
- Grade3 3rd Q-ScienceDocument5 pagesGrade3 3rd Q-Scienceflower.power11233986No ratings yet
- Thermodynamics 1 Thermodynamics 1Document73 pagesThermodynamics 1 Thermodynamics 1Dinesh Pandian67% (3)
- Interpretation of DSC Curves in Polymer Analysis 2000 - ToledoDocument0 pagesInterpretation of DSC Curves in Polymer Analysis 2000 - ToledoyrecoverNo ratings yet