You might also like
- Recent Advances in The Treatment of ShockDocument52 pagesRecent Advances in The Treatment of ShockasupicuNo ratings yet
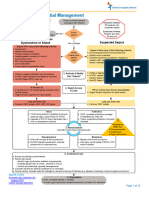
- Management Algorithm For Patients With Severe SepsisDocument1 pageManagement Algorithm For Patients With Severe SepsisgilankwibawaNo ratings yet
- SepsisDocument10 pagesSepsisJessa MaeNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- NRNP 6566 Week 4 Knowledge CheckDocument7 pagesNRNP 6566 Week 4 Knowledge Checkmary011danielNo ratings yet
- Tumor Lysis Oral Boards CasesDocument15 pagesTumor Lysis Oral Boards Casesczalesky66No ratings yet
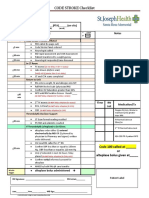
- Protocols Checklists Sepsis Alert Wesley HealthcareDocument1 pageProtocols Checklists Sepsis Alert Wesley HealthcareeryxspNo ratings yet
- SepsisDocument1 pageSepsisCharlie LeeNo ratings yet
- (Systemic Inflammatory Response Syndrome) : Norepinephrine Vasopressin or DopamineDocument2 pages(Systemic Inflammatory Response Syndrome) : Norepinephrine Vasopressin or DopaminejamesomooreNo ratings yet
- Dengue: History Physical Examination InvestigationDocument4 pagesDengue: History Physical Examination InvestigationNik Hanisah Zuraidi AfandiNo ratings yet
- Protocols ST Helens Adult Sepsis Management PathwayDocument1 pageProtocols ST Helens Adult Sepsis Management Pathwayputra purnomoNo ratings yet
- Mis C Clinical GuidelineDocument9 pagesMis C Clinical GuidelineasyqarNo ratings yet
- Mis C Clinical GuidelineDocument8 pagesMis C Clinical GuidelineClamargav aNo ratings yet
- SEPSIS Rev 21092020Document46 pagesSEPSIS Rev 21092020rani asfiyaNo ratings yet
- EGDT SepsisDocument8 pagesEGDT Sepsissiti fatmalaNo ratings yet
- The PatientDocument9 pagesThe PatientJan Crizza Dale R. FrancoNo ratings yet
- Lit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCDocument76 pagesLit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCKomang_JananuragaNo ratings yet
- Sepsis: ManagementDocument50 pagesSepsis: Managementer bcmNo ratings yet
- SEPSIS Early DetectionDocument35 pagesSEPSIS Early DetectionKomang_JananuragaNo ratings yet
- SepsisDocument3 pagesSepsisPhilip Poerworahjono100% (3)
- Evaluation and Diagnosis: New York State Department of HealthDocument2 pagesEvaluation and Diagnosis: New York State Department of HealthNisa Annisa ArfiyantiNo ratings yet
- NEONATOLOGYDocument8 pagesNEONATOLOGYmymamym100% (1)
- CURB-65 Score For Pneumonia Score DescriptionDocument14 pagesCURB-65 Score For Pneumonia Score DescriptionMelvin CarewNo ratings yet
- Cookeville Regional Medical Center Severe Sepsis/Septic Shock Clinical PathwayDocument4 pagesCookeville Regional Medical Center Severe Sepsis/Septic Shock Clinical PathwayArnelli HutagalungNo ratings yet
- Morning Report: Physician in ChargeDocument33 pagesMorning Report: Physician in ChargeIka AyuNo ratings yet
- The Intern Pocket Card Surviving GraysDocument2 pagesThe Intern Pocket Card Surviving GraysKathleen Grace ManiagoNo ratings yet
- Ecg PediaDocument2 pagesEcg PediaAdrian Ulu100% (1)
- Case Presentation On Supraventricular TachycardiaDocument64 pagesCase Presentation On Supraventricular TachycardiaHazel AsperaNo ratings yet
- Fluid Resuscitation in SepsisDocument68 pagesFluid Resuscitation in SepsisRonald Ariyanto WiradirnataNo ratings yet
- High Yield Surgery Compatible Version-2Document20 pagesHigh Yield Surgery Compatible Version-2zoozsuhai2No ratings yet
- CODE STROKE Checklist:: NotesDocument1 pageCODE STROKE Checklist:: NotesAdam MochtarNo ratings yet
- Case Scenario:: Is An Eye Finding Occurring Early inDocument5 pagesCase Scenario:: Is An Eye Finding Occurring Early inDenice Tamayo De GuzmanNo ratings yet
- From SIRS To Septic Shock (2022!01!22 00-25-28 UTC)Document1 pageFrom SIRS To Septic Shock (2022!01!22 00-25-28 UTC)Andrea AndradaNo ratings yet
- Shanz - Pedia Ii 2.04Document4 pagesShanz - Pedia Ii 2.04Petrina XuNo ratings yet
- STEMI Thrombolysis Protocol STElevation MIDocument6 pagesSTEMI Thrombolysis Protocol STElevation MISurya AtmajaNo ratings yet
- C. DiffDocument7 pagesC. DiffrNo ratings yet
- Sample Case ScenarioDocument8 pagesSample Case ScenarioJan Crizza Dale R. FrancoNo ratings yet
- High Yield Surgery Compatible Version PDFDocument20 pagesHigh Yield Surgery Compatible Version PDFSurgery CSC1No ratings yet
- Stemi Pathway: Record TimeDocument2 pagesStemi Pathway: Record TimeOlga Jadha CasmiraNo ratings yet
- 13.30 DR Arunraj Navaratnarajah - The Septic PatientDocument49 pages13.30 DR Arunraj Navaratnarajah - The Septic PatientagusNo ratings yet
- Februari, 22 Morning ReportDocument25 pagesFebruari, 22 Morning Reportnadia shabriNo ratings yet
- Post Arrest Hemodynamic OptDocument1 pagePost Arrest Hemodynamic OptMarinaJiménezNo ratings yet
- AKI Pathway (Nottingham University Hospitals April 2015)Document3 pagesAKI Pathway (Nottingham University Hospitals April 2015)Yadi SupriyadiNo ratings yet
- SYOK - Desi Surya IniDocument40 pagesSYOK - Desi Surya IniDesi Suryani DewiNo ratings yet
- Anak - Kasus 7 - Kelompok 7Document48 pagesAnak - Kasus 7 - Kelompok 7mehakNo ratings yet
- AUBF - MidtermsDocument14 pagesAUBF - MidtermsRomie Solacito100% (1)
- Sepsis in The Setting of AspleniaDocument30 pagesSepsis in The Setting of Aspleniaapi-740273867No ratings yet
- Haemorrhage ProtocolDocument1 pageHaemorrhage ProtocolHerwinda GeraldineNo ratings yet
- Resusitasi CairanDocument48 pagesResusitasi Cairanadi tiarmanNo ratings yet
- Sop NBNDocument55 pagesSop NBNSanthosh KumarNo ratings yet
- EGDT - PICU-NICU-Bandung-2016-DadangHDocument63 pagesEGDT - PICU-NICU-Bandung-2016-DadangHvillnachintyaNo ratings yet
- Case Study PDFDocument12 pagesCase Study PDFAngelica AdlawanNo ratings yet
- Post PCI Care When To ReferDocument25 pagesPost PCI Care When To ReferRahmat HidayatullahNo ratings yet
- Severe DengueDocument101 pagesSevere Denguetarakeeshbai1802No ratings yet
- Rhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Document10 pagesRhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Luis PadillaNo ratings yet
- Group Fdar Hemophilia ADocument2 pagesGroup Fdar Hemophilia AMika SaldañaNo ratings yet
- ECG How To InterpretDocument10 pagesECG How To InterpretMohamad DanialNo ratings yet
- Touch Imprint Cytology: A Rapid and Accurate Method For Diagnosis of Oral Cancer Original ArticleDocument19 pagesTouch Imprint Cytology: A Rapid and Accurate Method For Diagnosis of Oral Cancer Original ArticleNiketa SharmaNo ratings yet
- Strategies For Acute Metabolic DisordersDocument14 pagesStrategies For Acute Metabolic DisordersAhmed AnwarNo ratings yet
- Acute Pancreatitis PresentationDocument24 pagesAcute Pancreatitis PresentationhtmgNo ratings yet
- Lab Report 15438869 20231127064225Document1 pageLab Report 15438869 20231127064225carilloabhe21No ratings yet
- NARPAA E-Class Module 3 - Historical Definitions of AutismDocument19 pagesNARPAA E-Class Module 3 - Historical Definitions of AutismnarpaaNo ratings yet
- Lab Report Activity GlucoseDocument6 pagesLab Report Activity GlucoseTheodore LiwonganNo ratings yet
- Nursing Care Plan 2021-2022Document7 pagesNursing Care Plan 2021-2022AhmedGamalNo ratings yet
- SBAR Communication Form: and Progress NoteDocument3 pagesSBAR Communication Form: and Progress NoteTisa Meriel100% (1)
- Social Change Campaign in IndiaDocument7 pagesSocial Change Campaign in IndiaGauri GargNo ratings yet
- Axis I Clinical Psychiatric Disorders - LMM-1Document11 pagesAxis I Clinical Psychiatric Disorders - LMM-1richhuangNo ratings yet
- Mock Ospe Me211Document15 pagesMock Ospe Me211sahirbuleNo ratings yet
- 3.2 Dr. Taufin SpOT - Operating RoomDocument29 pages3.2 Dr. Taufin SpOT - Operating RoomTaqwatin Ma'rifahNo ratings yet
- Abatacept Hervey2006Document9 pagesAbatacept Hervey2006Calvin Tanuwijaya Stick BolaNo ratings yet
- Swedish Medical Center Patient LetterDocument2 pagesSwedish Medical Center Patient LetterMichael_Lee_RobertsNo ratings yet
- Jin Gui Shen QiDocument2 pagesJin Gui Shen QiJoana ValenteNo ratings yet
- Ap Lang Memoir EssayDocument13 pagesAp Lang Memoir Essayapi-305343417100% (1)
- Aplastic Anemia: Savita HandayaniDocument24 pagesAplastic Anemia: Savita HandayaniAnna Puteri GozaliNo ratings yet
- Cerebral CirculationDocument85 pagesCerebral CirculationCharles Nkurunziza100% (2)
- Teaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIDocument3 pagesTeaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIkasjdkasNo ratings yet
- Principles of Test Taking MTCDocument28 pagesPrinciples of Test Taking MTCMyk MacalintalNo ratings yet
- Introduction History Examination (Prosthodontics)Document37 pagesIntroduction History Examination (Prosthodontics)sarah0% (1)
- Humoral ImmunityDocument86 pagesHumoral ImmunitySinthiya KanesaratnamNo ratings yet
- Telegram@DrbooksDocument493 pagesTelegram@DrbooksDanh Nguyễn100% (3)
- Multi-Frequency and Multi-Component TympanometryDocument8 pagesMulti-Frequency and Multi-Component TympanometryEstudiantede FonoaudiologíaNo ratings yet
- Carevent Dra Rev 8-10-16Document2 pagesCarevent Dra Rev 8-10-16Adrian MorenoNo ratings yet
- Research Paper - Celiac DiseaseDocument5 pagesResearch Paper - Celiac Diseaseapi-316625517100% (1)
- Maternal and Child Health Programmes: MCH ServicesDocument10 pagesMaternal and Child Health Programmes: MCH ServicesRosebel LaguraNo ratings yet
- Dead Space ManagementDocument26 pagesDead Space ManagementIgnasNo ratings yet
- "The Man Who Mistook His Wife For Hat" Is ADocument9 pages"The Man Who Mistook His Wife For Hat" Is AIADT Psy50% (2)
- Rosh Review 11Document6 pagesRosh Review 11Sarwar BaigNo ratings yet