You might also like
- Study of Pediatric Congenital Cardiac Malformations by EchocardiographyDocument23 pagesStudy of Pediatric Congenital Cardiac Malformations by EchocardiographyRana Abd AlmugeethNo ratings yet
- Billiary SystemDocument60 pagesBilliary SystemDONALD UNASHENo ratings yet
- Bloom SyndromeDocument2 pagesBloom SyndromeDrMubashir ShaikhNo ratings yet
- Reproduction System 1Document48 pagesReproduction System 1SITI AISYAHNo ratings yet
- Vascular Vascular: Medicine (ST George's Hospital Medical School) Medicine (ST George's Hospital Medical School)Document7 pagesVascular Vascular: Medicine (ST George's Hospital Medical School) Medicine (ST George's Hospital Medical School)shravaniNo ratings yet
- Ultrasonography Assessment of Lower Limb VeinsDocument49 pagesUltrasonography Assessment of Lower Limb VeinsPutra AchmadNo ratings yet
- Congenital Anomalies of Kidney and Urinary TractDocument53 pagesCongenital Anomalies of Kidney and Urinary TractDoctor peds100% (1)
- Ultrasound: Made By: Conny LeoDocument15 pagesUltrasound: Made By: Conny LeoChristabelle ConnyNo ratings yet
- Pancreas and SpleenDocument44 pagesPancreas and SpleenOgbuefi PascalNo ratings yet
- Moderator: Mr. Ram Singh Lecturer Department of Radiodiagnosis and Imaging PGIMER, ChandigarhDocument87 pagesModerator: Mr. Ram Singh Lecturer Department of Radiodiagnosis and Imaging PGIMER, ChandigarhMunish DograNo ratings yet
- ULTRASOUND Fetal AnomaliesdocxDocument86 pagesULTRASOUND Fetal AnomaliesdocxAlexandra MateiNo ratings yet
- CXR Lecture DR Lenora FernandezDocument70 pagesCXR Lecture DR Lenora Fernandezapi-19431894100% (1)
- Cyanosis in The NewbornDocument32 pagesCyanosis in The Newbornimma_2014No ratings yet
- Radiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDocument100 pagesRadiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDiana OCtavinaNo ratings yet
- Abdominal Trauma - 0Document129 pagesAbdominal Trauma - 0Tan DanNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnNo ratings yet
- Approach in Lymphadenopathy in ChildrenDocument14 pagesApproach in Lymphadenopathy in Childrennahiry100% (1)
- Radiology of The AbdomenDocument19 pagesRadiology of The AbdomenShaktisila FatrahadyNo ratings yet
- Atelektasis: Penyaji: Martvera SDocument20 pagesAtelektasis: Penyaji: Martvera Saidil ilham100% (1)
- BCBR - Review + Cycle 3Document103 pagesBCBR - Review + Cycle 3Dr. Richa Choudhary89% (9)
- Pulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesDocument5 pagesPulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesIJAR JOURNALNo ratings yet
- The Chemistry of Copper: Number 83 WWW - Curriculum-Press - Co.ukDocument5 pagesThe Chemistry of Copper: Number 83 WWW - Curriculum-Press - Co.uks7076728g100% (1)
- Interpreting The Chest Radio Graph Friendly)Document9 pagesInterpreting The Chest Radio Graph Friendly)Vagner BorgesNo ratings yet
- 2019 Sec 4 Pure Chemistry SA2 Anderson SecondaryDocument65 pages2019 Sec 4 Pure Chemistry SA2 Anderson SecondaryChloe Tang KYNo ratings yet
- 3 Abdominal Ultrasound Imaging AnatomyDocument7 pages3 Abdominal Ultrasound Imaging Anatomyjefaturaimagenologia Hospital NogalarNo ratings yet
- DORVDocument33 pagesDORVjayasiinputNo ratings yet
- Critical Case in Congenital Heart Disease, What's The Sign and Initial Treatment For Them (Prof. Dr. Dr. Mulyadi M.djer, SpA (K) )Document69 pagesCritical Case in Congenital Heart Disease, What's The Sign and Initial Treatment For Them (Prof. Dr. Dr. Mulyadi M.djer, SpA (K) )tyesNo ratings yet
- 14 - Barium Studies For GIT With NotesDocument50 pages14 - Barium Studies For GIT With NotesSunil ThomasNo ratings yet
- PrediabetesDocument8 pagesPrediabetesVimal NishadNo ratings yet
- Pediatrics ECG by DR Ali Bel KheirDocument9 pagesPediatrics ECG by DR Ali Bel KheirFerasNo ratings yet
- Diagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020Document16 pagesDiagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- Cystic Adenomatoid Malformation (CAM)Document38 pagesCystic Adenomatoid Malformation (CAM)Aliyah Tofani PawelloiNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Chapter 2 - FIR Filters - Digital Filter Design - Mikroelektronika PDFDocument114 pagesChapter 2 - FIR Filters - Digital Filter Design - Mikroelektronika PDFAnimesh NagrareNo ratings yet
- Atrial Septial DefectDocument22 pagesAtrial Septial DefectJulie MckinneyNo ratings yet
- Approach To A Child With Cough and Difficulty in BreathingDocument23 pagesApproach To A Child With Cough and Difficulty in BreathingKashif Burki100% (2)
- Sickle Cell Anemia PowerpointDocument29 pagesSickle Cell Anemia Powerpointapi-263353704100% (1)
- HERNIADocument34 pagesHERNIAAtiqah ShahNo ratings yet
- Uroflowmetry InterpretationDocument4 pagesUroflowmetry InterpretationMeryl PulcheriaNo ratings yet
- Ccam N Bps Management PDFDocument9 pagesCcam N Bps Management PDFEthan AmalNo ratings yet
- Congenital Heart DiseaseDocument74 pagesCongenital Heart DiseaseKeith LajotNo ratings yet
- Diagnosis and Management of The Neonate With Critical Congenital Heart DiseaseDocument35 pagesDiagnosis and Management of The Neonate With Critical Congenital Heart Diseasemotzco0% (1)
- L-R ShuntDocument88 pagesL-R ShuntnanohaniwiekoNo ratings yet
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Atls Approach To Pediatric TraumaDocument8 pagesAtls Approach To Pediatric TraumaMakoto KyogokuNo ratings yet
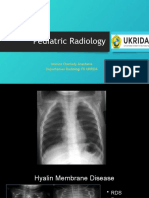
- Pediatric Radiology: Monica Cherlady Anastasia Departemen Radiologi FK UKRIDADocument23 pagesPediatric Radiology: Monica Cherlady Anastasia Departemen Radiologi FK UKRIDARoni HirewakeNo ratings yet
- AP WindowDocument13 pagesAP WindowHugo GonzálezNo ratings yet
- Radiologi Kasus DigestifDocument110 pagesRadiologi Kasus DigestifarifgteguhNo ratings yet
- Chest X - Rays in Pediatric CardiologyDocument8 pagesChest X - Rays in Pediatric CardiologyAimhigh_PPMNo ratings yet
- Clinical ExDocument123 pagesClinical ExDeepti ChaharNo ratings yet
- Chest ExaminationDocument14 pagesChest Examinationsajad abasewNo ratings yet
- Chest Radiology For DummiesDocument6 pagesChest Radiology For DummiesTom MallinsonNo ratings yet
- AsdaDocument42 pagesAsdaratchagarajaNo ratings yet
- Pediatric X RaysDocument88 pagesPediatric X RaysprinceejNo ratings yet
- X Ray PediatricsDocument13 pagesX Ray PediatricsMobin Ur Rehman KhanNo ratings yet
- OSCE Checklist Newborn Baby Assessment NIPEDocument3 pagesOSCE Checklist Newborn Baby Assessment NIPETauqeer Ahmed0% (1)
- DR Lily - Resp Distress in Newborn Infants PDFDocument45 pagesDR Lily - Resp Distress in Newborn Infants PDFM Ilham MNo ratings yet
- Disorder of Sex DevelopmentDocument40 pagesDisorder of Sex DevelopmentAndi AdityaNo ratings yet
- Toacs 7Document208 pagesToacs 7Mobin Ur Rehman Khan100% (1)
- Pediatric RadiologyDocument59 pagesPediatric RadiologyNguyễn Tiến ĐồngNo ratings yet
- MediastiniumDocument25 pagesMediastiniumahmedzakaria0No ratings yet
- Bones Anatomy: Wiki RadiographyDocument59 pagesBones Anatomy: Wiki RadiographyniputusellyowNo ratings yet
- Vimal PAD - SlidesDocument53 pagesVimal PAD - SlidesVimal NishadNo ratings yet
- ARRYHTHMIADocument122 pagesARRYHTHMIAVimal NishadNo ratings yet
- pm0150 LooksteinRobert Debulki MondayDocument27 pagespm0150 LooksteinRobert Debulki MondayVimal NishadNo ratings yet
- European J of Heart Fail - 2022 - Guazzi - Exercise Testing in Heart Failure With Preserved Ejection Fraction An AppraisalDocument19 pagesEuropean J of Heart Fail - 2022 - Guazzi - Exercise Testing in Heart Failure With Preserved Ejection Fraction An AppraisalVimal NishadNo ratings yet
- Heart Sounds S2Document31 pagesHeart Sounds S2Vimal NishadNo ratings yet
- Hipertensión Pulmonar (2022)Document114 pagesHipertensión Pulmonar (2022)Mauricio CabreraNo ratings yet
- Merchant 2019Document7 pagesMerchant 2019Vimal NishadNo ratings yet
- Mcqs in Cardiology Based On Braunwald by Dr. Adithya Udupa K Aortic Valve DiseaseDocument25 pagesMcqs in Cardiology Based On Braunwald by Dr. Adithya Udupa K Aortic Valve DiseaseVimal NishadNo ratings yet
- Seminar TopicsDocument4 pagesSeminar TopicsVimal NishadNo ratings yet
- Index of Microcirculatory Resistance:: The BasicsDocument54 pagesIndex of Microcirculatory Resistance:: The BasicsVimal NishadNo ratings yet
- Medicine Emergency ChartsDocument1 pageMedicine Emergency ChartsVimal NishadNo ratings yet
- Transcatheter Therapies For Valvular Heart DiseaseDocument10 pagesTranscatheter Therapies For Valvular Heart DiseaseVimal NishadNo ratings yet
- Assessment of Glycemic Status, Insulin Resistance and HypogonadismDocument5 pagesAssessment of Glycemic Status, Insulin Resistance and HypogonadismVimal NishadNo ratings yet
- Questions On The Kidney and Urinary Tract-2Document7 pagesQuestions On The Kidney and Urinary Tract-2Vimal NishadNo ratings yet
- Assessment of Glycemic Status, Insulin Resistance and HypogonadismDocument5 pagesAssessment of Glycemic Status, Insulin Resistance and HypogonadismVimal NishadNo ratings yet
- Evaluation of EndotheliumDocument3 pagesEvaluation of EndotheliumVimal NishadNo ratings yet
- 12 OA Evaluation of Febrile Thrombocytopenia CasesDocument5 pages12 OA Evaluation of Febrile Thrombocytopenia CasesVimal NishadNo ratings yet
- Mod Rhuematic Fever Final PDFDocument90 pagesMod Rhuematic Fever Final PDFVimal NishadNo ratings yet
- Towards Developing A Scoring System For Febrile ThrombocytopeniaDocument5 pagesTowards Developing A Scoring System For Febrile ThrombocytopeniaVimal NishadNo ratings yet
- CardiologyDocument29 pagesCardiologyVimal NishadNo ratings yet
- Fluid and ElectrolyteDocument6 pagesFluid and ElectrolyteVimal NishadNo ratings yet
- TBM 1Document2 pagesTBM 1Vimal NishadNo ratings yet
- Mesna PM ENG v4.0 011218Document23 pagesMesna PM ENG v4.0 011218Vimal NishadNo ratings yet
- PDFDocument1 pagePDFVimal NishadNo ratings yet
- Neet As OrderDocument1 pageNeet As OrderVimal NishadNo ratings yet
- 483 PDFDocument6 pages483 PDFVimal NishadNo ratings yet
- Neurophysiology Quiz Oct 03Document3 pagesNeurophysiology Quiz Oct 03Vimal NishadNo ratings yet
- S 5359 LBLDocument58 pagesS 5359 LBLNidershan SuguneshwaranNo ratings yet
- Hyperlogic Heavy Metal 120x60 Skid System Quick Start Installation InstructionsDocument17 pagesHyperlogic Heavy Metal 120x60 Skid System Quick Start Installation Instructionsapi-247828287No ratings yet
- 21 10 26 Tastytrade ResearchDocument7 pages21 10 26 Tastytrade ResearchCSNo ratings yet
- Definitions - Topic 9 The Periodic Table - CAIE Chemistry IGCSE PDFDocument1 pageDefinitions - Topic 9 The Periodic Table - CAIE Chemistry IGCSE PDFAtif BakhshNo ratings yet
- Cooling Solutions About UsDocument18 pagesCooling Solutions About UsBlender RemixNo ratings yet
- REVIEW TASK 1 - Capitalization, Punctuation, Fragments, Run-On Sentences and Subject & Verb Agreement Review (-1Document2 pagesREVIEW TASK 1 - Capitalization, Punctuation, Fragments, Run-On Sentences and Subject & Verb Agreement Review (-1Johao DoradoNo ratings yet
- Practical Exercise 02Document17 pagesPractical Exercise 02FeRro ReniNo ratings yet
- UserDocument150 pagesUserRahul ShardhaNo ratings yet
- Surge Arresters: Selection, Application and Testing: Pass YouDocument30 pagesSurge Arresters: Selection, Application and Testing: Pass YouOoi Ban JuanNo ratings yet
- Supplemental Activity 1Document2 pagesSupplemental Activity 1Angelika DomondonNo ratings yet
- Examples S-Convex FunctionsDocument7 pagesExamples S-Convex Functionstradutora100% (2)
- Gauss Contest: Grade 7Document4 pagesGauss Contest: Grade 7irwan syahNo ratings yet
- Analog Communications-Notes PDFDocument110 pagesAnalog Communications-Notes PDFjyothimunjam100% (1)
- Samsung Scala2-Amd r1.0 SchematicsDocument55 pagesSamsung Scala2-Amd r1.0 SchematicsJunioNo ratings yet
- K Type Thermocouple Extension Cable KXYY (1-50) Pairs X 1.5 MM 300 VDocument1 pageK Type Thermocouple Extension Cable KXYY (1-50) Pairs X 1.5 MM 300 VArthurNo ratings yet
- Ready To Use Therapeutic Food in RwandaDocument25 pagesReady To Use Therapeutic Food in RwandaKABERA RENENo ratings yet
- AC Commutator Motors Repulsion Series Motor UniversalDocument3 pagesAC Commutator Motors Repulsion Series Motor UniversalwhrferNo ratings yet
- ADAT Optical Audio Data Generator and Encoder V1401Document8 pagesADAT Optical Audio Data Generator and Encoder V1401mylitalindaNo ratings yet
- Mark Scheme: June 2018Document12 pagesMark Scheme: June 2018BethanyNo ratings yet
- DD210-V 9604sb PDFDocument4 pagesDD210-V 9604sb PDFBrandon MoralesNo ratings yet
- Aerodyn2 Discussion 11 Ceilings Ant Time To ClimbDocument26 pagesAerodyn2 Discussion 11 Ceilings Ant Time To Climbshop printNo ratings yet
- Optimization Technique Group 1Document60 pagesOptimization Technique Group 1jmlafortezaNo ratings yet
- AirCheck Detail Report - PK8AP01Document116 pagesAirCheck Detail Report - PK8AP01Trion Ragil NugrohoNo ratings yet
- Sapmm - Spro .Path SettingsDocument2 pagesSapmm - Spro .Path SettingsVijay AnandNo ratings yet
- 0w 30 Yağ ÖzellikleriDocument2 pages0w 30 Yağ ÖzellikleriahmetNo ratings yet
- Norma JIC 37Document36 pagesNorma JIC 37guguimirandaNo ratings yet
- LAMIGAS - BSN2H-Laboratory No. 2Document3 pagesLAMIGAS - BSN2H-Laboratory No. 2Juliemae LamigasNo ratings yet
- Properties of LiOH and LiNO3 Aqueous SolutionsDocument13 pagesProperties of LiOH and LiNO3 Aqueous Solutionstim tengNo ratings yet