You might also like
- University of Michigan Surgery Oral Exam ReviewDocument21 pagesUniversity of Michigan Surgery Oral Exam ReviewSharad Patel100% (2)
- BTK Quick Hits Final PDFDocument24 pagesBTK Quick Hits Final PDFcusom34No ratings yet
- Surgery BoardsDocument16 pagesSurgery Boardscusom34100% (1)
- BTK Quick Hits Final PDFDocument24 pagesBTK Quick Hits Final PDFcusom34No ratings yet
- Pharmaceutical CareDocument114 pagesPharmaceutical CareRisdaFitriaNo ratings yet
- Wing 1981 AspergerDocument15 pagesWing 1981 Asperger__aguNo ratings yet
- Tomatoes and Tomato Products - Nutritional, Medicinal and Therapeutic PropertiesDocument664 pagesTomatoes and Tomato Products - Nutritional, Medicinal and Therapeutic PropertiesAndreea MerţNo ratings yet
- Hamdi, JPRAS2006Document9 pagesHamdi, JPRAS2006Zouzou YuNo ratings yet
- Reconstruction of The Skin Defect of The Knee Using A Reverse Anterolateral Thigh Island FlapDocument4 pagesReconstruction of The Skin Defect of The Knee Using A Reverse Anterolateral Thigh Island FlapAndrea Del VillarNo ratings yet
- Chimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Document10 pagesChimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Manny TrujilloNo ratings yet
- Lymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019Document4 pagesLymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019yeapdshengNo ratings yet
- 2015 AltDocument11 pages2015 Altplay259No ratings yet
- BibliographyDocument6 pagesBibliographysuryaNo ratings yet
- The Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic ReconstrDocument8 pagesThe Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic Reconstrydk sinhNo ratings yet
- Tang 2010Document5 pagesTang 2010Elena ShekaNo ratings yet
- Triangular Fiibrocartilage Complex: Anatomico-Clinical CorrelationsDocument7 pagesTriangular Fiibrocartilage Complex: Anatomico-Clinical CorrelationsPaula BautistaNo ratings yet
- Techniques in Hand and Amp Upper ExtremiDocument6 pagesTechniques in Hand and Amp Upper ExtremiSotiris PlakoutsisNo ratings yet
- Foramen Huschke PatologicoDocument7 pagesForamen Huschke PatologicoLM AdrianneNo ratings yet
- 1 s2.0 S2352587814000060 MainDocument5 pages1 s2.0 S2352587814000060 MainjikhNo ratings yet
- Ross OtoHNS2005 ArterialCouplingDocument5 pagesRoss OtoHNS2005 ArterialCouplingSungjin SongNo ratings yet
- The Anatomy of The Musculocutaneous Latissumus Dorsi Flap For Neophalloplasty - Dennis Et Al - Clinical Anatomy (2018)Document8 pagesThe Anatomy of The Musculocutaneous Latissumus Dorsi Flap For Neophalloplasty - Dennis Et Al - Clinical Anatomy (2018)jean.josytbNo ratings yet
- Visweswar Bhattacharya, Rajesh Kumar WattsDocument6 pagesVisweswar Bhattacharya, Rajesh Kumar WattsViswanath_Poli_2693No ratings yet
- Revisiting The Surgical Anatomy of The Triangle of Doom and The Triangle of PainDocument7 pagesRevisiting The Surgical Anatomy of The Triangle of Doom and The Triangle of PainLITTLESWEETKILLERNo ratings yet
- Clinical StudyDocument6 pagesClinical StudyHendra JurbonNo ratings yet
- Andrade 2018Document6 pagesAndrade 2018Fausto Fernandes de CastroNo ratings yet
- Fai 2011 0818Document4 pagesFai 2011 0818Mohamed GoudaNo ratings yet
- Early Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessDocument6 pagesEarly Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessJohannes CordeNo ratings yet
- Optimizing Survival of Large Fibula Osteocutaneous Flaps For Extensive Full-Thickness Oromandibular Defects. A Two-Stage Approach With Temporary Orocutaneous FistulaDocument7 pagesOptimizing Survival of Large Fibula Osteocutaneous Flaps For Extensive Full-Thickness Oromandibular Defects. A Two-Stage Approach With Temporary Orocutaneous FistulaAlvaro rivero calleNo ratings yet
- Pi Is 1079210402000458Document7 pagesPi Is 1079210402000458Sanjay RinaNo ratings yet
- A Rare Anatomical Variation in The Pedicle of Anterolateral Thigh (ALT) FlapDocument3 pagesA Rare Anatomical Variation in The Pedicle of Anterolateral Thigh (ALT) FlapLukesh PatilNo ratings yet
- 1 s2.0 S1010518216000652 Main PDFDocument9 pages1 s2.0 S1010518216000652 Main PDFRoberto AmayaNo ratings yet
- Acute ScrotumDocument15 pagesAcute ScrotumakreditasirsurNo ratings yet
- Shape and Volume of Craniofacial Cavities in Intentional Skull DeformationsDocument10 pagesShape and Volume of Craniofacial Cavities in Intentional Skull DeformationsGastón SalasNo ratings yet
- Selecting A Free Flap For Soft Tissue Coverage in Lower ExtremityDocument8 pagesSelecting A Free Flap For Soft Tissue Coverage in Lower ExtremityMuhammad RifkiNo ratings yet
- 010 - Hand FlapsDocument20 pages010 - Hand FlapsJayNo ratings yet
- Transporte Oseo Postinfeccion en TibiaDocument7 pagesTransporte Oseo Postinfeccion en TibiaSusan Ly VillalobosNo ratings yet
- Reconstruction of Groin Defects Following Radical Inguinal Lymphadenectomy: An Evidence Based ReviewDocument9 pagesReconstruction of Groin Defects Following Radical Inguinal Lymphadenectomy: An Evidence Based ReviewamdreyNo ratings yet
- Medicine The American Journal of SportsDocument8 pagesMedicine The American Journal of Sportshieuminhduong7No ratings yet
- Development of A Mouse Model of Supraspinatus Tendon Insertion Site HealingDocument8 pagesDevelopment of A Mouse Model of Supraspinatus Tendon Insertion Site Healingatika5No ratings yet
- Hindquarter IJOCDocument4 pagesHindquarter IJOCRyanAdnaniNo ratings yet
- Treatment of Ischial Pressure Sores With Both Profunda Femoris Artery Perforator Flaps and Muscle FlapsDocument7 pagesTreatment of Ischial Pressure Sores With Both Profunda Femoris Artery Perforator Flaps and Muscle FlapsIntan Permata WNo ratings yet
- Burger Et Al 2002 Abdominal Incisions Techniques and Postoperative ComplicationsDocument7 pagesBurger Et Al 2002 Abdominal Incisions Techniques and Postoperative ComplicationsagengbsNo ratings yet
- Autoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSDocument5 pagesAutoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSVillateAngelaNo ratings yet
- Fractures of The Talus Current ConceptsDocument10 pagesFractures of The Talus Current ConceptsBalsam TeineNo ratings yet
- Cincinnati 11Document4 pagesCincinnati 11eugenemukeba71No ratings yet
- Malata 2006Document7 pagesMalata 2006Female calmNo ratings yet
- Combined Massive Allograft and Intramedullary Vascularized Fibula Transfer The Capanna Technique For Treatment of Congenital Pseudarthrosis of TheDocument7 pagesCombined Massive Allograft and Intramedullary Vascularized Fibula Transfer The Capanna Technique For Treatment of Congenital Pseudarthrosis of TheHenrique NetoNo ratings yet
- J ArthrnjknliDocument10 pagesJ ArthrnjknliJahid HasanNo ratings yet
- Article PDFDocument9 pagesArticle PDFAqsa FarooqNo ratings yet
- Basics of Elbow Arthroscopy Part I: Surface Anatomy, Portals, and Structures at RiskDocument5 pagesBasics of Elbow Arthroscopy Part I: Surface Anatomy, Portals, and Structures at RiskMoustafa MohamedNo ratings yet
- 06 Traboulsi-Garet 등 - 2021 - Influence of Different Incision Designs on Flap ExDocument7 pages06 Traboulsi-Garet 등 - 2021 - Influence of Different Incision Designs on Flap Exsupercool0120No ratings yet
- Management and Aesthetic Results of Support Grafts in Saddle Nose SurgeryDocument6 pagesManagement and Aesthetic Results of Support Grafts in Saddle Nose SurgeryAndy HongNo ratings yet
- The Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegDocument7 pagesThe Proximally Based Sural Artery Flap For Coverage of Soft Tissue Defects Around The Knee and On The Proximal Third and Middle Third of The Lower LegMarco Antonio MiraveteNo ratings yet
- Ann Burns and Fire Disasters 29 209Document6 pagesAnn Burns and Fire Disasters 29 209fabian hernandez medinaNo ratings yet
- Total Knee Arthroplasty For Severe Valgus Deformity: J Bone Joint Surg AmDocument15 pagesTotal Knee Arthroplasty For Severe Valgus Deformity: J Bone Joint Surg AmAbdiel NgNo ratings yet
- Jena 2015Document3 pagesJena 2015amdreyNo ratings yet
- Aps 39 345Document9 pagesAps 39 345isabelNo ratings yet
- The Chertsey Classification of Tibial Plateau FracDocument2 pagesThe Chertsey Classification of Tibial Plateau FracWahyuu N PutraNo ratings yet
- Protesis 15Document9 pagesProtesis 15ana márquezNo ratings yet
- Anterior Anterolateral Posterior App Advantages DisadvantagesDocument8 pagesAnterior Anterolateral Posterior App Advantages Disadvantagesmuhammad bayu wicaksonoNo ratings yet
- ENDOSCOPIC Alto RiesgoDocument5 pagesENDOSCOPIC Alto RiesgoIgnacio ToledoNo ratings yet
- Aortaresektion Marulli 2015Document6 pagesAortaresektion Marulli 2015t.krbekNo ratings yet
- 05 CastelnuovoDocument7 pages05 Castelnuovogabriele1977No ratings yet
- TRIGONOMETRIADocument7 pagesTRIGONOMETRIACatalina RodríguezNo ratings yet
- Nakama 2005Document7 pagesNakama 2005angelica barrazaNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- Spinal Tumor Surgery: A Case-Based ApproachFrom EverandSpinal Tumor Surgery: A Case-Based ApproachDaniel M. SciubbaNo ratings yet
- Efficacy of Anti-Interleukin-1 Receptor Antagonist Anakinra (Kineret of Refractory Sweet's SyndromeDocument5 pagesEfficacy of Anti-Interleukin-1 Receptor Antagonist Anakinra (Kineret of Refractory Sweet's Syndromecusom34No ratings yet
- Microsurgery ArticleDocument6 pagesMicrosurgery Articlecusom34No ratings yet
- Investigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake FunctionDocument3 pagesInvestigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake Functioncusom34No ratings yet
- Synpor Synthes Porous Polyethylene Implant: Surgical TechniqueDocument16 pagesSynpor Synthes Porous Polyethylene Implant: Surgical Techniquecusom34No ratings yet
- Rhinplasty For Adult Cleft Lip Nasal Deformity PDFDocument26 pagesRhinplasty For Adult Cleft Lip Nasal Deformity PDFcusom34No ratings yet
- Head and Neck Free - Ap Reconstruction in The Elderly: E.E.M. NaoDocument5 pagesHead and Neck Free - Ap Reconstruction in The Elderly: E.E.M. Naocusom34No ratings yet
- Bike It Map Gap WebDocument2 pagesBike It Map Gap Webcusom34No ratings yet
- Testosterone SummaryDocument35 pagesTestosterone Summarycusom34No ratings yet
- Study of Neurovascular Anatomy of The Split Gracilis Facial ReanimaitonDocument9 pagesStudy of Neurovascular Anatomy of The Split Gracilis Facial Reanimaitoncusom34No ratings yet
- Aging Neck ManagementDocument10 pagesAging Neck Managementcusom34No ratings yet
- Autologous Fat Grafting - Harvesting Techniques PDFDocument7 pagesAutologous Fat Grafting - Harvesting Techniques PDFcusom34No ratings yet
- Autologous Fat Grafting - Harvesting Techniques PDFDocument7 pagesAutologous Fat Grafting - Harvesting Techniques PDFcusom34No ratings yet
- Rhinplasty For Adult Cleft Lip Nasal Deformity PDFDocument26 pagesRhinplasty For Adult Cleft Lip Nasal Deformity PDFcusom34No ratings yet
- Anatomical Basis of The Posterior Brachial Skin Flap: SummaryDocument6 pagesAnatomical Basis of The Posterior Brachial Skin Flap: Summarycusom34No ratings yet
- Nose and Lips Graft Variants A Subunit Anatomical StudyDocument30 pagesNose and Lips Graft Variants A Subunit Anatomical Studycusom34No ratings yet
- Pediatric PatientDocument29 pagesPediatric Patientcusom34No ratings yet
- Pediatric PatientDocument29 pagesPediatric Patientcusom34No ratings yet
- Original1.Chapter 53 Surgical Complications of Cirrhosis and Portal HypertensionDocument23 pagesOriginal1.Chapter 53 Surgical Complications of Cirrhosis and Portal Hypertensioncusom34No ratings yet
- Facial Reanimation With Masseter Nerve-Innervated Free Gracilis Muscle Transfer in Established Facial Palsy PatientsDocument7 pagesFacial Reanimation With Masseter Nerve-Innervated Free Gracilis Muscle Transfer in Established Facial Palsy Patientscusom34No ratings yet
- Anatomically Based Breast Augmentation: A 6-Plane Autologous ApproachDocument2 pagesAnatomically Based Breast Augmentation: A 6-Plane Autologous Approachcusom34No ratings yet
- Breast Reconstruction With Free Anterolateral Thigh FlapDocument6 pagesBreast Reconstruction With Free Anterolateral Thigh Flapcusom34No ratings yet
- ABSITE High YieldDocument2 pagesABSITE High Yieldcusom34100% (2)
- Indications and Cont in Total Breast Reconstruction With LipomodelingDocument7 pagesIndications and Cont in Total Breast Reconstruction With Lipomodelingcusom34No ratings yet
- Early Ambulation After Microsurgical Reconstruction of The Lower ExtremityDocument3 pagesEarly Ambulation After Microsurgical Reconstruction of The Lower Extremitycusom34No ratings yet
- Breast Reconstruction With Free Anterolateral Thigh FlapDocument5 pagesBreast Reconstruction With Free Anterolateral Thigh Flapcusom34No ratings yet
- Wa0003Document4 pagesWa0003YegaNo ratings yet
- Depresia PostpartumDocument18 pagesDepresia PostpartumIonela BogdanNo ratings yet
- Bivalirudin Anticoagulant1Document6 pagesBivalirudin Anticoagulant1walid hassanNo ratings yet
- Clavicle and Sternoclavicular JointDocument14 pagesClavicle and Sternoclavicular JointChavdarNo ratings yet
- 常用詞彙表Document10 pages常用詞彙表GXNo ratings yet
- Cardiocare 2000 Operation ManualDocument61 pagesCardiocare 2000 Operation ManualDokter MoezNo ratings yet
- REV #5 - Introduction To GeneticsDocument3 pagesREV #5 - Introduction To GeneticsCatalytic AintNo ratings yet
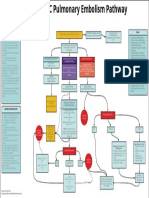
- EMCrit Lae Pulmonary FlowDocument1 pageEMCrit Lae Pulmonary FlowhmsptrNo ratings yet
- 9 Dissacharides Metabolism Compatibility ModeDocument16 pages9 Dissacharides Metabolism Compatibility ModeAubrey Nativity Ostulano YangzonNo ratings yet
- ASV GalileoDocument43 pagesASV GalileoalvyandaniNo ratings yet
- Long Term Follow Up After Admin Human GT Products - Jan - 2020Document37 pagesLong Term Follow Up After Admin Human GT Products - Jan - 2020DNo ratings yet
- A2 - Practice 29Document2 pagesA2 - Practice 29123VinhcuuNo ratings yet
- Artikel Bahasa Inggris Tentang Kesehatan LingkunganDocument2 pagesArtikel Bahasa Inggris Tentang Kesehatan LingkunganYolanda SefraniNo ratings yet
- Free Class Asclepio Metabolic SyndromeDocument6 pagesFree Class Asclepio Metabolic SyndromeJames BudiantoNo ratings yet
- Overview of AntibioticsDocument5 pagesOverview of AntibioticsakshahinbdNo ratings yet
- Gen Bio 2 Q4 Module 4Document25 pagesGen Bio 2 Q4 Module 4Shoto TodorokiNo ratings yet
- Chordoma Current Concepts Management and Future DirectionsDocument8 pagesChordoma Current Concepts Management and Future DirectionsChristian AdeNo ratings yet
- 1 s2.0 S240589632201374X MainDocument6 pages1 s2.0 S240589632201374X MainApollonia VitelliNo ratings yet
- Analytical Exposition Text For Advanced ReadingDocument8 pagesAnalytical Exposition Text For Advanced ReadingBambang SatoNo ratings yet
- 9721 Smoking Cessaton Newsletter 1981Document8 pages9721 Smoking Cessaton Newsletter 1981Julia PurperaNo ratings yet
- RRL LocalinternationalDocument11 pagesRRL LocalinternationalkdfhjfhfNo ratings yet
- Guía Manejo Del Shock 2023Document67 pagesGuía Manejo Del Shock 2023Alvaro ArriagadaNo ratings yet
- Palliative Care Pain and Symptom Control GuidelinesDocument128 pagesPalliative Care Pain and Symptom Control GuidelinesAQSA AHMED SIDDIQUINo ratings yet
- Copd Action Plan PDFDocument2 pagesCopd Action Plan PDFdtech2No ratings yet
- Inles 4Document2 pagesInles 4Astrid CruzNo ratings yet
- Nicu ReportDocument66 pagesNicu ReportEr Shah Rukh QadriNo ratings yet
- CT/MRI Ordering Guide: Body Part Signs/Symptoms Exam To OrderDocument2 pagesCT/MRI Ordering Guide: Body Part Signs/Symptoms Exam To OrderCourtNo ratings yet