You might also like
- Oral Contrast CinDocument6 pagesOral Contrast CinTommy TunggamoroNo ratings yet
- Contrast Induced NephropathyDocument2 pagesContrast Induced NephropathySri HariNo ratings yet
- CIN Consensus StrategiesDocument19 pagesCIN Consensus StrategiesThomas PhilipNo ratings yet
- Open 2015 ZhangDocument13 pagesOpen 2015 ZhangadsfadfasdNo ratings yet
- Contrast Induced Nephropathy: September 2007Document12 pagesContrast Induced Nephropathy: September 2007usmanmekanNo ratings yet
- New Insight Into Cerebrovascular Diseases - An Updated Comprehensive ReviewDocument25 pagesNew Insight Into Cerebrovascular Diseases - An Updated Comprehensive ReviewNguyễn PhúcNo ratings yet
- Contrast-Induced Nephropathy: Evidence SummaryDocument5 pagesContrast-Induced Nephropathy: Evidence SummaryDenataNo ratings yet
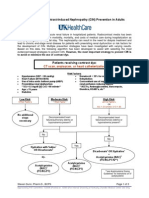
- Prevention of Contrast-Induced Nephropathy (CIN) in Interventional Radiology PracticeDocument12 pagesPrevention of Contrast-Induced Nephropathy (CIN) in Interventional Radiology PracticeReioctabianoNo ratings yet
- IKD6 - Contrast Associated AKIDocument44 pagesIKD6 - Contrast Associated AKIRenal Association MauritiusNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- 16111-Article Text-58468-1-10-20130807Document8 pages16111-Article Text-58468-1-10-20130807Dr. TomNo ratings yet
- Falla Renal 2011Document8 pagesFalla Renal 2011Mattya SalazarNo ratings yet
- Contrast Induced NephropathyDocument25 pagesContrast Induced NephropathyXin Yee TanNo ratings yet
- 0054KCJ - KCJ 41 695Document8 pages0054KCJ - KCJ 41 695Valentina Giraldo JaramilloNo ratings yet
- Update Guideline For Intravenous Contrast Used of CT and MRIDocument12 pagesUpdate Guideline For Intravenous Contrast Used of CT and MRITenta Hartian HendyatamaNo ratings yet
- The Challenge of Kidney Damage During Interventional Cardiology ProceduresDocument6 pagesThe Challenge of Kidney Damage During Interventional Cardiology ProceduresIJAR JOURNALNo ratings yet
- Journal of Nephropathology: Contrast-Induced Nephropathy A Literature ReviewDocument6 pagesJournal of Nephropathology: Contrast-Induced Nephropathy A Literature ReviewayupurnamasariiNo ratings yet
- Ojsadmin, 176Document4 pagesOjsadmin, 176Signor 2019No ratings yet
- Preoperative Serum Bicarbonate Levels Predict Acute Kidney Injury After Cardiac SurgeryDocument11 pagesPreoperative Serum Bicarbonate Levels Predict Acute Kidney Injury After Cardiac SurgeryRoni ArmandaNo ratings yet
- Acute Renal Failure in The ICU PulmCritDocument27 pagesAcute Renal Failure in The ICU PulmCritchadchimaNo ratings yet
- Perioperative Acute Kidney InjuryDocument11 pagesPerioperative Acute Kidney InjuryNabil BachmidNo ratings yet
- Perioperative Acute Kidney Injury: DR Mukul Kapoor Director Anesthesia, Max Smart Super Specialty Hospital, Saket, DelhiDocument46 pagesPerioperative Acute Kidney Injury: DR Mukul Kapoor Director Anesthesia, Max Smart Super Specialty Hospital, Saket, DelhiChiragNo ratings yet
- Prevention and Management AKIDocument24 pagesPrevention and Management AKIZulhendraNo ratings yet
- Size-Selective Genetic Nanocage-Based Activatable Crispr-Cas12A For Hypersensitive Along With Accurate Detection of Older MicrornaDocument1 pageSize-Selective Genetic Nanocage-Based Activatable Crispr-Cas12A For Hypersensitive Along With Accurate Detection of Older Micrornaflareyellow24No ratings yet
- Preventing Contrast-Induced Renal Failure: A Guide: CoronaryDocument7 pagesPreventing Contrast-Induced Renal Failure: A Guide: CoronarySisca Dwi AgustinaNo ratings yet
- Ijda 5 024 PDFDocument5 pagesIjda 5 024 PDFKumarsai DurusojuNo ratings yet
- Chapter 31 - Anesthesia For Patients With Kidney DiseaseDocument21 pagesChapter 31 - Anesthesia For Patients With Kidney DiseasefewNo ratings yet
- EGDTDocument33 pagesEGDTaLineLanNo ratings yet
- Lesion Renal Aguda 2017Document20 pagesLesion Renal Aguda 2017Jorge Luis German BecerraNo ratings yet
- Serum Uric Acid To Albumin Ratio Can Predict Contrast-Induced Nephropathy in ST-Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary inDocument9 pagesSerum Uric Acid To Albumin Ratio Can Predict Contrast-Induced Nephropathy in ST-Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary intinatobingNo ratings yet
- Surviving Sepsis: Early Goal Directed TherapyDocument34 pagesSurviving Sepsis: Early Goal Directed Therapyyehezkiel_yesiNo ratings yet
- Modern Management of Acute PancreatitisDocument8 pagesModern Management of Acute Pancreatitisheyiy20669No ratings yet
- 8 Meq/L PH 7.2) May Require Iv Therapy (See Chap. 51) .: Evaluation of Therapeutic OutcomesDocument2 pages8 Meq/L PH 7.2) May Require Iv Therapy (See Chap. 51) .: Evaluation of Therapeutic OutcomesDebbyNovriozaNo ratings yet
- Brar 2014Document10 pagesBrar 2014Ismael Rivera DiazNo ratings yet
- Tumor Lysis SyndromeDocument5 pagesTumor Lysis SyndromeSusan RamosNo ratings yet
- The Janus Faces of Bicarbonate Therapy in The ICU: What'S New in Intensive CareDocument3 pagesThe Janus Faces of Bicarbonate Therapy in The ICU: What'S New in Intensive CarenidaNo ratings yet
- Contrast NephRopathy GuidelinesDocument3 pagesContrast NephRopathy GuidelinesStacey WoodsNo ratings yet
- Clinical Pearls in NephrologyDocument5 pagesClinical Pearls in NephrologyEdmilson R. LimaNo ratings yet
- Kontras StatinDocument10 pagesKontras Statinale_rhdNo ratings yet
- Management of Diabetes Mellitus in Patients With Chronic Kidney DiseaseDocument9 pagesManagement of Diabetes Mellitus in Patients With Chronic Kidney DiseasezakyNo ratings yet
- CKD DietDocument4 pagesCKD Dietpj rakNo ratings yet
- Select Drug-Drug Interactions With Colchicine and Cardiovascular Medications A ReviewDocument23 pagesSelect Drug-Drug Interactions With Colchicine and Cardiovascular Medications A ReviewsunhaolanNo ratings yet
- Perioperative Acute Kidney Injury: Charuhas V. ThakarDocument9 pagesPerioperative Acute Kidney Injury: Charuhas V. ThakarjessicaNo ratings yet
- Novel Aspects of Pharmacological Therapies For Acute Renal FailureDocument16 pagesNovel Aspects of Pharmacological Therapies For Acute Renal FailureproluvieslacusNo ratings yet
- Association Between Blood Transfusion and Serum Creatinine As A Major Risk Factor in Patients Undergoing Cardiac Surgeries: An Observational StudyDocument5 pagesAssociation Between Blood Transfusion and Serum Creatinine As A Major Risk Factor in Patients Undergoing Cardiac Surgeries: An Observational StudyIseth ISethNo ratings yet
- Bahan CKD Jurnal ProposalDocument6 pagesBahan CKD Jurnal ProposalArjunaPamungkasNo ratings yet
- Sepsis and Septic Shock Guidelines: DR Mahesh KumarDocument45 pagesSepsis and Septic Shock Guidelines: DR Mahesh KumarMahesh RajwalNo ratings yet
- Kidney Biomarkers: Clinical Aspects and Laboratory DeterminationFrom EverandKidney Biomarkers: Clinical Aspects and Laboratory DeterminationSeema S. AhujaNo ratings yet
- Out 21 PDFDocument10 pagesOut 21 PDFBlank SpaceNo ratings yet
- Treatment of Hepatitis C in Patients With Renal Impairment: Background and DefinitionsDocument23 pagesTreatment of Hepatitis C in Patients With Renal Impairment: Background and DefinitionsAnonymous ce3S6XFdwUNo ratings yet
- Delaying or Halting Progression of Chronic Kidney DiseaseDocument9 pagesDelaying or Halting Progression of Chronic Kidney Diseasehannya manNo ratings yet
- Cleveland Clinic Journal of Medicine 2013 BARON 354 9Document6 pagesCleveland Clinic Journal of Medicine 2013 BARON 354 9Stephanie PlascenciaNo ratings yet
- Management of Severe Sepsis: Learning ObjectivesDocument5 pagesManagement of Severe Sepsis: Learning ObjectivesVictoriano Valiente100% (1)
- Continuous Renal Replacement Therapy Among Patients With COVID-19 and Acute Kidney InjuryDocument8 pagesContinuous Renal Replacement Therapy Among Patients With COVID-19 and Acute Kidney InjuryPIR BanjarmasinNo ratings yet
- Continuous Intravenous Vitamin C in The Cancer Treatment - Reevaluation of A Phase I Clinical StudyDocument25 pagesContinuous Intravenous Vitamin C in The Cancer Treatment - Reevaluation of A Phase I Clinical StudyFilipos ConstantinNo ratings yet
- Acute Kidney Injury 2Document15 pagesAcute Kidney Injury 2Manish VijayNo ratings yet
- Pi Is 1089326121000039Document20 pagesPi Is 1089326121000039Muzaffar MehdiNo ratings yet
- Pearls Nov Dec 2010Document2 pagesPearls Nov Dec 2010MohammadAwitNo ratings yet
- Pearls Nov Dec 2010Document2 pagesPearls Nov Dec 2010MohammadAwitNo ratings yet
- Role of Ultrasonography in Knee Osteoarthritis: EviewDocument6 pagesRole of Ultrasonography in Knee Osteoarthritis: EviewSandroLao0% (1)
- Complication of Spina AnesthesiaDocument8 pagesComplication of Spina AnesthesiaSandroLaoNo ratings yet
- Breast Feading in Woman That Take Antepileptic DrugsDocument8 pagesBreast Feading in Woman That Take Antepileptic DrugsSandroLaoNo ratings yet
- Statin Treatment Reduce SeizureDocument8 pagesStatin Treatment Reduce SeizureSandroLaoNo ratings yet
- Dysfunction of The Sacroiliac Joint and Its Treatment : Richard L. Dontigny, BS, PTTDocument14 pagesDysfunction of The Sacroiliac Joint and Its Treatment : Richard L. Dontigny, BS, PTTSandroLaoNo ratings yet
- Wednesday Paris (Bercy Seine) : Connection 801Document2 pagesWednesday Paris (Bercy Seine) : Connection 801SandroLaoNo ratings yet
- Caffeine in The Management of Patients With Headache: Reviewarticle Open AccessDocument11 pagesCaffeine in The Management of Patients With Headache: Reviewarticle Open AccessSandroLaoNo ratings yet
- Tanda Vital NormalDocument1 pageTanda Vital NormalSandroLaoNo ratings yet
- Knee OADocument4 pagesKnee OASandroLaoNo ratings yet
- Tanda Vital NormalDocument1 pageTanda Vital NormalSandroLaoNo ratings yet
- Investigation of Leukimia in Childhood and AdultDocument8 pagesInvestigation of Leukimia in Childhood and AdultSandroLaoNo ratings yet
- Playing Video Games Liked To AsthmaDocument2 pagesPlaying Video Games Liked To AsthmaSandroLaoNo ratings yet
- 148E CPG August2004Document7 pages148E CPG August2004Ekhlas Al-AbsyNo ratings yet
- Kuis FMS 2Document8 pagesKuis FMS 2SandroLaoNo ratings yet
- Weight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Document1 pageWeight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Malisa LukmanNo ratings yet
- EAU Guidelines Renal Cell Carcinoma 2016Document62 pagesEAU Guidelines Renal Cell Carcinoma 2016SandroLaoNo ratings yet
- 2012 Diabetic Foot Infections GuidelineDocument42 pages2012 Diabetic Foot Infections GuidelineFadilLoveMamaNo ratings yet
- 11 Retinopa PDFDocument4 pages11 Retinopa PDFNiko Nofian NugrohoNo ratings yet
- RdsDocument11 pagesRdsSandroLaoNo ratings yet
- Toxic Hepatitis: What Does The Liver Do?Document2 pagesToxic Hepatitis: What Does The Liver Do?SandroLaoNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaSandroLaoNo ratings yet
- Gangguan Mood Episode Depresi SedangDocument6 pagesGangguan Mood Episode Depresi SedangSandroLaoNo ratings yet
- PA NeuroDocument2 pagesPA NeuroSandroLaoNo ratings yet
- Mikro BioDocument3 pagesMikro BioSandroLaoNo ratings yet
- Jumlah SKS 23 20100046: No Kode MK Deskripsi Class Number/Section SKS UTS UASDocument1 pageJumlah SKS 23 20100046: No Kode MK Deskripsi Class Number/Section SKS UTS UASSandroLaoNo ratings yet
- Latihan NeuroDocument9 pagesLatihan NeuroSandroLaoNo ratings yet
- GRCHRT Boys 24HdCirc-L4W Rev90910Document1 pageGRCHRT Boys 24HdCirc-L4W Rev90910jjys29No ratings yet
- Pepperberg Notes On The Learning ApproachDocument3 pagesPepperberg Notes On The Learning ApproachCristina GherardiNo ratings yet
- ITCNASIA23 - Visitor GuideDocument24 pagesITCNASIA23 - Visitor Guideibrahim shabbirNo ratings yet
- Mahindra First Choice Wheels LTD: 4-Wheeler Inspection ReportDocument5 pagesMahindra First Choice Wheels LTD: 4-Wheeler Inspection ReportRavi LoveNo ratings yet
- Analysis of MMDR Amendment ActDocument5 pagesAnalysis of MMDR Amendment ActArunabh BhattacharyaNo ratings yet
- Jar Doc 06 Jjarus Sora Executive SummaryDocument3 pagesJar Doc 06 Jjarus Sora Executive Summaryprasenjitdey786No ratings yet
- Iit-Jam Mathematics Test: Modern Algebra Time: 60 Minutes Date: 08-10-2017 M.M.: 45Document6 pagesIit-Jam Mathematics Test: Modern Algebra Time: 60 Minutes Date: 08-10-2017 M.M.: 45Lappy TopNo ratings yet
- Service Letter Service Letter Service Letter Service Letter: Commercial Aviation ServicesDocument3 pagesService Letter Service Letter Service Letter Service Letter: Commercial Aviation ServicesSamarNo ratings yet
- Molde Soldadura TADocument1 pageMolde Soldadura TAMarcos Ivan Ramirez AvenaNo ratings yet
- DILG Opinion-Sanggunian Employees Disbursements, Sign Checks & Travel OrderDocument2 pagesDILG Opinion-Sanggunian Employees Disbursements, Sign Checks & Travel OrderCrizalde de DiosNo ratings yet
- Beng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtDocument9 pagesBeng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtMarcelo BaptistaNo ratings yet
- Coefficient of Restitution - Center of MassDocument3 pagesCoefficient of Restitution - Center of MassMannyCesNo ratings yet
- Eaai S 23 02045 PDFDocument28 pagesEaai S 23 02045 PDFAnjali JainNo ratings yet
- Master Data FileDocument58 pagesMaster Data Fileinfo.glcom5161No ratings yet
- Coc 1 ExamDocument7 pagesCoc 1 ExamJelo BioNo ratings yet
- International Business ManagementDocument3 pagesInternational Business Managementkalaiselvi_velusamyNo ratings yet
- Pds Hempel's Maestro Water Borne Primer 28830 En-GbDocument2 pagesPds Hempel's Maestro Water Borne Primer 28830 En-GbKalaiyazhagan ElangeeranNo ratings yet
- SAP HCM Case StudyDocument17 pagesSAP HCM Case StudyRafidaFatimatuzzahraNo ratings yet
- Offshore Training Matriz Matriz de Treinamentos OffshoreDocument2 pagesOffshore Training Matriz Matriz de Treinamentos OffshorecamiladiasmanoelNo ratings yet
- Evaporative CoolingDocument68 pagesEvaporative Coolingshivas34regal100% (1)
- HYDRAULIC WINCH-MS1059 - Operation & Maintenance Manual Rev ADocument33 pagesHYDRAULIC WINCH-MS1059 - Operation & Maintenance Manual Rev Azulu80No ratings yet
- Eddie Struble - Spring Valley Police Report Page 1Document1 pageEddie Struble - Spring Valley Police Report Page 1watchkeepNo ratings yet
- Schermer 1984Document25 pagesSchermer 1984Pedro VeraNo ratings yet
- Mini Project A-9-1Document12 pagesMini Project A-9-1santhoshrao19No ratings yet
- 4BT3 9-G2 PDFDocument5 pages4BT3 9-G2 PDFNv Thái100% (1)
- Technical DescriptionDocument2 pagesTechnical Descriptioncocis_alexandru04995No ratings yet
- p7000 Series PDFDocument592 pagesp7000 Series PDFtony445No ratings yet
- Ce Licensure Examination Problems Rectilinear Translation 6Document2 pagesCe Licensure Examination Problems Rectilinear Translation 6Ginto AquinoNo ratings yet
- Die Openbare BeskermerDocument3 pagesDie Openbare BeskermerJaco BesterNo ratings yet
- Adding and Subtracting FractionsDocument4 pagesAdding and Subtracting Fractionsapi-508898016No ratings yet
- Reviewer in EntrepreneurshipDocument6 pagesReviewer in EntrepreneurshipRachelle Anne SaldeNo ratings yet