You might also like
- Benefit Manual - Aecom IndiaDocument32 pagesBenefit Manual - Aecom IndiaAnil PuvadaNo ratings yet
- Removal of Sharp Object Patient SaftyDocument6 pagesRemoval of Sharp Object Patient SaftyAlibaba AlihaihaiNo ratings yet
- Ipsg 6 Patient SafetyDocument12 pagesIpsg 6 Patient SafetyJamilaturRasyidahEfendiNo ratings yet
- Sample Research ProposalDocument43 pagesSample Research ProposalLuis LazaroNo ratings yet
- IBISWorld Industry Report Physical Therapists in The US 2019Document39 pagesIBISWorld Industry Report Physical Therapists in The US 2019uwybkpeyawxubbhxjyNo ratings yet
- Quality Improvement Paper FinalDocument11 pagesQuality Improvement Paper Finalapi-291740538No ratings yet
- OPPE & FPPE Joint Commission Standards - HuntDocument11 pagesOPPE & FPPE Joint Commission Standards - HuntUwie AnaNo ratings yet
- HealthCare Industry AnalysisDocument20 pagesHealthCare Industry Analysisbinzidd00767% (3)
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Quality Improvement in Reducing Falls in A Medical-Surgical-TelemDocument41 pagesQuality Improvement in Reducing Falls in A Medical-Surgical-Telemtahani tttNo ratings yet
- PICOT Question GRADEDDocument6 pagesPICOT Question GRADEDkeybateNo ratings yet
- MICE (Syllabus)Document7 pagesMICE (Syllabus)felamendoNo ratings yet
- Test Bank For Fundamentals of Management 11th Edition by RobbinsDocument24 pagesTest Bank For Fundamentals of Management 11th Edition by RobbinsKathyChristiancxpy98% (45)
- Effectiveness of A Fall Prevention ChecklistDocument36 pagesEffectiveness of A Fall Prevention ChecklistAndreaNo ratings yet
- Manual of Standards On Quality Management System in The Clinical Laboratory Ver 2008Document76 pagesManual of Standards On Quality Management System in The Clinical Laboratory Ver 2008vincent frederick botin100% (1)
- Establishing a Culture of Patient Safety: Improving Communication, Building Relationships, and Using Quality ToolsFrom EverandEstablishing a Culture of Patient Safety: Improving Communication, Building Relationships, and Using Quality ToolsNo ratings yet
- To Study The Perception and Attitude of People Towards Public and Private Healthcare Facilities in ChandigarhDocument62 pagesTo Study The Perception and Attitude of People Towards Public and Private Healthcare Facilities in ChandigarhSneha RajNo ratings yet
- Evidence Based RUADocument12 pagesEvidence Based RUAAsma AliNo ratings yet
- Literature Review GRADEDDocument7 pagesLiterature Review GRADEDkeybateNo ratings yet
- Quantitative Article Critique and SummaryDocument8 pagesQuantitative Article Critique and SummaryEmmanuelNo ratings yet
- Nurse Practitioner Research PaperDocument8 pagesNurse Practitioner Research Paperqzafzzhkf100% (1)
- Fall Prevention Research PaperDocument8 pagesFall Prevention Research Paperorlfgcvkg100% (1)
- Falls Preventative MeasuresDocument20 pagesFalls Preventative MeasuresjosephineNo ratings yet
- Declaration of Vienna ArticleDocument6 pagesDeclaration of Vienna ArticleDwi SurantoNo ratings yet
- 1 Running Head: Therapeutic Nursing InterventionsDocument8 pages1 Running Head: Therapeutic Nursing Interventionsapi-337126539No ratings yet
- MID 2 SJ - bdj.2012.1008Document5 pagesMID 2 SJ - bdj.2012.1008Green SleevesNo ratings yet
- Fall Prevention ThesisDocument5 pagesFall Prevention ThesisFelicia Clark100% (2)
- Running Head: Professional Development Assignment 1Document12 pagesRunning Head: Professional Development Assignment 1api-396212664No ratings yet
- 10 1016@j Ijnurstu 2019 103449Document24 pages10 1016@j Ijnurstu 2019 103449mahrani_adrinNo ratings yet
- Running Head: PATIENT FALLS 1Document9 pagesRunning Head: PATIENT FALLS 1api-284786443No ratings yet
- Leadership Analysis PaperDocument8 pagesLeadership Analysis Paperapi-238680155No ratings yet
- Nur 467 Portfolio Scholarly Work 1 02 17 14Document8 pagesNur 467 Portfolio Scholarly Work 1 02 17 14api-247935508No ratings yet
- Black Elk Medical CenterDocument4 pagesBlack Elk Medical Centergeelickvb0% (1)
- Activity 3Document2 pagesActivity 39cwkwgccdjNo ratings yet
- Practices: in Patient CareDocument5 pagesPractices: in Patient Careahmad nuril hidayatNo ratings yet
- QI ProjectDocument14 pagesQI ProjectAbigailNo ratings yet
- Research Paper On Health Care CrisisDocument8 pagesResearch Paper On Health Care Crisiscaq5s6ex100% (1)
- Epidemiology Thesis PDFDocument6 pagesEpidemiology Thesis PDFafknojbcf100% (2)
- Community Health Nursing Research PapersDocument8 pagesCommunity Health Nursing Research Papersegabnlrhf100% (1)
- Daily Goals Tools Enhancing Outcomes in A Surgical Intensive Care Unit by ImplementingDocument14 pagesDaily Goals Tools Enhancing Outcomes in A Surgical Intensive Care Unit by ImplementingAnugerah Eka PurwantiNo ratings yet
- Chinese Nursing Research: Yuan-Yuan Gu, Koen Balcaen, Yicheng Ni, Jan Ampe, Jan Gof FinDocument4 pagesChinese Nursing Research: Yuan-Yuan Gu, Koen Balcaen, Yicheng Ni, Jan Ampe, Jan Gof FinRara RianitaNo ratings yet
- Implementing Interventions To Reduce Falls RevisedDocument12 pagesImplementing Interventions To Reduce Falls RevisedScholah NgeiNo ratings yet
- WFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionDocument13 pagesWFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionJuan Carlos Mora TorresNo ratings yet
- Quality Improvement ProjectDocument6 pagesQuality Improvement Projectapi-317112346No ratings yet
- Hand Hygiene Thesis IntroductionDocument7 pagesHand Hygiene Thesis Introductionbk34np00100% (2)
- Thesis Hospital AdministrationDocument8 pagesThesis Hospital Administrationjanaclarkbillings100% (1)
- Designing and Implementing A Zero Harm Falls.2Document7 pagesDesigning and Implementing A Zero Harm Falls.2hikmaanas02No ratings yet
- JOURNALsDocument3 pagesJOURNALsJhexy Rhay BayagenNo ratings yet
- Thesis Statement On HospitalsDocument5 pagesThesis Statement On Hospitalsbkrj0a1k100% (1)
- NR520 Module 3 Assessment Project Area of Interest FormDocument5 pagesNR520 Module 3 Assessment Project Area of Interest Form96rubadiri96No ratings yet
- Healthcare Management Thesis PDFDocument5 pagesHealthcare Management Thesis PDFmelissabuckleyomaha100% (2)
- Implementing A Fall Prevention Program - A Quality Improvement ProDocument68 pagesImplementing A Fall Prevention Program - A Quality Improvement Protahani tttNo ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Research Paper Nursing ShortageDocument5 pagesResearch Paper Nursing Shortagezijkchbkf100% (1)
- Epidemiology PHD Thesis PDFDocument6 pagesEpidemiology PHD Thesis PDFxnehytwff100% (1)
- Thesis Statement About Health Care ManagementDocument9 pagesThesis Statement About Health Care Managementubkciwwff100% (2)
- Health Care Crisis Thesis StatementDocument4 pagesHealth Care Crisis Thesis Statementsdeaqoikd100% (1)
- Interventions To Decrease Catheter-Related Bloodstream Infections in The ICU: The Keystone Intensive Care Unit ProjectDocument5 pagesInterventions To Decrease Catheter-Related Bloodstream Infections in The ICU: The Keystone Intensive Care Unit ProjectanggitaNo ratings yet
- Groah 2014 Table TalkDocument12 pagesGroah 2014 Table TalkChandra JohannesNo ratings yet
- Master of Public Health Thesis ExamplesDocument5 pagesMaster of Public Health Thesis Examplesp0kasov1syd2100% (2)
- Eblr Formal Paper KropkoDocument10 pagesEblr Formal Paper Kropkoapi-586815209No ratings yet
- Health Care Crisis Research PaperDocument5 pagesHealth Care Crisis Research Paperjrqkuvwgf100% (1)
- Apss VapDocument14 pagesApss VapRoxanA BocaNo ratings yet
- Final Safety Group Paper490WDocument17 pagesFinal Safety Group Paper490WLYZETTE TERMANNo ratings yet
- Understanding The Nursing ProcessDocument7 pagesUnderstanding The Nursing ProcessAbdul HakeemNo ratings yet
- Synthesis Project Group Final-FallsDocument18 pagesSynthesis Project Group Final-Fallsapi-290381420No ratings yet
- Managemen MutuDocument8 pagesManagemen MutuMerty TaolinNo ratings yet
- Literature Review On Patient FallsDocument7 pagesLiterature Review On Patient Fallsaflsiosbe100% (1)
- Information On Clinical Device Protocol TemplateDocument25 pagesInformation On Clinical Device Protocol TemplatefelamendoNo ratings yet
- NET Topic 20080226 Disclosure of Adverse EventsDocument23 pagesNET Topic 20080226 Disclosure of Adverse EventsfelamendoNo ratings yet
- CPE19 Ethics Discussion Questions Oct 2007Document16 pagesCPE19 Ethics Discussion Questions Oct 2007felamendoNo ratings yet
- Case Scenarios On EthicsDocument2 pagesCase Scenarios On EthicsfelamendoNo ratings yet
- Annual Progress Report Form ResearchDocument4 pagesAnnual Progress Report Form ResearchfelamendoNo ratings yet
- APP022 Reportable Events Form - FORMFILLDocument2 pagesAPP022 Reportable Events Form - FORMFILLfelamendoNo ratings yet
- PGdissertationguidelinesDocument27 pagesPGdissertationguidelinesfelamendoNo ratings yet
- NET Topic 20030429 Disclosing Adverse EventsDocument19 pagesNET Topic 20030429 Disclosing Adverse EventsfelamendoNo ratings yet
- A) College of Arts Research Ethics Checklist: Ethics Committee For Non-Clinical Research Involving Human SubjectsDocument4 pagesA) College of Arts Research Ethics Checklist: Ethics Committee For Non-Clinical Research Involving Human SubjectsfelamendoNo ratings yet
- Don Moore, PHD Candidate, Mcmaster UniversityDocument12 pagesDon Moore, PHD Candidate, Mcmaster UniversityfelamendoNo ratings yet
- Information Memorandum P02-1 State of New Jersey Department of Human ServicesDocument5 pagesInformation Memorandum P02-1 State of New Jersey Department of Human ServicesfelamendoNo ratings yet
- Ethical ReasoningDocument3 pagesEthical ReasoningfelamendoNo ratings yet
- Ethics Gifts BetweenDocument2 pagesEthics Gifts BetweenfelamendoNo ratings yet
- GNAC Sportsmanship FormDocument2 pagesGNAC Sportsmanship FormfelamendoNo ratings yet
- National Association of School Psychologists: Formal Ethics Complaint FormDocument2 pagesNational Association of School Psychologists: Formal Ethics Complaint Formfelamendo0% (1)
- Ethics and Media Globalization QuizDocument3 pagesEthics and Media Globalization QuizfelamendoNo ratings yet
- Ethics and Media Globalization QuizDocument3 pagesEthics and Media Globalization QuizfelamendoNo ratings yet
- Be It Enacted by The General Assembly of The Commonwealth of KentuckyDocument5 pagesBe It Enacted by The General Assembly of The Commonwealth of KentuckyfelamendoNo ratings yet
- Tradoc 122261Document3 pagesTradoc 122261felamendoNo ratings yet
- 17OMD185Document6 pages17OMD185felamendoNo ratings yet
- National Association of School Psychologists: Formal Ethics Complaint FormDocument2 pagesNational Association of School Psychologists: Formal Ethics Complaint Formfelamendo0% (1)
- Statement On Scholarly Capacity Rule and UECDocument1 pageStatement On Scholarly Capacity Rule and UECfelamendoNo ratings yet
- EE Policy 2006Document3 pagesEE Policy 2006felamendoNo ratings yet
- Stress ManagementDocument10 pagesStress ManagementRishabh MehtaNo ratings yet
- Abuse Prevention / Services: Worcester CountyDocument3 pagesAbuse Prevention / Services: Worcester CountyfelamendoNo ratings yet
- Response Form - Mental Health of Men and Boys InquiryDocument4 pagesResponse Form - Mental Health of Men and Boys InquiryfelamendoNo ratings yet
- Adult Education: Was There An "Embodied Argument"? If So, What Happened To It?Document7 pagesAdult Education: Was There An "Embodied Argument"? If So, What Happened To It?felamendoNo ratings yet
- Certified For Publication: Filed 1/8/19Document15 pagesCertified For Publication: Filed 1/8/19felamendoNo ratings yet
- Certified For Publication: Filed 1/8/19Document15 pagesCertified For Publication: Filed 1/8/19felamendoNo ratings yet
- Problem Identification and Policy Development TranscriptDocument3 pagesProblem Identification and Policy Development Transcriptreadandwrite512No ratings yet
- SC Judgment For Acid Attack VictimsDocument25 pagesSC Judgment For Acid Attack VictimsLatest Laws Team100% (1)
- AnnualReport2017 2018 PDFDocument236 pagesAnnualReport2017 2018 PDFsuryateja kudapaNo ratings yet
- Cally Lanning 2013Document2 pagesCally Lanning 2013api-242477507No ratings yet
- Sbi General'S Arogya Plus Policy: Assure Your Health For A Fixed PremiumDocument9 pagesSbi General'S Arogya Plus Policy: Assure Your Health For A Fixed Premiumdinesh banaNo ratings yet
- Director ResponsibilitiesDocument4 pagesDirector ResponsibilitiesNeerja ChauhanNo ratings yet
- PIVOT Strategic Plan 2018-2022Document35 pagesPIVOT Strategic Plan 2018-2022PivotNo ratings yet
- Asking Question, Introduction, Language and FunctionDocument42 pagesAsking Question, Introduction, Language and FunctionAbdul adhimNo ratings yet
- Basic PlanDocument3 pagesBasic Planrahul sNo ratings yet
- Sehteq CARE and CARE PLUS RN3 Network - May 2021Document87 pagesSehteq CARE and CARE PLUS RN3 Network - May 2021cmthebossNo ratings yet
- DOH AO No - 2020 0021Document15 pagesDOH AO No - 2020 0021MariaChristinaVaronaTemplanzaNo ratings yet
- Open For Business Magazine - Oct/No v14 IssueDocument13 pagesOpen For Business Magazine - Oct/No v14 IssueEugene Area Chamber of Commerce CommunicationsNo ratings yet
- Effective Use of Behavioral Care PlansDocument27 pagesEffective Use of Behavioral Care PlansZahraa Ali dawoodNo ratings yet
- Lifeline 2.0 Policy WordingDocument60 pagesLifeline 2.0 Policy WordingAsish Kumar JenaNo ratings yet
- Unit 5 Security Assignment 1 of 1Document6 pagesUnit 5 Security Assignment 1 of 1Swam Pyae Maung Maung100% (1)
- POS CodesDocument5 pagesPOS CodesKarna Palanivelu100% (2)
- Gondar, EthiopiaDocument27 pagesGondar, Ethiopianegussie birieNo ratings yet
- Introduction:-: Ambulatory Healthcare Organizations IntroducedDocument7 pagesIntroduction:-: Ambulatory Healthcare Organizations Introducedanimesh pandaNo ratings yet
- Model Statues 2016Document309 pagesModel Statues 2016Adnan KhanNo ratings yet
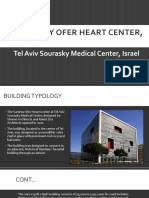
- The Sammy Ofer Heart CenterDocument17 pagesThe Sammy Ofer Heart CenterHIRA SHABBIR100% (1)
- Company ProfileDocument5 pagesCompany Profileganguly_ajayNo ratings yet
- KZN Health Act 1 20091Document51 pagesKZN Health Act 1 20091ZizileMaNkosiButheleziNo ratings yet
- YawaDocument6 pagesYawaChuche Marie TumarongNo ratings yet