You might also like
- Surgical Management of Childhood Glaucoma: Clinical Considerations and TechniquesFrom EverandSurgical Management of Childhood Glaucoma: Clinical Considerations and TechniquesAlana L. GrajewskiNo ratings yet
- Vitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyDocument8 pagesVitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyVlady BordaNo ratings yet
- Posterior Surgical Revision of Failed TrabDocument7 pagesPosterior Surgical Revision of Failed TrabASHOK KUMAR SINGHNo ratings yet
- Pars Plana VitrekDocument8 pagesPars Plana VitrekAnggisari Danastri DharmaNo ratings yet
- OJOph 2016062717483031Document8 pagesOJOph 2016062717483031dechastraNo ratings yet
- 69 EdDocument10 pages69 EdAnna ListianaNo ratings yet
- JurdingDocument8 pagesJurdingTanani 102014007No ratings yet
- Comparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesDocument7 pagesComparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesVlady BordaNo ratings yet
- 1 s2.0 S1319453417301418 MainDocument4 pages1 s2.0 S1319453417301418 MainEzra MargarethNo ratings yet
- AVB Christakis2016Document10 pagesAVB Christakis2016Ahmed NahrawyNo ratings yet
- Safety and Efficacy of Ahmed Glaucoma Valve Implantation in Refractory Glaucomas in Northern Indian EyesDocument7 pagesSafety and Efficacy of Ahmed Glaucoma Valve Implantation in Refractory Glaucomas in Northern Indian EyesVlady BordaNo ratings yet
- Surgery For Glaucoma in Patients With Facial Port Wine MarkDocument6 pagesSurgery For Glaucoma in Patients With Facial Port Wine MarkPutri kartiniNo ratings yet
- Silicone Ahmed Glaucoma Valve With and Without Intravitreal Triamcinolone Acetonide For Neovascular Glaucoma: Randomized Clinical TrialDocument7 pagesSilicone Ahmed Glaucoma Valve With and Without Intravitreal Triamcinolone Acetonide For Neovascular Glaucoma: Randomized Clinical TrialVlady BordaNo ratings yet
- Anterior Vitrectomy and Partial Capsulectomy Anterior Approach To Treat Chronic Postoperative EndophthalmitisDocument3 pagesAnterior Vitrectomy and Partial Capsulectomy Anterior Approach To Treat Chronic Postoperative EndophthalmitisSurendar KesavanNo ratings yet
- Dr. Ankur Kumar, Dr. Kishor KumarDocument4 pagesDr. Ankur Kumar, Dr. Kishor KumarValentina Gracia ReyNo ratings yet
- 2005 Minimally Invasive Glaucoma SurgeryDocument9 pages2005 Minimally Invasive Glaucoma SurgeryJoseNo ratings yet
- Anaesthesia For Vitreo-Retinal SurgeryDocument6 pagesAnaesthesia For Vitreo-Retinal SurgeryRuwan KuruppuNo ratings yet
- Kag Rully (B.IG)Document7 pagesKag Rully (B.IG)Rully Dwi SaputraNo ratings yet
- 3 Piece IOL SCL FixDocument6 pages3 Piece IOL SCL FixTvrtka BenašićNo ratings yet
- Efficacy of Autologous Blood Clot in Primary Pterygium Surgery Compared With Suture Technique in A Tertiary Hospital of BangladeshDocument7 pagesEfficacy of Autologous Blood Clot in Primary Pterygium Surgery Compared With Suture Technique in A Tertiary Hospital of BangladeshBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Trabeculectomy With Large Area Mitomycin-C Application As A First-Line Treatment in Advanced Glaucoma: Retrospective ReviewDocument6 pagesTrabeculectomy With Large Area Mitomycin-C Application As A First-Line Treatment in Advanced Glaucoma: Retrospective ReviewMaria Angelina BunawanNo ratings yet
- Comparison of Postoperative Refractive Outcome in Eyes UndergoingDocument9 pagesComparison of Postoperative Refractive Outcome in Eyes UndergoingAndi Ayu LestariNo ratings yet
- Clinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsDocument6 pagesClinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsAldoNo ratings yet
- Staining Vitreous Triamcinolone Removes Dropped NucleiDocument4 pagesStaining Vitreous Triamcinolone Removes Dropped NucleiLina MarcelaNo ratings yet
- Vitrectomy For Endophthalmitis: 5-Year Study of Outcomes and ComplicationsDocument8 pagesVitrectomy For Endophthalmitis: 5-Year Study of Outcomes and ComplicationsqisthiNo ratings yet
- (19330693 - Journal of Neurosurgery) Neuroendoscopic Stent Placement For Cerebrospinal Fluid Pathway Obstructions in AdultsDocument9 pages(19330693 - Journal of Neurosurgery) Neuroendoscopic Stent Placement For Cerebrospinal Fluid Pathway Obstructions in AdultsVlad VPNo ratings yet
- Evaluation of SuturlessDocument7 pagesEvaluation of SuturlesskenapayaNo ratings yet
- ABSTRACT - BOOK - 10th IcgsDocument135 pagesABSTRACT - BOOK - 10th Icgsd_kourkoutasNo ratings yet
- Tugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Document8 pagesTugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Arina SetyaningrumNo ratings yet
- Surgical outcomes of retinal detachment in toxoplasmosis patientsDocument5 pagesSurgical outcomes of retinal detachment in toxoplasmosis patientsketrin capanemaNo ratings yet
- None 3Document11 pagesNone 3Yehiel FlaviusNo ratings yet
- Clinical StudyDocument6 pagesClinical StudyKarina Mega WNo ratings yet
- TVT Nihms335507 PDFDocument30 pagesTVT Nihms335507 PDFAhmed NahrawyNo ratings yet
- Retinal Detachment Repair Techniques 1-Year OutcomesDocument5 pagesRetinal Detachment Repair Techniques 1-Year OutcomesmardocoftNo ratings yet
- Facoemulsifucacion + Stent TrabecularDocument8 pagesFacoemulsifucacion + Stent TrabecularCarlos VerdiNo ratings yet
- Sulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryDocument6 pagesSulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryPrizilia SaimimaNo ratings yet
- Tube Exposure Repair: 10.5005/jp-Journals-10008-1121Document4 pagesTube Exposure Repair: 10.5005/jp-Journals-10008-1121alineochoaaNo ratings yet
- Suturas Liberables Ejo.5000718Document8 pagesSuturas Liberables Ejo.5000718Emile NumberNo ratings yet
- A Clinical Study On Visual Outcome and Complications of Penetrating KeratoplastyDocument12 pagesA Clinical Study On Visual Outcome and Complications of Penetrating KeratoplastyIOSRjournalNo ratings yet
- OpthalmologiDocument7 pagesOpthalmologirais123No ratings yet
- 16 Nigwekar Etal.Document4 pages16 Nigwekar Etal.editorijmrhsNo ratings yet
- The Effect of Trabeculectomy On Astigmatism .99150Document5 pagesThe Effect of Trabeculectomy On Astigmatism .99150Yulias YoweiNo ratings yet
- Glaukoma TripleDocument5 pagesGlaukoma TripleR.m. IrsanNo ratings yet
- Abstractbook2020 2Document50 pagesAbstractbook2020 2alpaslan alkanNo ratings yet
- Anaesthesia for Vitreo-Retinal SurgeryDocument6 pagesAnaesthesia for Vitreo-Retinal Surgeryluis castro martinezNo ratings yet
- Analysis of Intraoperative and Postoperative Complications in Pseudoexfoliation Eyes Undergoing Cataract SurgeryDocument4 pagesAnalysis of Intraoperative and Postoperative Complications in Pseudoexfoliation Eyes Undergoing Cataract SurgerymathyasthanamaNo ratings yet
- 3-Year Outcomes of Tube vs Trabeculectomy in Glaucoma StudyDocument13 pages3-Year Outcomes of Tube vs Trabeculectomy in Glaucoma StudyAhmed NahrawyNo ratings yet
- Macular and Visual Outcomes After Cataract Extraction For Highly Myopic FoveoschisisDocument5 pagesMacular and Visual Outcomes After Cataract Extraction For Highly Myopic Foveoschisisloshaana105No ratings yet
- Jurnal 1Document6 pagesJurnal 1Gusti Tanjung Putera RahayuNo ratings yet
- Keratopati BulosaDocument7 pagesKeratopati BulosaShafira LusianaNo ratings yet
- Eiger Moscovich2017Document6 pagesEiger Moscovich2017evilelagNo ratings yet
- Macular Hole Development After Vitrectomy For Floaters A Case ReportDocument5 pagesMacular Hole Development After Vitrectomy For Floaters A Case Reportmistic0No ratings yet
- KatarakDocument7 pagesKatarakayuNo ratings yet
- Ijo 10 12 1835Document9 pagesIjo 10 12 1835shofidhiaaaNo ratings yet
- A Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyDocument4 pagesA Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyRaul FonsecaNo ratings yet
- Emanuel 2017Document4 pagesEmanuel 2017Kimberly Ann SumbillaNo ratings yet
- Cost-Effectiveness of The Triple Procedure - PhacoDocument11 pagesCost-Effectiveness of The Triple Procedure - PhacoAndi Ayu LestariNo ratings yet
- Prabhakar 1Document4 pagesPrabhakar 1ChristaGisellaPirsouwNoyaNo ratings yet
- Clinical Study: Two-Year Accelerated Corneal Cross-Linking Outcome in Patients With Progressive KeratoconusDocument10 pagesClinical Study: Two-Year Accelerated Corneal Cross-Linking Outcome in Patients With Progressive KeratoconusPunam RazputriNo ratings yet
- Utility of Operative Glaucoma Tube Shunt Viscoelastic Bolus FlushDocument4 pagesUtility of Operative Glaucoma Tube Shunt Viscoelastic Bolus FlushNetflix DheaNo ratings yet
- Integrated Treatment During The Intravitreal Melphalan Era: Concurrent Intravitreal Melphalan and Systemic ChemoreductionDocument7 pagesIntegrated Treatment During The Intravitreal Melphalan Era: Concurrent Intravitreal Melphalan and Systemic ChemoreductionVlady BordaNo ratings yet
- Ce Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Document6 pagesCe Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Vlady BordaNo ratings yet
- Tacrolimus Optic NeuropathyDocument7 pagesTacrolimus Optic NeuropathyVlady BordaNo ratings yet
- Phacoemulsification Versus Extracapsular Cataract Extraction: Where Do We Stand?Document6 pagesPhacoemulsification Versus Extracapsular Cataract Extraction: Where Do We Stand?Vlady BordaNo ratings yet
- Retinoblastoma InglesDocument5 pagesRetinoblastoma InglesVlady BordaNo ratings yet
- Author Manuscript: Int Ophthalmol Clin. Author Manuscript Available in PMC 2012 July 1Document10 pagesAuthor Manuscript: Int Ophthalmol Clin. Author Manuscript Available in PMC 2012 July 1Vlady BordaNo ratings yet
- Advances of Optical Coherence Tomography in Myopia and Pathologic MyopiaDocument16 pagesAdvances of Optical Coherence Tomography in Myopia and Pathologic MyopiaVlady BordaNo ratings yet
- Evaluation of Effect of Topical Tacrolimus Treatment On Herpetic Stromal Keratitis in A Rat ModelDocument8 pagesEvaluation of Effect of Topical Tacrolimus Treatment On Herpetic Stromal Keratitis in A Rat ModelVlady BordaNo ratings yet
- Indian J Pediatr - Retinoblastoma: A ReviewDocument8 pagesIndian J Pediatr - Retinoblastoma: A ReviewVlady BordaNo ratings yet
- Update On Normal Tension Glaucoma: Review ArticleDocument10 pagesUpdate On Normal Tension Glaucoma: Review ArticleVlady BordaNo ratings yet
- Author Manuscript: Int Ophthalmol Clin. Author Manuscript Available in PMC 2012 July 1Document10 pagesAuthor Manuscript: Int Ophthalmol Clin. Author Manuscript Available in PMC 2012 July 1Vlady BordaNo ratings yet
- Fundamental of Clinical Ophthalmology .. StrabismDocument211 pagesFundamental of Clinical Ophthalmology .. StrabismMarcella PolittonNo ratings yet
- Optical Coherence Tomography Angiography of Pathological Myopia Sourced and Idiopathic Choroidal Neovascularization With Follow-UpDocument7 pagesOptical Coherence Tomography Angiography of Pathological Myopia Sourced and Idiopathic Choroidal Neovascularization With Follow-UpVlady BordaNo ratings yet
- Peripapillary Atrophy in Primary Angle-Closure Glaucoma: A ComparativeDocument8 pagesPeripapillary Atrophy in Primary Angle-Closure Glaucoma: A ComparativeVlady BordaNo ratings yet
- Silicone Ahmed Glaucoma Valve With and Without Intravitreal Triamcinolone Acetonide For Neovascular Glaucoma: Randomized Clinical TrialDocument7 pagesSilicone Ahmed Glaucoma Valve With and Without Intravitreal Triamcinolone Acetonide For Neovascular Glaucoma: Randomized Clinical TrialVlady BordaNo ratings yet
- Ahmed Glaucoma Valve and Single-Plate Molteno Implants in Treatment of Refractory Glaucoma: A Comparative StudyDocument10 pagesAhmed Glaucoma Valve and Single-Plate Molteno Implants in Treatment of Refractory Glaucoma: A Comparative StudyVlady BordaNo ratings yet
- Fundamental of Clinical Ophthalmology .. StrabismDocument211 pagesFundamental of Clinical Ophthalmology .. StrabismMarcella PolittonNo ratings yet
- Intravitreal Bevacizumab: Indications and Complications: Original ArticleDocument5 pagesIntravitreal Bevacizumab: Indications and Complications: Original ArticleVlady BordaNo ratings yet
- Sin Brown2Document353 pagesSin Brown2Vlady Borda100% (4)
- Comparison of Silicone and Polypropylene Ahmed Glaucoma Valves: Two-Year Follow-UpDocument8 pagesComparison of Silicone and Polypropylene Ahmed Glaucoma Valves: Two-Year Follow-UpVlady BordaNo ratings yet
- Safety and Efficacy of Ahmed Glaucoma Valve Implantation in Refractory Glaucomas in Northern Indian EyesDocument7 pagesSafety and Efficacy of Ahmed Glaucoma Valve Implantation in Refractory Glaucomas in Northern Indian EyesVlady BordaNo ratings yet
- RB ExpoDocument21 pagesRB ExpoVlady BordaNo ratings yet
- Ce Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Document6 pagesCe Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Vlady BordaNo ratings yet
- Ce Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Document5 pagesCe Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Vlady BordaNo ratings yet
- Ce Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Document5 pagesCe Ra1 F (Shu) Pf1 (Aj Shu) Pfa (Aj Shu) PB (Aj SL) PN (SL)Vlady BordaNo ratings yet
- Comparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesDocument7 pagesComparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesVlady BordaNo ratings yet
- Comparison of Polypropylene and Silicone Ahmed® Glaucoma Valves in The Treatment of Neovascular Glaucoma: A 2-Year Follow-UpDocument7 pagesComparison of Polypropylene and Silicone Ahmed® Glaucoma Valves in The Treatment of Neovascular Glaucoma: A 2-Year Follow-UpVlady BordaNo ratings yet
- Sin Brown2Document353 pagesSin Brown2Vlady Borda100% (4)
- Kodak Professional High-Speed Infrared Film: Technical Data / Black-And-White FilmDocument8 pagesKodak Professional High-Speed Infrared Film: Technical Data / Black-And-White FilmKhalid BahauddinNo ratings yet
- Colenbrander Measuring - Vis - Duane01 Voor MijDocument42 pagesColenbrander Measuring - Vis - Duane01 Voor MijJolien WalravenNo ratings yet
- Question 1-Canny Edge Detector (10 Points) : Fundamentals of Computer Vision - Midterm Exam Dr. B. NasihatkonDocument6 pagesQuestion 1-Canny Edge Detector (10 Points) : Fundamentals of Computer Vision - Midterm Exam Dr. B. NasihatkonHiroNo ratings yet
- Joe Burdett - : Astrophotography Cheat SheetDocument4 pagesJoe Burdett - : Astrophotography Cheat SheetM Mohsin ChowdhuryNo ratings yet
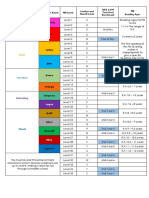
- PM reading levels and corresponding Fountas & Pinnell levelsDocument1 pagePM reading levels and corresponding Fountas & Pinnell levelsdot singh100% (1)
- Day-for-Night Filming TechniquesDocument7 pagesDay-for-Night Filming TechniquesArian Sánchez CovisaNo ratings yet
- The Far Point and Refractive Error ExplainedDocument44 pagesThe Far Point and Refractive Error ExplainedALberta YosheNo ratings yet
- Pengujian Hammer Test: SNI ASTM C805 2012 Modul Praktikum Ilmu BahanDocument54 pagesPengujian Hammer Test: SNI ASTM C805 2012 Modul Praktikum Ilmu BahanDiki SetiawanNo ratings yet
- Acrylic Painting Techniques: Methods On How To Paint With Acrylics For Acrylic Landscape Painting and InteriorsDocument25 pagesAcrylic Painting Techniques: Methods On How To Paint With Acrylics For Acrylic Landscape Painting and InteriorsRavin Taira Pal75% (4)
- Chapter-11 Human Eye and Colourful World MCQsDocument15 pagesChapter-11 Human Eye and Colourful World MCQsSiddhantNo ratings yet
- Optomap Af Diagnostic AtlasDocument36 pagesOptomap Af Diagnostic AtlasanamariaboariuNo ratings yet
- Clinical Ophthalmology Dadapeer 23 28Document6 pagesClinical Ophthalmology Dadapeer 23 28AntaraaNo ratings yet
- Photography Exam SoiDocument3 pagesPhotography Exam Soiapi-355648573No ratings yet
- 4fcolor Theory: 1 VGD - Headwaters CollegeDocument17 pages4fcolor Theory: 1 VGD - Headwaters CollegeAndroel LaemunNo ratings yet
- MalingeringDocument4 pagesMalingeringAnnamalai OdayappanNo ratings yet
- Diabetic Eye Disease ExplainedDocument35 pagesDiabetic Eye Disease Explainedruwan555No ratings yet
- Elements and Principle of ArtDocument37 pagesElements and Principle of ArtPrince RhaegarNo ratings yet
- Spirit 4K: High-Performance Film Scanner With Bones and DatacineDocument8 pagesSpirit 4K: High-Performance Film Scanner With Bones and DatacineJustinNo ratings yet
- Colored Pencil TechniquesDocument7 pagesColored Pencil TechniquesKiana Tehrani29% (7)
- Ñáç' Ã F'Å N Oéîk Q : Small, Compact and Versatile Improved Image Quality and Color Reproduction Flexible and EfficientDocument2 pagesÑáç' Ã F'Å N Oéîk Q : Small, Compact and Versatile Improved Image Quality and Color Reproduction Flexible and EfficientPc FastNo ratings yet
- Canon RF 1200mm f/8 L IS USM LensDocument2 pagesCanon RF 1200mm f/8 L IS USM LensNikonRumors100% (1)
- الدكتور سامي عطا دعسان استشاري طب وجراحة العيون والقرنية مركز دعسان للعيون medics index member 7122010Document6 pagesالدكتور سامي عطا دعسان استشاري طب وجراحة العيون والقرنية مركز دعسان للعيون medics index member 7122010jordanmedicsNo ratings yet
- ONYX Quality Evaluation PDFDocument1 pageONYX Quality Evaluation PDFMarek Jaroszewicz0% (1)
- M8. Introduction to GIMP in 40 CharactersDocument40 pagesM8. Introduction to GIMP in 40 CharactersAnan Guidel AnanNo ratings yet
- TERRAGEN DOFTutorialDocument14 pagesTERRAGEN DOFTutorialCresencio TurpoNo ratings yet
- Departemen Ilmu Kesehatan Mata Fakultas Kedokteran Universitas Padjadjaran Pusat Mata Nasional Rumah Sakit Mata Cicendo BandungDocument11 pagesDepartemen Ilmu Kesehatan Mata Fakultas Kedokteran Universitas Padjadjaran Pusat Mata Nasional Rumah Sakit Mata Cicendo BandungBambang RinandiNo ratings yet
- Colour Code Microsoft Excel WorksheetDocument8 pagesColour Code Microsoft Excel WorksheetVivek Kumar RaiNo ratings yet
- Crime Scene PhotoDocument4 pagesCrime Scene PhotoLhine KiwalanNo ratings yet
- Dickman - Delicious Food Photography (Sample)Document20 pagesDickman - Delicious Food Photography (Sample)Alexander Domoulin100% (1)
- Photoshop: Designing Graphics For The WebDocument27 pagesPhotoshop: Designing Graphics For The WebPhilip Jayson L. LestojasNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Secure Love: Create a Relationship That Lasts a LifetimeFrom EverandSecure Love: Create a Relationship That Lasts a LifetimeRating: 5 out of 5 stars5/5 (17)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)