Professional Documents
Culture Documents
Eczema and Heart Disease
Uploaded by
anonCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Eczema and Heart Disease
Uploaded by
anonCopyright:
Available Formats
RESEARCH
Severe and predominantly active atopic eczema in adulthood
and long term risk of cardiovascular disease: population based
cohort study
Richard J Silverwood,1 Harriet J Forbes,1 Katrina Abuabara,2 Anna Ascott,3 Morten Schmidt,4 5
Sigrún A J Schmidt,4 Liam Smeeth,1 Sinéad M Langan1
1
Faculty of Epidemiology and ABSTRACT outcomes. Additional adjustment for cardiovascular
Population Health, London OBJECTIVE risk factors as potential mediators partially attenuated
School of Hygiene and Tropical To investigate whether adults with atopic eczema are the point estimates, though associations persisted for
Medicine, London WC1E 7HT,
UK at an increased risk of cardiovascular disease and severe atopic eczema.
2
Program for Clinical Research, whether the risk varies by atopic eczema severity and CONCLUSIONS
Department of Dermatology, condition activity over time. Severe and predominantly active atopic eczema are
University of California, San
Francisco School of Medicine, DESIGN associated with an increased risk of cardiovascular
San Francisco, CA, USA Population based matched cohort study. outcomes. Targeting cardiovascular disease
3
Royal Sussex County Hospital, SETTING prevention strategies among these patients should be
Brighton, UK considered.
4
UK electronic health records from the Clinical Practice
Department of Clinical
Epidemiology, Aarhus University
Research Datalink, Hospital Episode Statistics, and data
Hospital, Aarhus, Denmark from the Office for National Statistics, 1998–2015. Introduction
5
Department of Cardiology, PARTICIPANTS Atopic eczema affects up to 10% of adults and is
Regional Hospital West Jutland,
Adults with a diagnosis of atopic eczema, matched becoming more common worldwide.1 It is caused by
Herning, Denmark both skin barrier and immune system defects, and there
(on age, sex, general practice, and calendar time) to
Correspondence to: S M Langan is increasing evidence that the systemic inflammatory
Sinead.Langan@lshtm.ac.uk up to five patients without atopic eczema.
component of atopic eczema may contribute to other
Additional material is published MAIN OUTCOME MEASURES
online only. To view please visit conditions, including cardiovascular outcomes.2 Given
Cardiovascular outcomes (myocardial infarction,
the journal online. the prevalence of atopic eczema, even a small increase
unstable angina, heart failure, atrial fibrillation,
Cite this as: BMJ 2018;361:k1786 in cardiovascular risk would be important from a
http://dx.doi.org/10.1136/bmj.k1786 stroke, and cardiovascular death).
public health perspective.
Accepted: 11 April 2018 RESULTS Mixed findings have been reported in cohort
387 439 patients with atopic eczema were matched to studies assessing associations between atopic eczema
1 528 477 patients without atopic eczema. The median and acute cardiovascular outcomes from Taiwan,
age was 43 at cohort entry and 66% were female. Denmark, and the USA.3-5 It is unclear if any increased
Median follow-up was 5.1 years. Evidence of a 10%
risk is explained by increased cardiovascular risk
to 20% increased hazard for the non-fatal primary
factors in patients with atopic eczema.3 In studies
outcomes for patients with atopic eczema was found by
assessing the association between atopic eczema and
using Cox regression stratified by matched set. There
acute cardiovascular outcomes where temporality
was a strong dose-response relation with severity of
can be inferred, key data on important lifestyle and
atopic eczema. Patients with severe atopic eczema had
anthropometric confounders, such as body mass index
a 20% increase in the risk of stroke (hazard ratio 1.22,
and smoking, are largely unavailable. Atopic eczema
99% confidence interval 1.01 to 1.48), 40% to 50%
is a relapsing and remitting condition which varies
increase in the risk of myocardial infarction, unstable
angina, atrial fibrillation, and cardiovascular death, and in severity and eczema activity, and it is also unclear
70% increase in the risk of heart failure (hazard ratio whether the potential association differs by these
1.69, 99% confidence interval 1.38 to 2.06). Patients characteristics. Estimates of the spectrum of atopic
with the most active atopic eczema (active >50% of eczema severity vary depending on the approach used
follow-up) were also at a greater risk of cardiovascular to define severity.6 Previous reports suggest that around
30% of patients with atopic eczema would be classified
as having moderate or severe atopic eczema.7-9
WHAT IS ALREADY KNOWN ON THIS TOPIC We therefore examined whether adults with atopic
Atopic eczema is a common systemic inflammatory condition eczema are at a greater risk of cardiovascular events.
Previous studies have reported mixed findings for the association between We also investigated whether the risk of cardiovascular
atopic eczema and cardiovascular outcomes disease varied by atopic eczema severity and eczema
activity over time.
WHAT THIS STUDY ADDS
Severe and predominantly active atopic eczema are associated with an increased
Methods
risk of cardiovascular outcomes
Study design and setting
Patients with severe atopic eczema were at a 20% increased risk of stroke, 35% We undertook a cohort study with data from the
to 40% increased risk of unstable angina, myocardial infarction, atrial fibrillation, UK Clinical Practice Research Datalink (CPRD),
and cardiovascular death, and 70% increased risk of heart failure linked to Hospital Episode Statistics inpatient
the bmj| BMJ 2018;361:k1786 | doi: 10.1136/bmj.k1786 1
RESEARCH
data, Office for National Statistics mortality data, diagnosis of atopic eczema; before their diagnosis of
and index of multiple deprivation data. CPRD is a atopic eczema, these patients were not considered
database of prospectively collected primary care to have atopic eczema and were therefore eligible to
records from general practitioners using Vision contribute to unexposed person time. Patients with
software; approximately 9% of the UK population are a diagnosis of atopic eczema who did not go on to
represented in the database.10 11 Data are anonymised meet the full definition of atopic eczema (at least one
and include diagnoses (coded using Read codes), diagnosis code and two treatment codes on separate
prescriptions (coded using British National Formulary dates) were also in the pool of eligible unexposed
codes), and referrals to specialists. Approximately patients up until the date of their atopic eczema
80% of CPRD practices registered in England have diagnosis code. Removing these patients from the pool
consented to their patients’ primary care records of eligible unexposed patients at the point of diagnosis
being linked to other data sources. Hospital Episode rather than allowing them to remain until they met
Statistics include all NHS inpatient hospital stays in the full validated definition of atopic eczema ensured
England since 1997, with diagnoses coded using greater certainty that the pool of unexposed patients
ICD-10 (international classification of diseases, 10th did not have atopic eczema. Patients could only be
revision) codes and procedures coded according to sampled as unexposed once during the study (ie,
OPCS Classification of Interventions and Procedures sampling without replacement).
codes. Office for National Statistics linked mortality
data contain the underlying cause of death, recorded Exclusions
on the death certificate, along with up to 15 other After matching, we excluded patients with codes
recorded causes of death. Causes are coded using indicating previous or current cardiovascular disease,
ICD-9 codes before January 2001 and ICD-10 codes including all the main outcome codes plus further
thereafter. Index of multiple deprivation data contain codes including history (or possible history) of each
quintiles of deprivation based on the patient’s outcome, epidural or subdural strokes, subarachnoid
postcode. For this study, data were extracted from the haemorrhagic strokes, and risk factors for subarachnoid
January 2016 CPRD build and the Set 12 linked data. haemorrhage, such as cerebral aneurysms in the circle
of Willis or arteriovenous malformations.
Study population
Adult patients (aged ≥18) contributing to CPRD Defining follow-up
between 2 January 1998 and 31 March 2015, with Follow-up for exposed patients began at the latest of:
linked Hospital Episode Statistics data were eligible for 2 January 1998, the date the individual turned 18
inclusion in the study. years old, the date of diagnosis of atopic eczema, or
the start of CPRD follow-up plus 365 days (to ensure a
Defining patients with atopic eczema cardiovascular outcome diagnosis was incident and not
The exposed cohort included all patients with atopic recorded retrospectively after registration at a general
eczema. We defined atopic eczema onset as the practice).13 Follow-up for unexposed individuals began
latest of an atopic eczema diagnosis and two atopic at the start date of their matched patient with atopic
eczema treatments (on separate dates), consistent eczema. Follow-up ended at the earliest of study end
with a validation study showing a positive predictive date, death (using Office for National Statistics date or,
value in adults of 82% (95% confidence interval if missing, CPRD death date), transfer out of practice,
73% to 89%).12 Atopic eczema diagnostic codes were practice last collection date, or the patient developing
identified in CPRD (using Read codes) and Hospital an outcome of interest. For analyses concerning
Episode Statistics (using ICD-10 codes in the primary stroke only, follow-up ended on the earliest of study
diagnosis field of any episode). Treatments included end date, death, transfer out of practice, practice last
atopic eczema related prescriptions from primary care: collection date, the patient developing an outcome of
emollients, topical and oral corticosteroids, tacrolimus interest, or the date of an epidural or subdural stroke,
and systemic immunosuppressants (methotrexate, subarachnoid haemorrhagic stroke, or risk factor for
ciclosporin, mycophenolate mofetil, or azathioprine), subarachnoid haemorrhage (such as embolisation of
and phototherapy records from CPRD or OPCS cerebral artery and non-ruptured cerebral aneurysm).
Classification of Interventions and Procedures codes in Patients contributing at least one day of follow-up were
Hospital Episode Statistics. included in the study.
Defining matched unexposed patients Severe and predominantly active atopic eczema
For each patient with atopic eczema, we randomly Severity of atopic eczema was defined as a time-
matched up to five patients by age (within 15 years), updated variable for patients with atopic eczema.
sex, general practice, and calendar time at cohort Patients with atopic eczema were considered to have
entry. These unexposed patients were required to have mild conditions by default. They were classified as
at least one year of follow-up in CPRD and no history having moderate atopic eczema at the first of: a second
of atopic eczema when matched. Any patients with a potent topical corticosteroid treatment within one
diagnosis of atopic eczema were included in the pool year or a first calcineurin inhibitor treatment. Patients
of eligible unexposed patients until the date of their were classified as having severe atopic eczema at the
2 doi: 10.1136/bmj.k1786 | BMJ 2018;361:k1786 | the bmj
RESEARCH
first of: a systemic immunosuppressant treatment; their prescription and three months after the end of the
a phototherapy code in CPRD or Hospital Episode prescription. Further details regarding the definition
Statistics; or a referral for atopic eczema. Once defined of these variables can be found in the supplementary
as moderate, patients with atopic eczema remained material.
as such unless they developed severe atopic eczema;
once defined as severe, patients with atopic eczema Statistical analysis
remained as such, similar to established approaches Primary analyses
for defining severity in psoriasis studies.14 At any given The characteristics of those with and without atopic
point during follow-up, patients with atopic eczema eczema (at cohort entry) were described. We used Cox
therefore belonged to one of three severity categories: regression stratified by matched set (matched on age at
mild, moderate, or severe. cohort entry, sex, general practice, and date at cohort
Atopic eczema activity was assessed over time. entry) with current age as the underlying timescale
Active atopic eczema started at the latest of two CPRD to generate hazard ratios for the association between
or Hospital Episode Statistics atopic eczema records atopic eczema and each cardiovascular outcome (the
(either diagnoses or treatment) appearing within any unadjusted model). Subsequent multivariable analyses
one year period. Active atopic eczema was assumed adjusted for current calendar period (1997-99, 2000-
to last for 12 months, unless another atopic eczema 04, 2005-09, 2010-15), current time since diagnosis
record appeared, in which case its duration was (0-4, 5-9, 10-14, 15-19, ≥20 years), socioeconomic
prolonged for another 12 months. Patients with atopic status, and time varying asthma (the adjusted model).
eczema were subsequently split into three categories The adjusted model was further adjusted for variables
for analysis: those who never had active atopic eczema which may have been on the causal pathway (ie,
during follow-up, those who had active atopic eczema mediators) between atopic eczema and cardiovascular
for less than 50% of follow-up, and those who had outcomes (smoking and body mass index at cohort
active atopic eczema for at least 50% of follow-up. entry, and time varying diabetes, hypertension,
hyperlipidaemia, depression and anxiety, and severe
Cardiovascular outcomes alcohol use) (the mediation model). Patients with
We identified the following individual cardiovascular missing body mass index, smoking, or index of multiple
diseases in CPRD and Hospital Episode Statistics deprivation data were excluded. These data are likely
(primary diagnosis fields of any episode): myocardial to be missing not at random (as missingness is likely
infarction, unstable angina, heart failure, atrial to depend on the actual values). Multiple imputation
fibrillation, stroke (ischaemic, haemorrhagic, or would therefore not be appropriate. Complete case
unspecified), and cardiovascular death. Secondary analysis is valid where the missingness is independent
outcomes included coronary revascularisation of each of the cardiovascular outcomes, conditional
procedures, identified in OPCS Classification of on the model covariates.16 We used 99% confidence
Interventions and Procedures data. Deaths from intervals and an implied 1% level of statistical
cardiovascular disease were identified from Office for significance to reduce the risk of type 1 error.
National Statistics data, defined as any ICD-9 or ICD- Incidence rates of each cardiovascular outcome
10 code related to cardiovascular disease recorded as in the patients with atopic eczema were estimated
a cause of death. by using the data in our sample. Incidence rates of
each cardiovascular outcome among patients without
Covariates atopic eczema (which cannot be reliably estimated
We used a directed acyclic graph to inform the from the sample owing to the matching) were then
identification of covariates and mediators and to estimated by multiplying the incidence rate in the
avoid collider bias (see supplementary figure S1).15 patients with atopic eczema by our corresponding
The covariates included current age, calendar period estimated hazard ratio (after having first inverted it
(1997-99, 2000-04, 2005-09, 2010-15), time since so that it compares unexposed with exposed). We
diagnosis (0-4, 5-9, 10-14, 15-19, ≥20 years), and calculated attributable risks as the difference between
socioeconomic status (quintiles of 2015 index of these exposure group specific incidence rates. The
multiple deprivation). Patients were defined as population attributable risk of each cardiovascular
having diabetes mellitus (type 1, type 2, or missing), outcome was estimated by using the estimated hazard
hypertension, hyperlipidaemia, depression, anxiety, ratio and assuming the prevalence of atopic eczema
or asthma on the date of their first ever Read code in to be 10%.17
CPRD for these conditions, which may have been after
cohort entry, as a time updated variable. Body mass Secondary analyses
index (according to WHO categories) and smoking We repeated the analyses within strata of sex, current
status (current smoker, former smoker, or non-smoker) asthma status, and current age (18-39, 40-59, and
were defined at cohort entry. Patients were defined as ≥60) to explore potential effect modification. We
having severe alcohol use at the first of: high alcohol also repeated the analysis with alternative exposure
use code or treatment for severe alcohol use recorded definitions, where atopic eczema was categorised
in CPRD. Patients were defined as exposed to high dose based on severity and, separately, on category of
(≥20 mg/day) oral corticosteroids for the duration of eczema activity.
the bmj| BMJ 2018;361:k1786 | doi: 10.1136/bmj.k1786 3
RESEARCH
Table 1 | Sensitivity analyses
Sensitivity analysis Justification
The activity analysis was repeated, restricted to patients with at least five To explore any potential bias caused by patients with
years of follow-up atopic eczema with short follow-up periods being more
likely to have either none or all of their follow-up with
active atopic eczema
The primary analysis was repeated on an incident atopic eczema cohort Covariates measured at entry precede atopic eczema on-
(exposed patients defined as those joining the cohort when they first fulfil our set so will not be on the causal pathway between atopic
diagnostic criteria and after the start of the study period) eczema and cardiovascular outcomes
The primary analysis was repeated on patients with at least one consultation To exclude practice non-attenders
with their doctor in the year before cohort entry
The primary analysis was repeated on a redefined cohort, where the pool of To explore the sensitivity of the results to the definition of
unexposed patients also included patients with an atopic eczema diagnosis the exposure
but without two further treatments for the entire duration of their follow-up
and patients in the exposed cohort (with an atopic eczema diagnosis and two
further treatments) were included as unexposed up until their cohort entry (ie,
the latest of their atopic eczema diagnosis and their two further treatments)
The primary analysis was repeated on a second redefined cohort where To explore the sensitivity of the results to the definition of
exposed patients were those with an atopic eczema diagnosis only (ie, without the exposure
requiring two atopic eczema treatments), and these patients were eligible for
the unexposed cohort up until their atopic eczema diagnosis (some patients
may have childhood atopic eczema, but may not have treatment codes record-
ed if they registered at the practice during adulthood, and therefore may be
erroneously excluded from the exposed cohort in the primary analysis)
The primary analysis was repeated on a subset of patients registered from Data on covariates, particularly body mass index and
2007 onwards smoking, would be expected to be more complete, thus
reducing any selection bias owing to missing data
The primary analysis was repeated on a subset of patients registered from To examine whether the omission of this covariate in the
2007 onwards, additionally adjusting for ethnic group (white, South Asian, primary analysis may have introduced bias
black, other, or mixed, identified from Clinical Practice Research Datalink and
Hospital Episode Statistics data using a previously developed algorithm)18
The primary analysis (mediation model only) was repeated with additional To examine whether the omission of this covariate in the
adjustment for time updated use of high dose corticosteroids primary analysis may have introduced bias
Sensitivity analyses and model checking Patient involvement
Table 1 shows the series of sensitivity analyses we The research questions, design, conduct, and initial
conducted. We also checked the proportional hazards results and interpretation of the findings of this study
assumption in all the primary analysis models through have been overseen by the Wellcome Senior Clinical
plots of the Schöenfeld residuals. Fellowship steering committee, which includes lay
representation. No patients were asked to advise on
interpretation or writing up of results. There are no
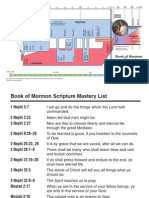
Atopic eczema diagnosis in Clinical Practice Research Datalink (CPRD) plans to disseminate the results of the research to
or Hospital Episode Statistics (HES) (n=1 139 527)
study participants.
Patients without any follow-up as adult, after atopic
eczema diagnosis, or during study period (n=459 242)
Results
Patients with an atopic eczema diagnosis in CPRD or HES and some eligible follow-up (n=680 285) Figure 1 shows that in total, 466 883 exposed and
2 169 123 unexposed patients were successfully
Patients without two atopic eczema treatments anywhere in their records (n=151 680)
matched and were eligible for cohort entry. Of these,
Atopic eczema diagnosis and two atopic eczema 517 444 (19.6%) were excluded from subsequent
treatments ever in CPRD (on separate days) (n=528 605) analyses as they did not have complete data on the
analysis variables (19.2% missing body mass index,
Match to unexposed patients 5.3% missing smoking, and 0.1% missing index of
multiple deprivation), and a further 202 646 (7.7%)
Patients with atopic eczema with no eligible unexposed matches (n=20 438)
patients were excluded as they had no remaining
Exposed and unexposed cohort (n=2 990 109): matches. This left a final analysis sample of 387 439
Exposed patients (n=508 167) exposed and 1 528 477 unexposed patients. Table 2
Unexposed patients (n=2 481 942)
and supplementary table S1 show that distributions
Excluded patients (n=354 103): of variables did not differ substantially between those
Patients with a history of cardiovascular disease in CPRD or HES (n=186 033) included in the final analysis sample and the overall
Other exclusions, including no eligible follow-up time (n=15 686)
Patients without any remaining matches (n=152 384) sample, except for a somewhat higher proportion
of exposed patients (20.2% v 17.7%), more female
Exposed and unexposed cohort, no history of cardiovascular disease at cohort entry, valid patients (66.0% v 60.0%), and fewer of the very
matched set (n=2 636 006):
Exposed patients (n=466 883) youngest (aged 18–19) patients (6.5% v 14.5%) in the
Unexposed patients (n=2 169 123) analysis sample. Median follow-up was 5.1 years and
over the follow-up period, 19 700 (5.1%) patients with
Fig 1 | Flowchart for cohort study, 1998-2015 atopic eczema experienced severe atopic eczema.
4 doi: 10.1136/bmj.k1786 | BMJ 2018;361:k1786 | the bmj
RESEARCH
Table 2 | Covariate summary statistics for patients with complete data on all analysis Effect estimates were substantially stronger in
variables and belonging to valid matched sets.* Values are mean (percentage) unless patients with severe atopic eczema, in particular for
stated otherwise unstable angina (hazard ratio 1.48, 99% confidence
Without atopic eczema With atopic eczema interval 1.08 to 2.03 in the adjusted model) and heart
Characteristic (n=1 528 477) (79.8%)) (n=387 439 (20.2%)) Total (n=1 915 916) failure (1.69, 1.38 to 2.06) (see fig 2 and supplementary
Follow-up (years) table S5). Similar findings were observed for patients
Median (interquartile 4.9 (2.0-9.6) 5.7 (2.4-10.3) 5.1 (2.0-9.8)
range)
with the most active atopic eczema, in particular for
At entry to cohort unstable angina (1.49, 1.30 to 1.72) and heart failure
Sex: (1.43, 1.30 to 1.56) (see fig 3 and supplementary table
Male 511 676 (33.5) 139 908 (36.1) 651 584 (34.0) S6).
Female 1 016 801 (66.5) 247 531 (63.9) 1 264 332 (66.0)
Age (years): Sensitivity analyses
18-19 87 600 (5.7) 36 392 (9.4) 123 992 (6.5)
Restricting the activity analysis to patients with at least
20-29 275 632 (18.0) 66 156 (17.1) 341 788 (17.8)
30-39 315 206 (20.6) 70 222 (18.1) 385 428 (20.1) five years of follow-up (43% of all patients) generally
40-49 272 436 (17.8) 61 898 (16.0) 334 334 (17.5) gave similar findings, though results for cardiovascular
50-59 243 469 (15.9) 55 294 (14.3) 298 763 (15.6) death changed more markedly, with the estimates for
60-69 195 936 (12.8) 49 420 (12.8) 245 356 (12.8) the never and <50% activity groups attenuated towards
70-79 104 132 (6.8) 33 837 (8.7) 137 969 (7.2) the null (see supplementary table S7). Results from the
≥80 34 066 (2.2) 14 220 (3.7) 48 286 (2.5)
analysis with the incident atopic eczema cohort (54%
Index of multiple depri-
vation: of those in the primary analysis) were very similar to
1 (least deprived) 370 953 (24.3) 94 223 (24.3) 465 176 (24.3) those in the primary analysis (see supplementary table
2 332 853 (21.8) 84 297 (21.8) 417 150 (21.8) S8). When analyses were restricted to patients with
3 312 836 (20.5) 78 603 (20.3) 391 439 (20.4) at least one consultation with their doctor in the year
4 273 332 (17.9) 69 223 (17.9) 342 555 (17.9)
before cohort entry (83% of all patients) the estimated
5 (most deprived) 238 503 (15.6) 61 093 (15.8) 299 596 (15.6)
Body mass index:
hazard ratios were attenuated slightly relative to those
Underweight 45 488 (3.0) 11 590 (3.0) 57 078 (3.0) in the primary analysis (see supplementary table S9).
Normal weight 709 903 (46.4) 174 234 (45.0) 884 137 (46.1) The results from the analyses with the two redefined
Overweight 484 434 (31.7) 123 352 (31.8) 607 786 (31.7) patient cohorts differed somewhat from those in the
Obese 288 652 (18.9) 78 263 (20.2) 366 915 (19.2) primary analysis (see supplementary tables S10 and
Smoking status:
S11); however, all confidence intervals included the
Non 699 570 (45.8) 168 221 (43.4) 867 791 (45.3)
point estimate from the main analysis. Only 11% of
Current 480 780 (31.5) 116 551 (30.1) 597 331 (31.2)
Former 348 127 (22.8) 102 667 (26.5) 450 794 (23.5) patients had registrations from 2007 onwards, and
Diabetes 51 213 (3.4) 15 777 (4.1) 66 990 (3.5) this small subset of patients differed substantially
Hypertension 190 217 (12.4) 58 001 (15.0) 248 218 (13.0) from the primary analysis sample, particularly in
Hyperlipidaemia 59 376 (3.9) 19 342 (5.0) 78 718 (4.1) terms of age (younger; see supplementary table S12),
Depression 300 699 (19.7) 95 131 (24.6) 395 830 (20.7) and therefore the hazard ratios differed markedly
Anxiety 194 289 (12.7) 65 248 (16.8) 259 537 (13.5)
(see supplementary table S13). Results adjusted for
Asthma 190 728 (12.5) 91 955 (23.7) 282 683 (14.8)
Severe alcohol use 28 803 (1.9) 8730 (2.3) 37 533 (2.0)
ethnic group (restricting to the 9% of patients with
*Matched sets including one exposed patient and at least one unexposed patient. such data) were consistent with the main analysis (see
supplementary table S14), suggesting limited bias
from omission of this covariate. Results adjusted for
Table 3 shows that in the primary analysis, there was time updated use of high dose corticosteroids were
evidence of associations between atopic eczema and consistent with the main analysis (see supplementary
all cardiovascular outcomes, except for cardiovascular table S15), similarly suggesting limited bias from
death. Associations were strongest with unstable omission of this covariate.
angina (hazard ratio 1.25, 99% confidence interval
1.11 to 1.41 in the adjusted model) and heart failure Discussion
(1.19, 1.10 to 1.30), with partial attenuation in the This study shows that atopic eczema is associated
mediation model. with a moderately increased risk of non-fatal
Table 4 shows that the estimated attributable risks cardiovascular outcomes, with a dose-response
confirm the increased incidence rates of cardiovascular for atopic eczema severity and cumulated activity.
outcomes among patients with atopic eczema. Patients with severe atopic eczema were at a 20%
Attributable risks were greatest for heart failure (40 per increased risk of stroke, 40-50% increased risk
100 000, 99% confidence interval 22 to 57) and atrial of unstable angina, myocardial infarction, atrial
fibrillation (37, 15 to 55). The greatest population fibrillation, and cardiovascular death, and 70%
attributable risks were estimated for unstable angina increased risk of heart failure. The most active
(2.4%, 1.1% to 3.9%) and heart failure (1.9%, 1.0% atopic eczema group had similar findings. Estimated
to 2.9%). attributable risks confirm the increased incidence
There was no convincing evidence of effect rates of cardiovascular outcomes among patients
modification by age, sex, or current asthma status (see with atopic eczema, with population attributable
supplementary tables S2-4). risks of 2% or more for some outcomes.
the bmj| BMJ 2018;361:k1786 | doi: 10.1136/bmj.k1786 5
RESEARCH
Table 3 | Association between atopic eczema and cardiovascular outcomes. Fitted to patients with complete data for
all variables included in the models and from valid matched sets* (n=1 915 916, 1 842 759 unique patients)
Patient years Hazard ratio (99% CI)†
Variables No at risk Events Unadjusted Adjusted‡ Mediation model§
Primary outcomes
Myocardial infarction:
Unexposed 1 528 477 9 361 522 17 178 1.00 (ref) 1.00 (ref) 1.00 (ref)
Exposed 387 439 2 569 214 5561 1.10 (1.05 to 1.15) 1.06 (0.98 to 1.15) 1.04 (0.96 to 1.13)
Unstable angina:
Unexposed 1 528 477 9 392 370 7059 1.00 (ref) 1.00 (ref) 1.00 (ref)
Exposed 387 439 2 578 165 2460 1.22 (1.14 to 1.31) 1.25 (1.11 to 1.41) 1.17 (1.03 to 1.32)
Heart failure:
Unexposed 1 528 477 9 375 383 16 983 1.00 (ref) 1.00 (ref) 1.00 (ref)
Exposed 387 439 2 570 412 6441 1.21 (1.16 to 1.26) 1.19 (1.10 to 1.30) 1.17 (1.08 to 1.28)
Atrial fibrillation:
Unexposed 1 528 477 9 316 331 28 571 1.00 (ref) 1.00 (ref) 1.00 (ref)
Exposed 387 439 2 552 311 9892 1.12 (1.08 to 1.16) 1.11 (1.04 to 1.18) 1.07 (1.00 to 1.15)
Stroke:
Unexposed 1 528 477 9 361 252 21 387 1.00 (ref) 1.00 (ref) 1.00 (ref)
Exposed 387 439 2 568 749 7149 1.07 (1.03 to 1.12) 1.10 (1.02 to 1.19) 1.08 (1.00 to 1.16)
Cardiovascular death:
Unexposed 1 528 477 9 427 420 30 116 1.00 (ref) 1.00 (ref) 1.00 (ref)
Exposed 387 439 2 590 305 10 813 1.07 (1.03 to 1.11) 0.98 (0.92 to 1.06) 0.96 (0.89 to 1.03)
Secondary outcome
Coronary revascularisation:
Unexposed 1 528 477 9 358 381 16 195 1.00 (ref) 1.00 (ref) 1.00 (ref)
Exposed 387 439 2 567 932 5056 1.12 (1.07 to 1.17) 1.14 (1.05 to 1.24) 1.08 (0.99 to 1.17)
*Matched sets including one exposed patient and at least one unexposed patient.
†Estimated hazard ratios from Cox regression with current age as underlying timescale, stratified by matched set (matched on age at cohort entry, sex,
general practice, and date at cohort entry).
‡Adjusted for current calendar period (1997-99, 2000-04, 2005-09, 2010-15), time since diagnosis (0-4, 5-9, 10-14, 15-19, ≥20 years), index of
multiple deprivation at cohort entry, and time-varying asthma.
§Adjusted additionally for body mass index and smoking at cohort entry, and time-varying hyperlipidaemia, hypertension, depression, anxiety, diabetes,
and severe alcohol use.
Comparison with other studies outcomes (including angina, myocardial infarction,
Mechanistic work suggests that atopic eczema may and stroke), whereas the association with mild
be associated with increased platelet activation and atopic eczema has been either slightly protective or
decreased fibrinolysis, which may increase the risk of close to zero.3 20 This may suggest a dose-response
clotting,19 though a recent study found no association effect, an alternative pathogenesis underlying
with metabolite levels.20 The association between mild compared with severe conditions, the effect
atopic eczema and cardiovascular outcomes has been of systemic therapies used to treat severe forms of
inconsistent in the literature. Studies from Taiwanese atopic eczema, or misclassification bias owing to
populations report a 1.33-fold increased incidence the way in which patients with atopic eczema were
of stroke, rising to 1.71-fold increase in those with classified. The European and Taiwanese studies used
severe atopic eczema.4 Studies in Danish and German data from administrative databases which are likely
populations have reported positive associations to have incomplete data on potentially important
between severe atopic eczema and cardiovascular cardiovascular risk factors including body mass index,
Table 4 | Absolute incidence rates, incidence rate differences (attributable risks), and population attributable risks of cardiovascular outcomes
Estimated incidence Estimated incidence Estimated incidence Estimated population
rate* in patients with Hazard ratio Inverse hazard rate* (99% CI) in patients rate difference* attributable risk (%)
Variables atopic eczema (99% CI)† ratio (99% CI)‡ without atopic eczema (99% CI) (99% CI)§
Primary outcomes
Myocardial infarction 205 1.06 (0.98 to 1.15) 0.94 (0.87 to 1.02) 193 (178 to 209) 12 (−4 to 27) 0.6 (−0.2 to 1.5)
Unstable angina 89 1.25 (1.11 to 1.41) 0.80 (0.71 to 0.90) 71 (63 to 80) 18 (9 to 26) 2.4 (1.1 to 3.9)
Heart failure 248 1.19 (1.10 to 1.30) 0.84 (0.77 to 0.91) 208 (191 to 226) 40 (22 to 57) 1.9 (1.0 to 2.9)
Atrial fibrillation 366 1.11 (1.04 to 1.18) 0.90 (0.85 to 0.96) 329 (311 to 351) 37 (15 to 55) 1.1 (0.4 to 1.8)
Stroke 276 1.10 (1.02 to 1.19) 0.91 (0.84 to 0.98) 251 (232 to 270) 25 (6 to 44) 1.0 (0.2 to 1.9)
Cardiovascular death 440 0.98 (0.92 to 1.06) 1.02 (0.94 to 1.09) 449 (414 to 480) −9 (−40 to 26) −0.2 (−0.8 to 0.6)
Secondary outcome
Coronary revascularisation 179 1.14 (1.05 to 1.24) 0.88 (0.81 to 0.95) 158 (145 to 170) 21 (9 to 34) 1.4 (0.5 to 2.3)
*Per 100 000 person years
†Adjusted for current calendar period (1997-99, 2000-04, 2005-09, 2010-15), time since diagnosis (0-4, 5-9, 10-14, 15-19, ≥20 years), index of multiple deprivation at cohort entry, and time-
varying asthma.
‡Comparing patients without atopic eczema to patients with atopic eczema.
§Estimated as P(HR-1)/(1+P(HR-1)) where P, the prevalence of atopic eczema, is assumed to be 10% and HR is the estimated hazard ratio‡.17
6 doi: 10.1136/bmj.k1786 | BMJ 2018;361:k1786 | the bmj
RESEARCH
Unadjusted Adjusted* Mediation model†
Hazard ratio Hazard ratio Hazard ratio Hazard ratio Hazard ratio Hazard ratio
(99% CI) (99% CI) (99% CI) (99% CI) (99% CI) (99% CI)
Myocardial infarction
Mild 1.03 (0.96 to 1.09) 1.00 (0.91 to 1.10) 1.00 (0.91 to 1.10)
Moderate 1.15 (1.07 to 1.23) 1.11 (1.01 to 1.23) 1.07 (0.97 to 1.18)
Severe 1.46 (1.21 to 1.74) 1.41 (1.15 to 1.71) 1.37 (1.12 to 1.68)
Unstable angina
Mild 1.22 (1.11 to 1.33) 1.25 (1.10 to 1.43) 1.19 (1.04 to 1.37)
Moderate 1.20 (1.08 to 1.34) 1.22 (1.06 to 1.42) 1.11 (0.96 to 1.29)
Severe 1.47 (1.10 to 1.97) 1.48 (1.08 to 2.03) 1.41 (1.02 to 1.95)
Heart failure
Mild 1.12 (1.05 to 1.19) 1.12 (1.02 to 1.23) 1.12 (1.02 to 1.24)
Moderate 1.27 (1.19 to 1.35) 1.25 (1.14 to 1.38) 1.20 (1.09 to 1.33)
Severe 1.71 (1.43 to 2.05) 1.69 (1.38 to 2.06) 1.67 (1.36 to 2.05)
Atrial fibrillation
Mild 1.05 (1.00 to 1.10) 1.05 (0.97 to 1.13) 1.02 (0.95 to 1.10)
Moderate 1.18 (1.12 to 1.24) 1.17 (1.08 to 1.27) 1.12 (1.04 to 1.21)
Severe 1.40 (1.21 to 1.62) 1.38 (1.17 to 1.62) 1.35 (1.14 to 1.59)
Stroke
Mild 1.03 (0.98 to 1.09) 1.07 (0.98 to 1.16) 1.06 (0.97 to 1.15)
Moderate 1.11 (1.04 to 1.18) 1.14 (1.04 to 1.25) 1.09 (1.00 to 1.20)
Severe 1.19 (1.00 to 1.42) 1.22 (1.01 to 1.48) 1.20 (0.99 to 1.46)
Cardiovascular death
Mild 0.97 (0.92 to 1.02) 0.90 (0.84 to 0.98) 0.90 (0.83 to 0.98)
Moderate 1.15 (1.09 to 1.21) 1.06 (0.98 to 1.15) 1.01 (0.93 to 1.10)
Severe 1.49 (1.29 to 1.73) 1.38 (1.17 to 1.62) 1.30 (1.10 to 1.53)
Coronary revascularisation
Mild 1.09 (1.02 to 1.16) 1.12 (1.02 to 1.23) 1.08 (0.98 to 1.19)
Moderate 1.11 (1.04 to 1.20) 1.14 (1.03 to 1.26) 1.05 (0.95 to 1.17)
Severe 1.42 (1.17 to 1.71) 1.47 (1.19 to 1.81) 1.36 (1.10 to 1.69)
0.8 1.0 1.5 2.0 0.8 1.0 1.5 2.0 0.8 1.0 1.5 2.0
Fig 2 | Association between atopic eczema and cardiovascular outcomes, by severity of atopic eczema versus no eczema. *Adjusted for current
calendar period (1997-99, 2000-04, 2005-09, 2010-15), time since diagnosis (0-4, 5-9, 10-14, 15-19, ≥20 years), index of multiple deprivation at
cohort entry, and time-varying asthma. †Adjusted additionally for body mass index and smoking at cohort entry, and time-varying hyperlipidaemia,
hypertension, depression, anxiety, diabetes, and severe alcohol use
smoking, and alcohol consumption. These factors with linked data on hospital stays and cause specific
may be more prevalent in patients with atopic eczema mortality.23 24 Previous studies have shown that this
and could therefore contribute to an increased risk of population is largely representative of the general UK
cardiovascular outcomes.21 Our cohort study is one population.11 We used a validated algorithm to identify
of the few longitudinal studies to have adjusted for atopic eczema and our approach to defining atopic
these risk factors. Silverberg et al adjusted for body eczema severity showed a similar distribution of severity
mass index, smoking, alcohol consumption, and to the literature.12 14 For most of our study population,
physical activity in three cross sectional surveys in we had data on body mass index, smoking, and
USA populations, and still found strong associations severe alcohol use, allowing us to adjust for potential
between atopic eczema and angina, coronary artery mediators between atopic eczema and cardiovascular
disease, myocardial infarction, and stroke.22 However, outcomes. We used a directed acyclic graph to identify
these studies were cross sectional, and misclassification covariates and mediators, and to avoid collider bias.15
is likely owing to exposures and outcomes being self The study outcomes require medical intervention and
reported. A study in a specific USA population found therefore presentation in primary or secondary care,
no noticeable association between self reported atopic meaning that ascertainment bias is unlikely to be a
eczema and either myocardial infarction or stroke in problem. One exception may be asymptomatic atrial
female nurses.5 fibrillation, though this is only a minor proportion
of the total patients with atrial fibrillation so any
Strengths and weaknesses of this study ascertainment bias is likely to be limited.
This is the largest study to assess the association Limitations of the study, inherent to most large
between atopic eczema and major cardiovascular observational studies, include the possibility for
events. It is also the first study based on primary confounding, bias, and missing data. It is not possible
care data, meaning that our results are generalisable to separate the effects of therapy and severity, owing
to a broad population with atopic eczema. We used to the nature of routinely collected data sources and
population based data from UK general practices observational settings whereby those with more
the bmj| BMJ 2018;361:k1786 | doi: 10.1136/bmj.k1786 7
RESEARCH
Unadjusted Adjusted* Mediation model†
Hazard ratio Hazard ratio Hazard ratio Hazard ratio Hazard ratio Hazard ratio
(99% CI) (99% CI) (99% CI) (99% CI) (99% CI) (99% CI)
Myocardial infarction
Never 0.96 (0.86 to 1.08) 0.92 (0.80 to 1.06) 0.95 (0.83 to 1.10)
<50% 1.00 (0.93 to 1.07) 0.95 (0.86 to 1.05) 0.94 (0.85 to 1.04)
≥50% 1.29 (1.20 to 1.38) 1.20 (1.09 to 1.32) 1.16 (1.05 to 1.27)
Unstable angina
Never 0.86 (0.72 to 1.03) 0.89 (0.72 to 1.10) 0.88 (0.70 to 1.10)
<50% 1.11 (1.01 to 1.23) 1.12 (0.97 to 1.29) 1.05 (0.91 to 1.22)
≥50% 1.56 (1.40 to 1.73) 1.49 (1.30 to 1.72) 1.36 (1.18 to 1.58)
Heart failure
Never 0.89 (0.78 to 1.01) 0.88 (0.76 to 1.03) 0.92 (0.79 to 1.08)
<50% 0.99 (0.93 to 1.07) 0.94 (0.85 to 1.05) 0.96 (0.86 to 1.07)
≥50% 1.55 (1.46 to 1.65) 1.43 (1.30 to 1.56) 1.37 (1.24 to 1.50)
Atrial fibrillation
Never 0.94 (0.86 to 1.04) 0.93 (0.83 to 1.05) 0.93 (0.83 to 1.05)
<50% 1.04 (0.99 to 1.10) 1.02 (0.94 to 1.10) 1.00 (0.92 to 1.08)
≥50% 1.27 (1.21 to 1.34) 1.22 (1.13 to 1.31) 1.17 (1.08 to 1.26)
Stroke
Never 1.07 (0.96 to 1.18) 1.10 (0.97 to 1.24) 1.12 (0.99 to 1.27)
<50% 0.93 (0.87 to 0.99) 0.94 (0.86 to 1.03) 0.93 (0.85 to 1.02)
≥50% 1.24 (1.17 to 1.32) 1.24 (1.14 to 1.35) 1.19 (1.09 to 1.30)
Cardiovascular death
Never 1.36 (1.24 to 1.48) 1.23 (1.10 to 1.38) 1.27 (1.13 to 1.43)
<50% 0.75 (0.71 to 0.80) 0.67 (0.61 to 0.73) 0.66 (0.60 to 0.72)
≥50% 1.32 (1.26 to 1.39) 1.16 (1.07 to 1.25) 1.10 (1.02 to 1.19)
Coronary revascularisation
Never 0.90 (0.80 to 1.01) 0.90 (0.79 to 1.04) 0.91 (0.79 to 1.05)
<50% 1.09 (1.02 to 1.16) 1.09 (0.99 to 1.21) 1.05 (0.94 to 1.16)
≥50% 1.27 (1.18 to 1.37) 1.26 (1.14 to 1.40) 1.16 (1.05 to 1.29)
0.6 0.8 1.0 1.5 2.0 0.6 0.8 1.0 1.5 2.0 0.6 0.8 1.0 1.5 2.0
Fig 3 | Association between atopic eczema and cardiovascular outcomes, by activity of atopic eczema versus no eczema. *Adjusted for current
calendar period (1997-99, 2000-04, 2005-09, 2010-15), time since diagnosis (0-4, 5-9, 10-14, 15-19, ≥20 years), index of multiple deprivation at
cohort entry, and time-varying asthma. †Adjusted additionally for body mass index and smoking at cohort entry, and time-varying hyperlipidaemia,
hypertension, depression, anxiety, diabetes, and severe alcohol use
severe atopic eczema are given specific treatments, studies. Assessing major long term health outcomes
and where those treatments might be continued for in a condition such as atopic eczema that frequently
long periods. Patients were matched within 15 year starts in early childhood may be challenging owing to
age intervals as finer age matching led to a noticeable possible survival bias; the prevalent cohort would have
loss of patients with atopic eczema, who did not have fewer patients rapidly developing the cardiovascular
any eligible matches. However, age was accounted for outcomes (those at greatest risk) as they may not
as the underlying timescale in all analyses, closely be eligible for sampling.25 26 As survival bias would
adjusting for the confounding effects of age. Exclusion bias the association between atopic eczema and
of patients without complete data on body mass index, cardiovascular disease towards the null, it cannot
smoking, and index of multiple deprivation reduced explain our findings, and could potentially have led
the sample by nearly 20%. However, we believe that to underestimation of the associations.27 Similarly
there are no factors leading to missing data which to activity of atopic eczema, misclassification of
would independently affect the cardiovascular condition severity is possible, for example if patients
outcomes in question, therefore using a complete with severe conditions used only topical treatment.
case analysis was valid. Findings for cardiovascular However, such misclassification would bias our result
death were counterintuitive, as low atopic eczema towards the null, underestimating the magnitude of
activity seemed protective against mortality relative the associations.
to no atopic eczema. This finding may be explained By contrast, bias owing to onset confounding
by the poor capture of data on activity: some patients (differential time since atopic eczema onset) may bias
may have active atopic eczema but do not adhere to away from the null if the risk of cardiovascular disease
treatment, thus being misclassified as never active. increases with time since atopic eczema onset and
As this association was largely attenuated when the most patients with atopic eczema are prevalent cases
analysis was restricted to patients with at least five who may have a greater risk of cardiovascular disease.
years of follow-up, another possible explanation could Consistency in results when restricting to incident atopic
be survival bias, but this needs to be confirmed in other eczema diagnoses suggests that this is not a major issue.
8 doi: 10.1136/bmj.k1786 | BMJ 2018;361:k1786 | the bmj
RESEARCH
Conclusions 7 Silverberg JI, Simpson EL. Associations of childhood eczema
severity: a US population-based study. Dermatitis 2014;25:107-14.
We have shown a clinically relevant increase in the doi:10.1097/DER.0000000000000034
risk of acute cardiovascular outcomes in patients 8 Silverberg JI, Vakharia PP, Chopra R, et al. Phenotypical Differences
of Childhood- and Adult-Onset Atopic Dermatitis. J Allergy Clin
with atopic eczema. This increased risk is largely
Immunol Pract 2017;S2213-2198(17)30757-2. doi:10.1016/j.
confined to patients with severe or more active atopic jaip.2017.10.005
eczema and persists despite adjusting for potential 9 Kim MJ, Kang TW, Cho EA, et al. Prevalence of atopic dermatitis
among Korean adults visiting health service center of the Catholic
mediators, including conventional risk factors for Medical Center in Seoul Metropolitan Area, Korea. J Korean Med
cardiovascular outcomes. Consideration should be Sci 2010;25:1828-30. doi:10.3346/jkms.2010.25.12.1828
10 Herrett E, Gallagher A, Bhaskaran K, et al. Completeness of Key
given to developing prevention strategies to reduce
Variables in the Clinical Practice Research Datalink (CPRD).
the risk of cardiovascular disease among patients Pharmacoepidemiol Drug Saf 2015;24:586-7. https://doi.
with severe or predominantly active atopic eczema, org/10.1002/pds.3838
11 Herrett E, Gallagher AM, Bhaskaran K, et al. Data Resource
including awareness of and screening for conventional Profile: Clinical Practice Research Datalink (CPRD). Int J
cardiovascular risk factors by those providing clinical Epidemiol 2015;44:827-36. doi:10.1093/ije/dyv098
12 Abuabara K, Magyari AM, Hoffstad O, et al. Development and
care. Current biological treatments for atopic eczema
validation of an algorithm to accurately identify atopic eczema
have the potential to greatly change care for those patients in primary care electronic health records from the UK. J Invest
with challenging eczema. The next objective will be to Dermatol 2017;137:1655-62. doi:10.1016/j.jid.2017.03.029
13 Lewis JD, Bilker WB, Weinstein RB, Strom BL. The relationship
reduce the risk of cardiovascular outcomes. between time since registration and measured incidence rates in
the General Practice Research Database. Pharmacoepidemiol Drug
We thank Amanda Roberts, lay member of the Wellcome Senior Saf 2005;14:443-51. doi:10.1002/pds.1115
Clinical Fellowship steering committee, for her input, and Krishnan 14 Gelfand JM, Troxel AB, Lewis JD, et al. The risk of mortality
Bhaskaran, associate professor, Faculty of Epidemiology and in patients with psoriasis: results from a population-based
Population Health, London School of Hygiene & Tropical Medicine, for study. Arch Dermatol 2007;143:1493-9. doi:10.1001/
advising on the analysis of our matched cohort study. archderm.143.12.1493
Contributors: RJS and HJF are joint first authors. RJS, HJF, KA, AA, 15 Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic
MS, SAJS, LS, and SML designed the study, contributed to drafts, and research. Epidemiology 1999;10:37-48. doi:10.1097/00001648-
approved the final manuscript. RJH, HJF, and SML wrote the first draft. 199901000-00008
RJH and HJF carried out the statistical analysis. RJH and HJF are the 16 White IR, Carlin JB. Bias and efficiency of multiple imputation
guarantors. compared with complete-case analysis for missing covariate values.
Stat Med 2010;29:2920-31. doi:10.1002/sim.3944
Funding: This work was supported by a Wellcome senior research 17 Silverberg JI. Public Health Burden and Epidemiology of Atopic
fellowship in clinical science (205039/Z/16/Z). The findings and Dermatitis. Dermatol Clin 2017;35:283-9. doi:10.1016/j.
conclusions in this report are those of the authors and do not det.2017.02.002
necessarily represent the views of the funders. 18 Mathur R, Bhaskaran K, Chaturvedi N, et al. Completeness and
Competing interests: All authors have completed the ICMJE uniform usability of ethnicity data in UK-based primary care and hospital
databases. J Public Health (Oxf) 2014;36:684-92. doi:10.1093/
disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no
pubmed/fdt116
support from any organisation for the submitted work; no financial
19 Tamagawa-Mineoka R, Katoh N, Ueda E, Masuda K, Kishimoto S.
relationships with any organisations that might have an interest in the Elevated platelet activation in patients with atopic dermatitis
submitted work in the previous three years; no other relationships or and psoriasis: increased plasma levels of beta-thromboglobulin
activities that could appear to have influenced the submitted work. and platelet factor 4. Allergol Int 2008;57:391-6. doi:10.2332/
Ethical approval: The study was approved by the Independent allergolint.O-08-537
Scientific Advisory Committee (16_100RA) and the London School of 20 Standl M, Tesch F, Baurecht H, et al. Association of Atopic
Hygiene and Tropical Medicine (11961). Dermatitis with Cardiovascular Risk Factors and Diseases.
J Invest Dermatol 2017;137:1074-81. doi:10.1016/j.
Data sharing: No additional data are available. jid.2016.11.031
Transparency: The manuscripts guarantors (RJH and HJF) affirm that 21 Silverberg JI, Greenland P. Eczema and cardiovascular risk factors in 2
this manuscript is an honest, accurate, and transparent account of US adult population studies. J Allergy Clin Immunol 2015;135:721-8.
the study being reported; that no important aspects of the study have doi:10.1016/j.jaci.2014.11.023
been omitted; and that any discrepancies from the study as planned 22 Silverberg JI. Association between adult atopic dermatitis,
(and, if relevant, registered) have been explained. cardiovascular disease, and increased heart attacks in three
population-based studies. Allergy 2015;70:1300-8. doi:10.1111/
This is an Open Access article distributed in accordance with the all.12685
terms of the Creative Commons Attribution (CC BY 4.0) license, which 23 Herrett E, Shah AD, Boggon R, et al. Completeness and diagnostic
permits others to distribute, remix, adapt and build upon this work, validity of recording acute myocardial infarction events in primary
for commercial use, provided the original work is properly cited. See: care, hospital care, disease registry, and national mortality records:
http://creativecommons.org/licenses/by/4.0/. cohort study. BMJ 2013;346:f2350. doi:10.1136/bmj.f2350
24 Herrett E, Thomas SL, Schoonen WM, Smeeth L, Hall AJ. Validation
1 Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI, and validity of diagnoses in the General Practice Research
ISAAC Phase Three Study Group. Global variations in prevalence of Database: a systematic review. Br J Clin Pharmacol 2010;69:4-14.
eczema symptoms in children from ISAAC Phase Three. J Allergy Clin doi:10.1111/j.1365-2125.2009.03537.x
Immunol 2009;124:1251-8. doi:10.1016/j.jaci.2009.10.009 25 Vandenbroucke J, Pearce N. Point: incident exposures,
2 Weidinger S, Novak N. Atopic dermatitis. Lancet 2016;387:1109-22. prevalent exposures, and causal inference: does limiting studies
doi:10.1016/S0140-6736(15)00149-X to persons who are followed from first exposure onward damage
3 Andersen YM, Egeberg A, Gislason GH, Hansen PR, Skov L, epidemiology? Am J Epidemiol 2015;182:826-33. doi:10.1093/aje/
Thyssen JP. Risk of myocardial infarction, ischemic stroke, and kwv225
cardiovascular death in patients with atopic dermatitis. J Allergy Clin 26 Vandenbroucke J, Pearce N. Vandenbroucke and Pearce respond
Immunol 2016;138:310-12. doi:10.1016/j.jaci.2016.01.015 to “incident and prevalent exposures and causal inference”. Am J
4 Su VY, Chen TJ, Yeh CM, et al. Atopic dermatitis and risk of ischemic Epidemiol 2015;182:846-7. doi:10.1093/aje/kwv219
stroke: a nationwide population-based study. Ann Med 2014;46: 27 Alcabes P, Pezzotti P, Phillips AN, Rezza G, Vlahov D. Long-term
84-9. doi:10.3109/07853890.2013.870018 perspective on the prevalent-cohort biases in studies of human
5 Drucker AM, Li WQ, Cho E, et al. Atopic dermatitis is not independently immunodeficiency virus progression. Am J Epidemiol 1997;146:
associated with nonfatal myocardial infarction or stroke among US 543-51. doi:10.1093/oxfordjournals.aje.a009312
women. Allergy 2016;71:1496-500. doi:10.1111/all.12957
6 Emerson RM, Williams HC, Allen BR. Severity distribution of atopic
dermatitis in the community and its relationship to secondary Supplementary information: Methods S1, tables S1-
referral. Br J Dermatol 1998;139:73-6. doi:10.1046/j.1365-
2133.1998.02316.x S15, and figure S1
No commercial reuse: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
You might also like
- Oaks - The Powers of The Priesthood - by President Dallin H. OaksDocument2 pagesOaks - The Powers of The Priesthood - by President Dallin H. OaksanonNo ratings yet
- Legal Analysis of Utah Medical Marijuana InitiativeDocument7 pagesLegal Analysis of Utah Medical Marijuana InitiativeRobert GehrkeNo ratings yet
- Instruction Booklet For New Providers 2018Document35 pagesInstruction Booklet For New Providers 2018anonNo ratings yet
- 8c99f2 PDFDocument52 pages8c99f2 PDFKrisParadajsNo ratings yet
- Timing Booklet enDocument12 pagesTiming Booklet enanonNo ratings yet
- 2018 Candidate Information Booklet Pain MedicineDocument21 pages2018 Candidate Information Booklet Pain Medicineanon100% (1)
- CT Ordering Guide: Tumor Staging and Follow UpDocument2 pagesCT Ordering Guide: Tumor Staging and Follow UpanonNo ratings yet
- Edwards Critical Care Quick Guide To Cardiopulmonary Care PDFDocument188 pagesEdwards Critical Care Quick Guide To Cardiopulmonary Care PDFanonNo ratings yet
- Swan Ganz CatheterDocument40 pagesSwan Ganz CatheterRobertson Sliva100% (3)
- Old Testament Timeline BookmarkDocument2 pagesOld Testament Timeline BookmarkanonNo ratings yet
- New Testament ChronologyDocument2 pagesNew Testament ChronologyanonNo ratings yet
- Book of Mormon Timeline BookmarkDocument2 pagesBook of Mormon Timeline Bookmarkanon100% (4)
- ArrestPac RefSheet AHADocument2 pagesArrestPac RefSheet AHAanonNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Water, Air, Soil Pollution Major Global Health RiskDocument2 pagesWater, Air, Soil Pollution Major Global Health RiskSabina Lucia GrapiniNo ratings yet
- Bacteria Viruses Lesson PlanDocument7 pagesBacteria Viruses Lesson Planapi-665322772No ratings yet
- Template RSB Puskesmas: Dokumen Pra BLUD PuskesmasDocument50 pagesTemplate RSB Puskesmas: Dokumen Pra BLUD PuskesmasSofiaNo ratings yet
- America'S Opioid Ecosystem: How Leveraging System Interactions Can Help Curb Addiction, Overdose, and Other HarmsDocument618 pagesAmerica'S Opioid Ecosystem: How Leveraging System Interactions Can Help Curb Addiction, Overdose, and Other HarmsMayankNo ratings yet
- AJ PACKAGING LIMIT-35113 - MIS - Claim - Details - Till-13 - 09 - 21Document27 pagesAJ PACKAGING LIMIT-35113 - MIS - Claim - Details - Till-13 - 09 - 21Yanamandra Radha Phani ShankarNo ratings yet
- Digital Rectal ExaminationDocument7 pagesDigital Rectal ExaminationAla'a Emerald AguamNo ratings yet
- Government of NCT of Delhi Delhi Subordinate Services Selection Board Fc-18, Institutional Area, Karkardooma, DelhiDocument3 pagesGovernment of NCT of Delhi Delhi Subordinate Services Selection Board Fc-18, Institutional Area, Karkardooma, DelhiVivekRawalNo ratings yet
- DSM-5's Quick Guide to Feeding and Eating DisordersDocument17 pagesDSM-5's Quick Guide to Feeding and Eating DisordersHana alassafNo ratings yet
- Pain and Symptom Management in Palliative Care and at End ofDocument11 pagesPain and Symptom Management in Palliative Care and at End ofelbaNo ratings yet
- Why Can'T We Just Drink The Water From Natural Sources?: Myths About Contaminated WaterDocument2 pagesWhy Can'T We Just Drink The Water From Natural Sources?: Myths About Contaminated WaterAiron Kaye SameloNo ratings yet
- Well Fact Sheet: Suitability of Water For Livestock Fact SheetDocument2 pagesWell Fact Sheet: Suitability of Water For Livestock Fact SheetHill County Conservation DistrictNo ratings yet
- Pregabalin vs Pramipexole for RLS AugmentationDocument49 pagesPregabalin vs Pramipexole for RLS AugmentationFrans JobethNo ratings yet
- Laryngeal Cancer: Anh Q. Truong MS-4 University of Washington, SOMDocument33 pagesLaryngeal Cancer: Anh Q. Truong MS-4 University of Washington, SOMSri Agustina0% (1)
- Guideline For The Diagnosis, Treatment and Long-Term Management of Cutaneous Lupus ErythematosusDocument16 pagesGuideline For The Diagnosis, Treatment and Long-Term Management of Cutaneous Lupus ErythematosusMariana de la VegaNo ratings yet
- Assessing Children's Pain: R-Flacc Pain Rating Scale For Children With Developmental DisabilityDocument1 pageAssessing Children's Pain: R-Flacc Pain Rating Scale For Children With Developmental DisabilityifanNo ratings yet
- The Importance of Using ContraceptivesDocument14 pagesThe Importance of Using ContraceptivesYsabelle De GuzmanNo ratings yet
- Example PT1 Backwards Planning - DeinstitutionalizationDocument8 pagesExample PT1 Backwards Planning - Deinstitutionalization213 212No ratings yet
- English 8-Q4-M7 PDFDocument14 pagesEnglish 8-Q4-M7 PDFLorry ManuelNo ratings yet
- Reimplantation of Avulsed Tooth - A Case StudyDocument3 pagesReimplantation of Avulsed Tooth - A Case Studyrahul sharmaNo ratings yet
- The Paper Test Includes 4 Pages Time Allowance: 40 Minutes Date: 06 June, 2021Document4 pagesThe Paper Test Includes 4 Pages Time Allowance: 40 Minutes Date: 06 June, 2021Truơng Anh TàiNo ratings yet
- Medicine CASES - CVS 2Document22 pagesMedicine CASES - CVS 2malaz adilNo ratings yet
- Lukeka Shabani Papy-CVDocument3 pagesLukeka Shabani Papy-CVAnonymous o32OUFNo ratings yet
- Pneumonia AnswersDocument5 pagesPneumonia AnswersColeen Mae CamaristaNo ratings yet
- Journal FoodDocument4 pagesJournal FoodMizaZainalNo ratings yet
- Nursing Case Analysis 4Document3 pagesNursing Case Analysis 4Luna GrayNo ratings yet
- DepED PFT Score CardDocument1 pageDepED PFT Score CardFelix Llamera80% (30)
- Stunting Kamas Kirim, DR. Dr. Titis Prawitasari, Sp.A (K), 160622Document51 pagesStunting Kamas Kirim, DR. Dr. Titis Prawitasari, Sp.A (K), 160622Theodora NancyNo ratings yet
- LastCallProgram ScienceDocument16 pagesLastCallProgram ScienceConiforNo ratings yet
- Managing Rheumatic and Musculoskeletal Diseases - Past, Present and FutureDocument6 pagesManaging Rheumatic and Musculoskeletal Diseases - Past, Present and FutureNICOLASNo ratings yet
- Is An Intensive Outpatient ProgramDocument1 pageIs An Intensive Outpatient ProgramJack williamNo ratings yet