You might also like
- Caries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFDocument7 pagesCaries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFGen LCNo ratings yet
- The Incipient Caries: January 2013Document6 pagesThe Incipient Caries: January 2013Ramya ReddyNo ratings yet
- Current Status of Conservative Treatment of Deep Car Ious LesionsDocument5 pagesCurrent Status of Conservative Treatment of Deep Car Ious LesionsHamad KayaniNo ratings yet
- International Caries Detection and Assessment System (ICDAS) PDFDocument4 pagesInternational Caries Detection and Assessment System (ICDAS) PDFKelvin Jaya AlamNo ratings yet
- Caries Detection and Diagnosis Novel TechnologiesDocument13 pagesCaries Detection and Diagnosis Novel TechnologiesIustina-Maria VladescuNo ratings yet
- Gug Nani 2011Document8 pagesGug Nani 2011danielstevenNo ratings yet
- G Restorative PDFDocument12 pagesG Restorative PDFerma gusmayantiNo ratings yet
- 1.dental CariesDocument12 pages1.dental CariesMatt NooriNo ratings yet
- HIGHLIGHTER Article #10Document13 pagesHIGHLIGHTER Article #10neeNo ratings yet
- Caries Process and Prevention Strategies DiagnosisDocument9 pagesCaries Process and Prevention Strategies Diagnosisnoelah salcedoNo ratings yet
- 16 Access Related Endodontic Mishaps.20170115064301Document8 pages16 Access Related Endodontic Mishaps.20170115064301Amrutha DasariNo ratings yet
- Tecnica de HallDocument4 pagesTecnica de HallYalile TurkaNo ratings yet
- Pubic AssignmentDocument11 pagesPubic AssignmentAbdulRahman M. AbdulJlilNo ratings yet
- Restoring Proximal Caries Lesions Conservatively With Tunnel RestorationsDocument8 pagesRestoring Proximal Caries Lesions Conservatively With Tunnel RestorationsyesikaichaaNo ratings yet
- Minimally Invasive Caries Management ProtocolDocument8 pagesMinimally Invasive Caries Management ProtocolKarReséndizNo ratings yet
- 2014 Sheets 2Document9 pages2014 Sheets 2Cathleen LiNo ratings yet
- Dental Caries CaseDocument5 pagesDental Caries CaseEerrmmaa Ssaarrell Rroommaann PpaarraaNo ratings yet
- Metode de DiagnosticDocument10 pagesMetode de DiagnosticDorina IonescuNo ratings yet
- BP Restorativedent PDFDocument13 pagesBP Restorativedent PDFFrancisca AndreaNo ratings yet
- Diag 1 Current and Future Research in Diagnostic Criteria and Evaluation of Caries Detection MethodsDocument10 pagesDiag 1 Current and Future Research in Diagnostic Criteria and Evaluation of Caries Detection MethodsAbdulmajeed alluqmaniNo ratings yet
- Pediatric Restorative DentistryDocument13 pagesPediatric Restorative DentistryJamaludin Nawawi100% (1)
- CariesDocument9 pagesCariesKhotimatul BarkiNo ratings yet
- Guideline On Restorative Dentist: Originating CommitteeDocument13 pagesGuideline On Restorative Dentist: Originating CommitteeAnaMaríaRGNo ratings yet
- Conservative Treatment of Deep Carious LesionsDocument4 pagesConservative Treatment of Deep Carious LesionsMarïsa CastellonNo ratings yet
- Minimal Invasive DentistryDocument9 pagesMinimal Invasive DentistryLamia HusseinNo ratings yet
- New Caries Diagnostic MethodsDocument9 pagesNew Caries Diagnostic MethodsKarma YogaNo ratings yet
- Evans Article Caries in AdultDocument10 pagesEvans Article Caries in AdultInVision Dental-Models100% (2)
- Diagnostic Aids in Pediatric Dentistry: Ijcpd Review ArticleDocument7 pagesDiagnostic Aids in Pediatric Dentistry: Ijcpd Review Articlechaithra shree s raoNo ratings yet
- Minimal Intervention Dentistry: Part 4. Detection and Diagnosis of Initial Caries LesionsDocument7 pagesMinimal Intervention Dentistry: Part 4. Detection and Diagnosis of Initial Caries LesionsAdriana Paola Vega YanesNo ratings yet
- Evans Et Al-2008-Australian Dental Journal PDFDocument10 pagesEvans Et Al-2008-Australian Dental Journal PDFtea metaNo ratings yet
- Journal DenradDocument6 pagesJournal DenradFelianda ThaliaNo ratings yet
- Clinical Evaluation of Caries Removal Efficacy of Polymer Burs Running Title Efficacy of Polymer BursDocument8 pagesClinical Evaluation of Caries Removal Efficacy of Polymer Burs Running Title Efficacy of Polymer BursInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Lambrianidis Ledging EndodontictopicsDocument20 pagesLambrianidis Ledging EndodontictopicsAyu Diah LestariNo ratings yet
- Van Thompson 2008 Treatment of Deep Carious Lesions by CompleteDocument8 pagesVan Thompson 2008 Treatment of Deep Carious Lesions by CompleteAli Al-QaysiNo ratings yet
- Apexification-Then and NowDocument4 pagesApexification-Then and NowLaura RuZeNo ratings yet
- CviDocument12 pagesCviMarwane BenzianeNo ratings yet
- Qi 23 5 Ripa 2Document9 pagesQi 23 5 Ripa 2Ifi Nursari RosantiNo ratings yet
- Chapter 2 DiagnosisDocument24 pagesChapter 2 DiagnosisnilafebryNo ratings yet
- Afraccion PDFDocument9 pagesAfraccion PDFzayraNo ratings yet
- Caries Classification: CUNY Academic WorksDocument4 pagesCaries Classification: CUNY Academic Worksragu nathanNo ratings yet
- SJ BDJ 2012 615Document8 pagesSJ BDJ 2012 615alfredoibcNo ratings yet
- Ekstrand2001 ARTICULO SEMINADocument7 pagesEkstrand2001 ARTICULO SEMINACarolina Rodríguez RamírezNo ratings yet
- Accurate Detection of Non-Cavitated Proximal Caries in Posterior Permanent Teeth: An in Vivo StudyDocument6 pagesAccurate Detection of Non-Cavitated Proximal Caries in Posterior Permanent Teeth: An in Vivo StudyPutu WidiastriNo ratings yet
- Odontología Restaurativa NiñosDocument13 pagesOdontología Restaurativa NiñosAndrea Mackarena Inostroza ÓrdenesNo ratings yet
- Incomplete Caries Remova Asystematic Review and Meta AnalysisDocument10 pagesIncomplete Caries Remova Asystematic Review and Meta AnalysisSadeer RiyadNo ratings yet
- I0003-3219-89!3!359 White Spot Lesion AlignerDocument6 pagesI0003-3219-89!3!359 White Spot Lesion AlignerLima JúniorNo ratings yet
- Banarjee 2020-2 PDFDocument9 pagesBanarjee 2020-2 PDFMaximiliano Jara ContrerasNo ratings yet
- 0121 246X Rfoua 28 02 00341Document13 pages0121 246X Rfoua 28 02 00341Kevinn YupaNo ratings yet
- Jurnal BitewingDocument6 pagesJurnal BitewingWidi PrabowoNo ratings yet
- Commentary Guest Editoriatl P 12-16.ashxDocument3 pagesCommentary Guest Editoriatl P 12-16.ashxjharmandoNo ratings yet
- ArticuloDocument10 pagesArticuloMaría Fernanda MontealegreNo ratings yet
- Radiographic Decision Making-Outline.Document7 pagesRadiographic Decision Making-Outline.Rachael MutheuNo ratings yet
- Palatally Impacted CaninesDocument5 pagesPalatally Impacted CaninesMoisés MartinsNo ratings yet
- 1977 Indexing Occlusions For DentalDocument7 pages1977 Indexing Occlusions For Dentalplayer osamaNo ratings yet
- Makale4 PDFDocument6 pagesMakale4 PDFPatricio MendezNo ratings yet
- Does Operatory Field Isolation Influence The Performance of Direct Adhesive RestorationsDocument6 pagesDoes Operatory Field Isolation Influence The Performance of Direct Adhesive Restorationsdr.gonzalezcalvinoNo ratings yet
- Pre Bleaching ExamDocument2 pagesPre Bleaching ExamFeryn Adma WijayaNo ratings yet
- Laser Management of ScarsFrom EverandLaser Management of ScarsKayvan ShokrollahiNo ratings yet
- Negotiation Training - The Top 4 No-Oriented' QuestionsDocument3 pagesNegotiation Training - The Top 4 No-Oriented' Questionsjimmyboy111No ratings yet
- 8 Lessons in Military Leadership by Robert Kiyosaki, Author of Rich Dad, Poor Dad - NancyrubinDocument4 pages8 Lessons in Military Leadership by Robert Kiyosaki, Author of Rich Dad, Poor Dad - Nancyrubinjimmyboy111No ratings yet
- How To Fix A Sticky Trip-Lever Bathtub Drain StopperDocument6 pagesHow To Fix A Sticky Trip-Lever Bathtub Drain Stopperjimmyboy111100% (1)
- Understanding The Federal Reserve Balance SheetDocument4 pagesUnderstanding The Federal Reserve Balance Sheetjimmyboy111No ratings yet
- Texas Property Tax Exemptions 96-1740Document24 pagesTexas Property Tax Exemptions 96-1740jimmyboy111No ratings yet
- Myth-Busting - Equities Are An Inflation Hedge - CFA Institute Enterprising InvestorDocument5 pagesMyth-Busting - Equities Are An Inflation Hedge - CFA Institute Enterprising Investorjimmyboy111No ratings yet
- PROFLO PF1030GCP Tub and Shower Trim PackageDocument3 pagesPROFLO PF1030GCP Tub and Shower Trim Packagejimmyboy111No ratings yet
- Sanken Backlight LED Driver bl0202b TCL Roku - Ds - enDocument26 pagesSanken Backlight LED Driver bl0202b TCL Roku - Ds - enjimmyboy111100% (1)
- Simmerstats and Infinite Switches For OvensDocument25 pagesSimmerstats and Infinite Switches For Ovensjimmyboy111No ratings yet
- Annual S&P Sector PerformanceDocument3 pagesAnnual S&P Sector Performancejimmyboy111No ratings yet
- Portable Bandsaw Variable Speed: Assembly and Operating InstructionsDocument11 pagesPortable Bandsaw Variable Speed: Assembly and Operating Instructionsjimmyboy111No ratings yet
- Environment International: Lidia Morawska, Junji Cao TDocument3 pagesEnvironment International: Lidia Morawska, Junji Cao TGreysia ManarisipNo ratings yet
- Education As Heresy in The Middle Ages - Catholicism Church History - Ask MetaFilterDocument18 pagesEducation As Heresy in The Middle Ages - Catholicism Church History - Ask MetaFilterjimmyboy111No ratings yet
- 30 Phrases & Words To Flirt in FrenchDocument16 pages30 Phrases & Words To Flirt in Frenchjimmyboy111No ratings yet
- Getting Windbg Without The Whole WDK - Stack OverflowDocument7 pagesGetting Windbg Without The Whole WDK - Stack Overflowjimmyboy111No ratings yet
- Switch-Mode Power Converter Compensation Made Easy: Robert SheehanDocument38 pagesSwitch-Mode Power Converter Compensation Made Easy: Robert Sheehanjimmyboy111No ratings yet
- Simmerstat SwitchesDocument41 pagesSimmerstat Switchesjimmyboy111No ratings yet
- S101 M101 Precision AC Undervoltage Monitoring Chip IN1M101Document5 pagesS101 M101 Precision AC Undervoltage Monitoring Chip IN1M101jimmyboy111No ratings yet
- 77 Romantic French Words and Phrases To Melt Your Lover's HeartDocument17 pages77 Romantic French Words and Phrases To Melt Your Lover's Heartjimmyboy111No ratings yet
- UTILIZING ORANGE PEELS FOR ESSENTIAL OIL PRODUCTION Jeas - 0118 - 6632Document12 pagesUTILIZING ORANGE PEELS FOR ESSENTIAL OIL PRODUCTION Jeas - 0118 - 6632jimmyboy111No ratings yet
- Modern Extraction of Citrus Wastes - Foods-08-00523-V2 PDFDocument81 pagesModern Extraction of Citrus Wastes - Foods-08-00523-V2 PDFjimmyboy111No ratings yet
- SARS-Cov-2 RNA Found On Particulate Matter of Bergamo 2020.04.15.20065995v2.fullDocument7 pagesSARS-Cov-2 RNA Found On Particulate Matter of Bergamo 2020.04.15.20065995v2.fulljimmyboy111No ratings yet
- Toneohm 850 Operation Manual PDFDocument60 pagesToneohm 850 Operation Manual PDFjimmyboy111No ratings yet
- Extraction Methods of Citrus Peel Phenolic Compounds 10.1080@87559129.2014.924139Document59 pagesExtraction Methods of Citrus Peel Phenolic Compounds 10.1080@87559129.2014.924139jimmyboy111No ratings yet
- Hitachi Router M12VC - BD - 9292 PDFDocument4 pagesHitachi Router M12VC - BD - 9292 PDFjimmyboy111No ratings yet
- R3 Stuck Router Bits PDFDocument3 pagesR3 Stuck Router Bits PDFjimmyboy111No ratings yet
- Hitachi 2SB77 DatasheetDocument1 pageHitachi 2SB77 Datasheetjimmyboy111No ratings yet
- TDS ColorDocument1 pageTDS Colorjimmyboy111No ratings yet
- Snubber Circuits For Power Electronics - Severns PDFDocument346 pagesSnubber Circuits For Power Electronics - Severns PDFjimmyboy111No ratings yet
- Polar - Toneohm - 850a - Service - Manual - No Schematic PDFDocument36 pagesPolar - Toneohm - 850a - Service - Manual - No Schematic PDFjimmyboy111No ratings yet
- TM-8000 HD Manual PDFDocument37 pagesTM-8000 HD Manual PDFRoxana BirtumNo ratings yet
- Astm C892 - 00Document5 pagesAstm C892 - 00reneeNo ratings yet
- Crouse Hinds XPL Led BrochureDocument12 pagesCrouse Hinds XPL Led BrochureBrayan Galaz BelmarNo ratings yet
- Harmonics PatternsDocument4 pagesHarmonics PatternsIzzadAfif1990No ratings yet
- CheckList For Checking of Drawings-R1Document4 pagesCheckList For Checking of Drawings-R1jatin kalraNo ratings yet
- Nivel VV-VW Board User Guide enDocument5 pagesNivel VV-VW Board User Guide enHarveyWishtartNo ratings yet
- Impact of Retrofitting Existing Combined Heat and Power Plant With Polygeneration of Biomethane PDFDocument16 pagesImpact of Retrofitting Existing Combined Heat and Power Plant With Polygeneration of Biomethane PDFAwais Salman0% (1)
- Cisco 2500 Series RoutersDocument16 pagesCisco 2500 Series RoutersJull Quintero DazaNo ratings yet
- Save Water SpeechDocument4 pagesSave Water SpeechHari Prakash Shukla0% (1)
- 3 Tasks and ANS - Gamma Maths PDFDocument6 pages3 Tasks and ANS - Gamma Maths PDFNora ZhangNo ratings yet
- Shree New Price List 2016-17Document13 pagesShree New Price List 2016-17ontimeNo ratings yet
- Shawal 1431 AH Prayer ScheduleDocument2 pagesShawal 1431 AH Prayer SchedulemasjidibrahimNo ratings yet
- Provision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field DevelopmentDocument7 pagesProvision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field Developmentriandi100% (1)
- Stepan Formulation 926Document2 pagesStepan Formulation 926Moaz SiddigNo ratings yet
- Goldhofer FTV 850 BrochureDocument2 pagesGoldhofer FTV 850 BrochureMauroNo ratings yet
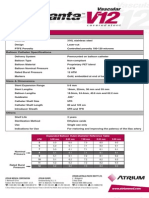
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiNo ratings yet
- Gemh 108Document20 pagesGemh 108YuvrajNo ratings yet
- Schneider Pressure Switch XMLDocument2 pagesSchneider Pressure Switch XMLhaoNo ratings yet
- User'S Guide: Tm4C Series Tm4C129E Crypto Connected Launchpad Evaluation KitDocument36 pagesUser'S Guide: Tm4C Series Tm4C129E Crypto Connected Launchpad Evaluation KitLương Văn HưởngNo ratings yet
- Hopeless PlacesDocument1,304 pagesHopeless Placesmoreblessingmarvellous659No ratings yet
- 14p-220 Mud PumpDocument2 pages14p-220 Mud PumpMurali Sambandan50% (2)
- Esteem 1999 2000 1.3L 1.6LDocument45 pagesEsteem 1999 2000 1.3L 1.6LArnold Hernández CarvajalNo ratings yet
- Biomedical Engineering Handbook Revised 5 2015Document37 pagesBiomedical Engineering Handbook Revised 5 2015Teja GuttiNo ratings yet
- Midterm Exam Gor Grade 11Document2 pagesMidterm Exam Gor Grade 11Algelle AbrantesNo ratings yet
- 300 PSI CTS (MP-1115) Operation Manual Rev1.3Document18 pages300 PSI CTS (MP-1115) Operation Manual Rev1.3Juan Manuel VizosoNo ratings yet
- Release From Destructive Covenants - D. K. OlukoyaDocument178 pagesRelease From Destructive Covenants - D. K. OlukoyaJemima Manzo100% (1)
- Fines Reduction Project at Wendling Bowser QuarryDocument2 pagesFines Reduction Project at Wendling Bowser QuarryMarcos Antonio ParoliniNo ratings yet
- Worlds Apart: A Story of Three Possible Warmer WorldsDocument1 pageWorlds Apart: A Story of Three Possible Warmer WorldsJuan Jose SossaNo ratings yet
- Native Data Sheet Asme b73.1Document4 pagesNative Data Sheet Asme b73.1Akhmad Faruq Alhikami100% (1)
- World's Standard Model G6A!: Low Signal RelayDocument9 pagesWorld's Standard Model G6A!: Low Signal RelayEgiNo ratings yet