You might also like
- Friedrich 2007Document10 pagesFriedrich 2007yenrilisnaNo ratings yet
- 2 Ref 7Document10 pages2 Ref 7arjun muchhadiyaNo ratings yet
- Does Experimental Low Back Pain Change PDocument8 pagesDoes Experimental Low Back Pain Change PJuancepaNo ratings yet
- Acrofobia 5Document4 pagesAcrofobia 5Teinei :vNo ratings yet
- Jurnal DizzinessDocument7 pagesJurnal DizzinessFila DelviaNo ratings yet
- Lecture Scap Malaga 2Document47 pagesLecture Scap Malaga 2danielaNo ratings yet
- EFFECTS OF MOBILIZATION WITH MOVEMENT ON Shoulder PainDocument8 pagesEFFECTS OF MOBILIZATION WITH MOVEMENT ON Shoulder PainDimasPrasetyoNo ratings yet
- Kalichman Ratmansky 2011-Hemiplegic Shoulder Pain PDFDocument13 pagesKalichman Ratmansky 2011-Hemiplegic Shoulder Pain PDFYandry MoreiraNo ratings yet
- Massó-Ortigosa Et al.-H-Reflex-DS-2019Document18 pagesMassó-Ortigosa Et al.-H-Reflex-DS-2019Robi SiliNo ratings yet
- Online Provisional: Postural Balance in Patients With Social Anxiety DisorderDocument7 pagesOnline Provisional: Postural Balance in Patients With Social Anxiety DisorderBombong ENNo ratings yet
- Biofeedback For Vertigo 2ndry To Cervical LesionDocument7 pagesBiofeedback For Vertigo 2ndry To Cervical LesionBassam EsmailNo ratings yet
- Manual Therapy: Ney Meziat Filho, Sonia Santos, Ricardo Mourilhe RochaDocument4 pagesManual Therapy: Ney Meziat Filho, Sonia Santos, Ricardo Mourilhe RochaVladislav KotovNo ratings yet
- 2018 Hippotherapy On Postural Balance in The Sitting Position of Children With Cerebral Palsy Longitudinal StudyDocument9 pages2018 Hippotherapy On Postural Balance in The Sitting Position of Children With Cerebral Palsy Longitudinal StudyMarta SommerNo ratings yet
- Dix HallPike TestDocument2 pagesDix HallPike TestnvalenzuelanNo ratings yet
- Characteristics of Cervical Position Sense in Subjects With Forward Head PostureDocument3 pagesCharacteristics of Cervical Position Sense in Subjects With Forward Head PostureA AZIZNo ratings yet
- Cheung2020 PDFDocument15 pagesCheung2020 PDFSandra Milena Cortes SotoNo ratings yet
- The Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyDocument8 pagesThe Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyAlexandra-Andreea BroascăNo ratings yet
- JANSSENS L IMTaffectsPropriocepticeUseAndLowBackPainDocument8 pagesJANSSENS L IMTaffectsPropriocepticeUseAndLowBackPainDaniel A Llanes MolinaNo ratings yet
- Kristenen, NeckmusclebalanceDocument9 pagesKristenen, NeckmusclebalancePhooi Yee LauNo ratings yet
- SSRN Id4093327Document24 pagesSSRN Id4093327Muhammad AbdullahNo ratings yet
- Sleep PaternDocument7 pagesSleep PaternidaNo ratings yet
- Reduced Cortical Folding in PPPDDocument12 pagesReduced Cortical Folding in PPPDDanielNo ratings yet
- Paper Positional Release Technique SF MWDocument17 pagesPaper Positional Release Technique SF MWkamNo ratings yet
- 2015 - Chronic Neck Pain Alters Muscle Activation Patterns To Sudden Movements (D. Falla)Document11 pages2015 - Chronic Neck Pain Alters Muscle Activation Patterns To Sudden Movements (D. Falla)romiromiromi123No ratings yet
- The Role of Muscle Strength & Activation Patterns in Patellofemoral PainDocument5 pagesThe Role of Muscle Strength & Activation Patterns in Patellofemoral Paincristian fabian perez romeroNo ratings yet
- Vestibular and Proprioceptive Contributions To Human Balance CorrectionsDocument12 pagesVestibular and Proprioceptive Contributions To Human Balance CorrectionsGinaDyoSalsabilaNo ratings yet
- 10 1016@j Ultrasmedbio 2020 02 004Document15 pages10 1016@j Ultrasmedbio 2020 02 004Humberto Salas VelizNo ratings yet
- 6 Ref 12Document9 pages6 Ref 12arjun muchhadiyaNo ratings yet
- Journal of Behavior Therapy and Experimental PsychiatryDocument8 pagesJournal of Behavior Therapy and Experimental PsychiatryAndré LuizNo ratings yet
- Wernli K. OSullivan P. Smith A. Campbell A. Kent O. 2020. Movement Posture and Low Back Pain. How Do They RelateDocument19 pagesWernli K. OSullivan P. Smith A. Campbell A. Kent O. 2020. Movement Posture and Low Back Pain. How Do They RelateVizaNo ratings yet
- Adhesive Capsulitis Presentation May 2009Document29 pagesAdhesive Capsulitis Presentation May 2009cm4100% (1)
- Postural Awareness and Its Relation To Pain ValidaDocument11 pagesPostural Awareness and Its Relation To Pain ValidacderosasNo ratings yet
- Jurnal Remato 2Document8 pagesJurnal Remato 2aandakuNo ratings yet
- Shoulder Impingement SyndromeDocument6 pagesShoulder Impingement SyndromeluizamgoNo ratings yet
- JurnalDocument8 pagesJurnalAlifia RizqiNo ratings yet
- Journal of Bodywork & Movement Therapies: A Systematic Review and Meta-AnalysisDocument11 pagesJournal of Bodywork & Movement Therapies: A Systematic Review and Meta-AnalysiswellytonNo ratings yet
- Glaa 014Document11 pagesGlaa 014wellingtaniad3426No ratings yet
- 1413 3555 Rbfis BJPT rbf20140158Document8 pages1413 3555 Rbfis BJPT rbf20140158Hector MiguelNo ratings yet
- Peterka - 2002 - J NeurophysDocument23 pagesPeterka - 2002 - J NeurophysKarem TuctoNo ratings yet
- 33 malchow2016Document10 pages33 malchow2016Sergio Machado NeurocientistaNo ratings yet
- Manual Therapy: Eva Barrett, Mary O'Keeffe, Kieran O'Sullivan, Jeremy Lewis, Karen MccreeshDocument9 pagesManual Therapy: Eva Barrett, Mary O'Keeffe, Kieran O'Sullivan, Jeremy Lewis, Karen MccreeshPrincess Dianna SulitNo ratings yet
- 2018 Article 2031Document10 pages2018 Article 2031marcelonorisNo ratings yet
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDocument14 pagesAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanNo ratings yet
- Journal RombergDocument7 pagesJournal RombergAnonymousssNo ratings yet
- Molina 2019Document10 pagesMolina 2019camila hernandezNo ratings yet
- Furman - 2007 Vestibo Ocular Function in Anxiety DisordersDocument8 pagesFurman - 2007 Vestibo Ocular Function in Anxiety DisordersJuan Hernández GarcíaNo ratings yet
- La Correlation Ntre La Mastication Unilateral Et Les Postures DevieesDocument8 pagesLa Correlation Ntre La Mastication Unilateral Et Les Postures DevieesbentatanihalNo ratings yet
- Impact of Osteopathic Therapy On Pro-Prioceptive Balance and Quality of Life in Patients With DizzinessDocument6 pagesImpact of Osteopathic Therapy On Pro-Prioceptive Balance and Quality of Life in Patients With DizzinessTria Mega HoliviaNo ratings yet
- Introduction: Convergence and Divergence of Opinions On Spinal ControlDocument4 pagesIntroduction: Convergence and Divergence of Opinions On Spinal ControlNaveen ChoudharyNo ratings yet
- Effect of Thoracic Spinal Manipulation On Lower Limb Neurodynamics in Healthy Young Adults: Neural Link To Regional InterdependenceDocument10 pagesEffect of Thoracic Spinal Manipulation On Lower Limb Neurodynamics in Healthy Young Adults: Neural Link To Regional InterdependencekotzaNo ratings yet
- 1 s2.0 S0165587622001008 MainDocument5 pages1 s2.0 S0165587622001008 MaintesteiroNo ratings yet
- The Role of Fear of Movement/ (Re) Injury in Pain DisabilityDocument18 pagesThe Role of Fear of Movement/ (Re) Injury in Pain DisabilityWilbur WhateleyNo ratings yet
- Effects of Thoracic Mobilization and Manipulation On Function and Mental State in Chronic Lower Back PainDocument4 pagesEffects of Thoracic Mobilization and Manipulation On Function and Mental State in Chronic Lower Back PainRatna Sulistya DewiNo ratings yet
- Lumbar Kinematic Variability During Gait in Chronic Low Back Pain and Associations With Pain, Disability and Isolated Lumbar Extension StrengthDocument8 pagesLumbar Kinematic Variability During Gait in Chronic Low Back Pain and Associations With Pain, Disability and Isolated Lumbar Extension StrengthebiNo ratings yet
- Research ArticleDocument12 pagesResearch ArticleIntan Maisaroh TYNo ratings yet
- Neuropsychologia: Nancy Byl, Wenlong Zhang, Sophia Coo, Masayoshi TomizukaDocument12 pagesNeuropsychologia: Nancy Byl, Wenlong Zhang, Sophia Coo, Masayoshi TomizukaMariachiaraRicciNo ratings yet
- Lumbar Spondylitis and Massage TherapyDocument9 pagesLumbar Spondylitis and Massage Therapyavonk515No ratings yet
- Altered Lumbopelvic Movement Control But Not Generalized Joint HypermobilityDocument6 pagesAltered Lumbopelvic Movement Control But Not Generalized Joint HypermobilityMário OrnelasNo ratings yet
- Fix 3 03000605221103543Document10 pagesFix 3 03000605221103543Teuku FadhliNo ratings yet
- Cell Biology Assays: Essential MethodsFrom EverandCell Biology Assays: Essential MethodsFanny JaulinNo ratings yet
- Anti-In Ammatory Effects of A Vegan Diet Versus The American Heart Association - Recommended Diet in Coronary Artery Disease TrialDocument14 pagesAnti-In Ammatory Effects of A Vegan Diet Versus The American Heart Association - Recommended Diet in Coronary Artery Disease TrialAnonymous b2k9ABe7eNo ratings yet
- Klooster ManDocument12 pagesKlooster ManAnonymous b2k9ABe7eNo ratings yet
- EU04 2016 Special DGE Eng FinalDocument11 pagesEU04 2016 Special DGE Eng FinalAnonymous b2k9ABe7eNo ratings yet
- Gravitational WaveDocument16 pagesGravitational WaveManodeep MondalNo ratings yet
- Gravity DummiesDocument31 pagesGravity DummiesRicardo CaffeNo ratings yet
- Klooster ManDocument59 pagesKlooster ManAnonymous b2k9ABe7eNo ratings yet
- Klooster ManDocument12 pagesKlooster ManAnonymous b2k9ABe7eNo ratings yet
- Alzofon - Anti-Gravity WTH Present Technology - Implementation and Theoretical Foundation - 1981 PDFDocument34 pagesAlzofon - Anti-Gravity WTH Present Technology - Implementation and Theoretical Foundation - 1981 PDFAnonymous b2k9ABe7eNo ratings yet
- RH25 - MelbournDocument1 pageRH25 - MelbournAnonymous b2k9ABe7eNo ratings yet
- Alzofon - Anti-Gravity WTH Present Technology - Implementation and Theoretical Foundation - 1981Document9 pagesAlzofon - Anti-Gravity WTH Present Technology - Implementation and Theoretical Foundation - 1981Anonymous b2k9ABe7eNo ratings yet
- Sanwellw and Smith 2008Document18 pagesSanwellw and Smith 2008Giulia LicocciaNo ratings yet
- Title: Instructions For UseDocument5 pagesTitle: Instructions For UseAnonymous b2k9ABe7eNo ratings yet
- Alzofon - Anti-Gravity WTH Present Technology - Implementation and Theoretical Foundation - 1981 PDFDocument34 pagesAlzofon - Anti-Gravity WTH Present Technology - Implementation and Theoretical Foundation - 1981 PDFAnonymous b2k9ABe7eNo ratings yet
- Myositis Core Set Measures of Activity Including The Mmt8 and Preliminary Definitions of Improvement 508Document25 pagesMyositis Core Set Measures of Activity Including The Mmt8 and Preliminary Definitions of Improvement 508Anonymous b2k9ABe7eNo ratings yet
- A Constraint On Antigravity of Antimatter From Precision Spectroscopy of Simple AtomsDocument7 pagesA Constraint On Antigravity of Antimatter From Precision Spectroscopy of Simple AtomsAnonymous b2k9ABe7eNo ratings yet
- 29 - Jpts 2017 158Document16 pages29 - Jpts 2017 158Anonymous b2k9ABe7eNo ratings yet
- J Phys Ther Sci - 26 (12) - 1871-1874Document3 pagesJ Phys Ther Sci - 26 (12) - 1871-1874Anonymous b2k9ABe7eNo ratings yet
- Title: Instructions For UseDocument5 pagesTitle: Instructions For UseAnonymous b2k9ABe7eNo ratings yet
- Anti-Gravity Treadmill Can Promote Aerobic ExercisDocument5 pagesAnti-Gravity Treadmill Can Promote Aerobic ExercisAnonymous b2k9ABe7eNo ratings yet
- Combined Flux Compression and Plasma Opening Switch On The Saturn Pulsed Power GeneratorDocument4 pagesCombined Flux Compression and Plasma Opening Switch On The Saturn Pulsed Power GeneratorAnonymous b2k9ABe7eNo ratings yet
- Testing Existence of AntigravityDocument12 pagesTesting Existence of AntigravityFausto IntillaNo ratings yet
- Cardiovascular Responses To Antigravity Muscle Loading During Head-Down Tilt at Rest and After Dynamic ExercisesDocument20 pagesCardiovascular Responses To Antigravity Muscle Loading During Head-Down Tilt at Rest and After Dynamic ExercisesAnonymous b2k9ABe7eNo ratings yet
- 9710562Document4 pages9710562Anonymous b2k9ABe7eNo ratings yet
- Nonlinear Dynamics of Multi-Component Bose-Einstein CondensatesDocument13 pagesNonlinear Dynamics of Multi-Component Bose-Einstein CondensatesAnonymous b2k9ABe7eNo ratings yet
- Gravity-Antigravity Interplay on Mpc ScaleDocument3 pagesGravity-Antigravity Interplay on Mpc ScaleAnonymous b2k9ABe7eNo ratings yet
- Anti-Gravity Treadmill Can Promote Aerobic ExercisDocument5 pagesAnti-Gravity Treadmill Can Promote Aerobic ExercisAnonymous b2k9ABe7eNo ratings yet
- Amman and Labruyere 2017 Letter To The EditorDocument3 pagesAmman and Labruyere 2017 Letter To The EditorAnonymous b2k9ABe7eNo ratings yet
- Femtosecond Laser Structuring of Janus Foam: Water Spontaneous Antigravity Unidirectional PenetratioDocument4 pagesFemtosecond Laser Structuring of Janus Foam: Water Spontaneous Antigravity Unidirectional PenetratioAnonymous b2k9ABe7eNo ratings yet
- Antigravity ESD - Double-Balloon-Assisted Underwater With Traction Hybrid TechniqueDocument6 pagesAntigravity ESD - Double-Balloon-Assisted Underwater With Traction Hybrid TechniqueAnonymous b2k9ABe7eNo ratings yet
- LMA Fast TrackDocument2 pagesLMA Fast TrackLeandro AlmeidaNo ratings yet
- Ayushman Bharat - KailashDocument11 pagesAyushman Bharat - KailashKailash NagarNo ratings yet
- IntroductiontoEpidemiologyandPublicHealth AnswersDocument17 pagesIntroductiontoEpidemiologyandPublicHealth AnswersDiamond_136100% (2)
- Science 5Document81 pagesScience 5Michael Joseph Santos100% (2)
- 00-30juni 2023 Data Stok FLDocument98 pages00-30juni 2023 Data Stok FLSunaryo AryandaNo ratings yet
- Diatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDocument13 pagesDiatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDani Daniela100% (1)
- All Topics - 2008-2011 - ADocument37 pagesAll Topics - 2008-2011 - ADebangshu KumarNo ratings yet
- Drug Study AdalatDocument4 pagesDrug Study AdalatLea CelestialNo ratings yet
- Hypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Document81 pagesHypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Alan K MhamadNo ratings yet
- Republic of The PhilippinesDocument95 pagesRepublic of The Philippineshitler dangatanNo ratings yet
- Obesity Exercise PrescriptionDocument34 pagesObesity Exercise Prescriptionkhushbu88% (8)
- Physiotherapy in LeprosyDocument4 pagesPhysiotherapy in LeprosymichaelsophianNo ratings yet
- DiarrheaDocument24 pagesDiarrheaash ashNo ratings yet
- Pelvic Floor Exercises in The Elderly Irmina Nahon1Document34 pagesPelvic Floor Exercises in The Elderly Irmina Nahon1Anonymous C7H7wS6No ratings yet
- IRB Definitions (Is It Research? and Definitions of Exempt, Expedited and Full)Document4 pagesIRB Definitions (Is It Research? and Definitions of Exempt, Expedited and Full)analyn123No ratings yet
- v1 High Sensitivity C-Reactive Protein HSCDocument2 pagesv1 High Sensitivity C-Reactive Protein HSCKhendy SugihartoNo ratings yet
- Portfolio Template for Diploma in Occupational MedicineDocument11 pagesPortfolio Template for Diploma in Occupational MedicineChengyuan ZhangNo ratings yet
- Medical Surgical Treatments For EDDocument31 pagesMedical Surgical Treatments For EDskumar_p7No ratings yet
- Aa 1 MasterRQsDocument93 pagesAa 1 MasterRQsSadhana SabhandasaniNo ratings yet
- RAV Admission Notice for Ayurveda CoursesDocument4 pagesRAV Admission Notice for Ayurveda CoursesBhargav KalalNo ratings yet
- Audit of Barangay Health Centers in PhilippinesDocument26 pagesAudit of Barangay Health Centers in PhilippineskenvysNo ratings yet
- Cardiogenic Shock Causes and TreatmentDocument43 pagesCardiogenic Shock Causes and TreatmentGalih Arief Harimurti WawolumajaNo ratings yet
- Philips Respironics Bipap ST Niv Noninvasive VentilatorDocument2 pagesPhilips Respironics Bipap ST Niv Noninvasive Ventilatorsonia87No ratings yet
- Strategic PlanDocument84 pagesStrategic PlanAurutchat VichaiditNo ratings yet
- PhobiasDocument10 pagesPhobiasapi-276690632No ratings yet
- Chapter 3 PsychDocument12 pagesChapter 3 Psychred_gyrl9282No ratings yet
- ReviewerDocument20 pagesReviewerYang MolosNo ratings yet
- Dental Anomalies II New PDFDocument34 pagesDental Anomalies II New PDFFranco Coco SartoriNo ratings yet
- Spironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabDocument2 pagesSpironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabAhmad KusayiriNo ratings yet
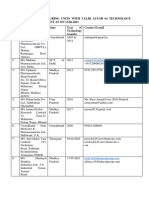
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Document5 pagesList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNo ratings yet