You might also like
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Tumor Med TysDocument21 pagesTumor Med TysTias DiahNo ratings yet
- TPE in Intensive Care - Dr. Teuku Yasir, SpAn-KIC, FIPMDocument17 pagesTPE in Intensive Care - Dr. Teuku Yasir, SpAn-KIC, FIPMTeuku FauzanoeNo ratings yet
- Adjuvan Anestesia PresentationDocument53 pagesAdjuvan Anestesia PresentationAdi Chand100% (1)
- Anestesi Pada ObstetriDocument20 pagesAnestesi Pada ObstetrieviherdiantiNo ratings yet
- Anestesi LaparoskopiDocument65 pagesAnestesi LaparoskopiArief Hariyadi SantosoNo ratings yet
- Refrat Obat Anestesi RilaDocument69 pagesRefrat Obat Anestesi RilaRila RivandaNo ratings yet
- Bone Cement Implantation SyndromeDocument19 pagesBone Cement Implantation SyndromeTafaNo ratings yet
- PVC Stoelting Coex 1Document29 pagesPVC Stoelting Coex 1Rudy SiahaanNo ratings yet
- Review Article: Pain Following Craniotomy: Reassessment of The Available OptionsDocument9 pagesReview Article: Pain Following Craniotomy: Reassessment of The Available Optionsssmall81No ratings yet
- Complicated AppendicitisDocument4 pagesComplicated AppendicitisMedardo ApoloNo ratings yet
- Perbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterDocument7 pagesPerbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterAfiani JannahNo ratings yet
- Osteonecrosis Caput FemurDocument23 pagesOsteonecrosis Caput FemurdrhendyjuniorNo ratings yet
- Supraclavicular Brachial Plexus BlockDocument2 pagesSupraclavicular Brachial Plexus BlockmagedemanNo ratings yet
- Perioperative Management 1203114432600412 4Document53 pagesPerioperative Management 1203114432600412 4polushkyNo ratings yet
- Compromised Patient (Klasifikasi Asa) : Surya Triharsa Andina Novita Sari Lisna Mirna Kuntari Muhamad SyafriDocument17 pagesCompromised Patient (Klasifikasi Asa) : Surya Triharsa Andina Novita Sari Lisna Mirna Kuntari Muhamad Syafridikadika_tansNo ratings yet
- Analgesi Dan Sedasi Di IcuDocument32 pagesAnalgesi Dan Sedasi Di IcuWidi Yuli HariantoNo ratings yet
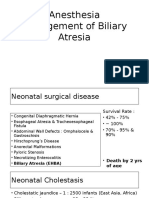
- 19 Anesthesia For Biliary AtresiaDocument19 pages19 Anesthesia For Biliary AtresiaDwiki Surya PrayogaNo ratings yet
- CVP Guided Deresuscitation in Managing Overload in Icu PDFDocument57 pagesCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- Anaesthetic Challenges and Management of Myelomeningocele RepairDocument6 pagesAnaesthetic Challenges and Management of Myelomeningocele RepairprastiaNo ratings yet
- Austin Journal of Anesthesia and AnalgesiaDocument3 pagesAustin Journal of Anesthesia and AnalgesiaAustin Publishing GroupNo ratings yet
- Acute Periopertive Pain Management (Sby)Document87 pagesAcute Periopertive Pain Management (Sby)Adam KurniaNo ratings yet
- Daftar Nilai Matrik BA Dan BI T.A. 2017-2018 PDFDocument138 pagesDaftar Nilai Matrik BA Dan BI T.A. 2017-2018 PDFNeni MartiniNo ratings yet
- AnestesiDocument11 pagesAnestesiAnonymous 8w9QEGNo ratings yet
- 145 One Lung VentilationDocument6 pages145 One Lung VentilationEyad AbdeljawadNo ratings yet
- CASP Checklist: Case Control Study How To Use This Appraisal ToolDocument6 pagesCASP Checklist: Case Control Study How To Use This Appraisal Toolanon_770867052No ratings yet
- Awake IntubationDocument35 pagesAwake IntubationEbeneser SitepuNo ratings yet
- Bimbingan ThoraksDocument71 pagesBimbingan ThoraksHedya Nadhrati SururaNo ratings yet
- BGA Acid Base Stepwise PradikDocument43 pagesBGA Acid Base Stepwise PradikZulfadly NuralimNo ratings yet
- EPOSTER HARIO-dikonversiDocument1 pageEPOSTER HARIO-dikonversiHario HendrokoNo ratings yet
- Guidelines For The Management of Superior Vena Cava ObstructDocument2 pagesGuidelines For The Management of Superior Vena Cava ObstructFuji Seprinur HidayatNo ratings yet
- Jurnal Reading Rizki Widya Kirana - 03012236Document15 pagesJurnal Reading Rizki Widya Kirana - 03012236R Widya KiranaNo ratings yet
- Terapi PaliatifDocument46 pagesTerapi PaliatifViviViviNo ratings yet
- VAE Venous Air Embolism GuideDocument11 pagesVAE Venous Air Embolism GuideAndini RizkyNo ratings yet
- CombinedDocument3 pagesCombinedSolape Akin-WilliamsNo ratings yet
- Taping OA Genu Dr. SIsca Susantio, Sp. KFRDocument11 pagesTaping OA Genu Dr. SIsca Susantio, Sp. KFRDsk IndryNo ratings yet
- Antikoagulan JurnalDocument5 pagesAntikoagulan JurnalansyemomoleNo ratings yet
- Dysuria Diagnosis AlgorithmDocument9 pagesDysuria Diagnosis AlgorithmM Fikri BetriandaNo ratings yet
- Teknik Anestesi UmumDocument128 pagesTeknik Anestesi UmumAkmalNourNo ratings yet
- Level of Cords of Brachial Plexus Lateral, Medial and Posterior (Named According To Relation To Axillary Artery)Document6 pagesLevel of Cords of Brachial Plexus Lateral, Medial and Posterior (Named According To Relation To Axillary Artery)tomlawson88No ratings yet
- Operative ObstetricsDocument6 pagesOperative ObstetricsGrasya ZackieNo ratings yet
- Intepretasi EKG (DR Eka)Document93 pagesIntepretasi EKG (DR Eka)Danil Anugrah JayaNo ratings yet
- Anestesi Pediatri Semester 7Document101 pagesAnestesi Pediatri Semester 7jackyploesNo ratings yet
- Anesthesia CHD Non Cardiac SurgeryDocument97 pagesAnesthesia CHD Non Cardiac SurgeryDon DavidNo ratings yet
- MorganDocument14 pagesMorganAdi WijayantoNo ratings yet
- Trombosis Vena Dalam: Pendidikan Kedokteran Berkelanjutan (PKB) XXI 2013Document13 pagesTrombosis Vena Dalam: Pendidikan Kedokteran Berkelanjutan (PKB) XXI 2013IkaNo ratings yet
- Diagnosis and Management of Stable AnginaDocument40 pagesDiagnosis and Management of Stable AnginaIno HajrinNo ratings yet
- Jurnal AnastesiDocument10 pagesJurnal AnastesiAnonymous m07Ogz0rNo ratings yet
- Midgut Volvulus 2018Document2 pagesMidgut Volvulus 2018zzzNo ratings yet
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNo ratings yet
- Pregnancy With MS MRDocument74 pagesPregnancy With MS MRRaj K SharmaNo ratings yet
- Anesthesia For Transsphenoidal Pituitary Surgery.Document6 pagesAnesthesia For Transsphenoidal Pituitary Surgery.ismaelNo ratings yet
- Patient Controlled AnalgesiaDocument35 pagesPatient Controlled AnalgesiamochkurniawanNo ratings yet
- Adrenergic AgonistsDocument52 pagesAdrenergic AgonistsTsegaye HailuNo ratings yet
- Anatomical anomalies in retractile testesDocument7 pagesAnatomical anomalies in retractile testesAhmad Rahmat Ramadhan TantuNo ratings yet
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansNo ratings yet
- Current Diagnosis and Management of Hirschsprung's DiseaseDocument20 pagesCurrent Diagnosis and Management of Hirschsprung's DiseaseIyan AsianaNo ratings yet
- Laparoscopic Cholecystectomy Under Spinal Anaesthesia: A Prospective StudyDocument4 pagesLaparoscopic Cholecystectomy Under Spinal Anaesthesia: A Prospective Studyrazaqhussain00No ratings yet
- 7 Early Clinical Experience Using High Intensity Focused Ultrasound For Palliation of Inoperable Pancreatic CancerDocument7 pages7 Early Clinical Experience Using High Intensity Focused Ultrasound For Palliation of Inoperable Pancreatic CancerEvelynLisettVargasNo ratings yet
- NO Nama Materi Pengajar Dr. ErikDocument3 pagesNO Nama Materi Pengajar Dr. ErikDjustiela KarrangNo ratings yet
- Spinal Deformity DJDocument2 pagesSpinal Deformity DJDjustiela KarrangNo ratings yet
- Pembagian Tugas Presentasi Bimbingan Daring: NO Nama Materi Pengajar Dr. IrvanDocument2 pagesPembagian Tugas Presentasi Bimbingan Daring: NO Nama Materi Pengajar Dr. IrvanDjustiela KarrangNo ratings yet
- Lapkas THTDocument2 pagesLapkas THTDjustiela KarrangNo ratings yet
- Adoption of Sacubitril/Valsartan For The Management of Patients With Heart FailureDocument12 pagesAdoption of Sacubitril/Valsartan For The Management of Patients With Heart FailureDjustiela KarrangNo ratings yet
- Management of Obesity: Ournal of Linical NcologyDocument13 pagesManagement of Obesity: Ournal of Linical NcologyDjustiela KarrangNo ratings yet
- Lapkas THTDocument2 pagesLapkas THTDjustiela KarrangNo ratings yet
- Lapkas THTDocument2 pagesLapkas THTDjustiela KarrangNo ratings yet
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Document4 pagesComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangNo ratings yet
- Management of Obesity: Ournal of Linical NcologyDocument13 pagesManagement of Obesity: Ournal of Linical NcologyDjustiela KarrangNo ratings yet
- Management of Obesity: Ournal of Linical NcologyDocument13 pagesManagement of Obesity: Ournal of Linical NcologyDjustiela KarrangNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument29 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDian Istiqamah MardhatillahNo ratings yet
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Document4 pagesComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangNo ratings yet
- Lapkas Callus PDFDocument30 pagesLapkas Callus PDFDjustiela KarrangNo ratings yet
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Document4 pagesComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangNo ratings yet
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18 PDFDocument4 pagesComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18 PDFDjustiela KarrangNo ratings yet
- Lapkas CallusDocument4 pagesLapkas CallusDjustiela KarrangNo ratings yet
- Lapkas Callus PDFDocument30 pagesLapkas Callus PDFDjustiela KarrangNo ratings yet
- Ignatavicius TOCDocument9 pagesIgnatavicius TOCjennaaahhhNo ratings yet
- EMBRYOLOGYDocument4 pagesEMBRYOLOGYbhagavan prasadNo ratings yet
- 1615 PDFDocument897 pages1615 PDFAmmar Mohamad Ziyadi100% (2)
- Journal Brain Gym and Mirror Box Therapy FIXDocument28 pagesJournal Brain Gym and Mirror Box Therapy FIXNur HasanahNo ratings yet
- Ehlers-Danlos Syndromes (EDS) : Fiona Li Pharm D Candidate University of Saint Joseph School of PharmacyDocument22 pagesEhlers-Danlos Syndromes (EDS) : Fiona Li Pharm D Candidate University of Saint Joseph School of PharmacyDiogo CapellaNo ratings yet
- Injury: Jae-Woo Cho, Jinil Kim, Won-Tae Cho, William T. Kent, Hyung-Jin Kim, Jong-Keon OhDocument10 pagesInjury: Jae-Woo Cho, Jinil Kim, Won-Tae Cho, William T. Kent, Hyung-Jin Kim, Jong-Keon OhKrishna CaitanyaNo ratings yet
- Smart Health Care ReportDocument86 pagesSmart Health Care ReportHEESOO LEENo ratings yet
- Rhs 15s Combined 12 Languages Translated PDFDocument56 pagesRhs 15s Combined 12 Languages Translated PDFRitaMorgadoLemosNo ratings yet
- Huguet 2019 Deficient Emotional Self RegulationDocument7 pagesHuguet 2019 Deficient Emotional Self RegulationIríada VerbeekNo ratings yet
- Research InstrumentDocument3 pagesResearch InstrumentMark Warren Atienza RevellameNo ratings yet
- Insights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityDocument4 pagesInsights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityHusnat hussainNo ratings yet
- Role of Nurses in Health Care SystemDocument1 pageRole of Nurses in Health Care Systemcadolly carnoiseNo ratings yet
- Interpretation MRCPCH 2009 Site: For Part 2 Exam For Part 2 ExamDocument35 pagesInterpretation MRCPCH 2009 Site: For Part 2 Exam For Part 2 Examyassine100% (1)
- Adoption Issues Young Children Face DevelopmentallyDocument6 pagesAdoption Issues Young Children Face DevelopmentallyNurfaradilla NasriNo ratings yet
- WCH Open Letter On Who Pandemic Treaty 2Document2 pagesWCH Open Letter On Who Pandemic Treaty 2Jamie White100% (3)
- Latihan Soal TERMINOLOGI MEDISDocument10 pagesLatihan Soal TERMINOLOGI MEDISdelia yuliantiNo ratings yet
- Forensic Drug AnalysisDocument6 pagesForensic Drug AnalysisIJRASETPublicationsNo ratings yet
- Research EthicsDocument2 pagesResearch EthicsCarla HAHAHAHANo ratings yet
- Intellectual DiabilityDocument10 pagesIntellectual DiabilityAngelo PapimNo ratings yet
- The Missing Key To Thyroid HealthDocument22 pagesThe Missing Key To Thyroid HealthEmily Williams0% (1)
- Dexmedetomidine Vs Propofol - RCT - Merry Andriany 406162043Document7 pagesDexmedetomidine Vs Propofol - RCT - Merry Andriany 406162043Merry AndrianyNo ratings yet
- Physiological Peculiarities, Vices, Senses, and Behaviour of HorsesDocument13 pagesPhysiological Peculiarities, Vices, Senses, and Behaviour of HorsesSantosh RajaNo ratings yet
- Coping Methods and Counseling for Grief Across AgesDocument8 pagesCoping Methods and Counseling for Grief Across AgesDaciana DumitrescuNo ratings yet
- Ethical Concerns in Family Therapy: Paulette M. Hines and Rachel T. Hare-MustinDocument7 pagesEthical Concerns in Family Therapy: Paulette M. Hines and Rachel T. Hare-MustinPaula CelsieNo ratings yet
- Jurnal Reading: Sit Dolor AmetDocument20 pagesJurnal Reading: Sit Dolor AmetLiri AndiyaniNo ratings yet
- Global Plan of Action:: Health Systems Address Violence Against Women and GirlsDocument32 pagesGlobal Plan of Action:: Health Systems Address Violence Against Women and GirlssofiabloemNo ratings yet
- Manifestations of ViolenceDocument2 pagesManifestations of ViolenceProjectSakinahDCNo ratings yet
- GO5509 ResidenDocument4 pagesGO5509 ResidenBrunoNo ratings yet
- Impact of Sleep Quality On Post-Stroke Anxiety in Stroke PatientsDocument9 pagesImpact of Sleep Quality On Post-Stroke Anxiety in Stroke PatientsTasya Putri Widyastika 2111166333No ratings yet
- Pregnancy BrochureDocument2 pagesPregnancy Brochureapi-464628523No ratings yet