You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Assessment of Hematologic Disorders: Patient HistoryDocument3 pagesAssessment of Hematologic Disorders: Patient HistoryUSC Upstate Nursing CoachesNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Musculoskeletal ProblemsDocument12 pagesMusculoskeletal ProblemsUSC Upstate Nursing CoachesNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Compilation of Class 10.26.10Document13 pagesCompilation of Class 10.26.10USC Upstate Nursing CoachesNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Assessment of Hematologic Disorders - Physical AssessmentDocument3 pagesAssessment of Hematologic Disorders - Physical AssessmentUSC Upstate Nursing CoachesNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Cheat Sheet RevisedDocument2 pagesCheat Sheet RevisedUSC Upstate Nursing Coaches100% (3)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
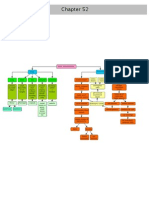
- Chapter 52 Bone ClassificationsDocument1 pageChapter 52 Bone ClassificationsUSC Upstate Nursing CoachesNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Lupus, Sclerosis, Lymes, Fibromyalgia GoutDocument2 pagesLupus, Sclerosis, Lymes, Fibromyalgia GoutUSC Upstate Nursing CoachesNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Sulfonylurea Agents (Diabinese, Glucotrol, Diabeta) : 2. Meglitinide Analogues (Prandin)Document11 pagesSulfonylurea Agents (Diabinese, Glucotrol, Diabeta) : 2. Meglitinide Analogues (Prandin)Kristin EdwardsNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Memory Pics: NeurologicalDocument12 pagesMemory Pics: NeurologicalUSC Upstate Nursing CoachesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- HIV - AIDS, Allergies, AutoimmunityDocument6 pagesHIV - AIDS, Allergies, AutoimmunityUSC Upstate Nursing CoachesNo ratings yet
- Memory Pics Hematology OncologyDocument28 pagesMemory Pics Hematology OncologyKristin EdwardsNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Chapter 41 Hematologic ProblemsDocument6 pagesChapter 41 Hematologic ProblemsUSC Upstate Nursing CoachesNo ratings yet
- Memory Pics: SensoryDocument12 pagesMemory Pics: SensoryUSC Upstate Nursing CoachesNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Immunity & Cancer (Spartanburg)Document17 pagesImmunity & Cancer (Spartanburg)USC Upstate Nursing CoachesNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Memory Pics: MusculoskeletalDocument17 pagesMemory Pics: MusculoskeletalUSC Upstate Nursing CoachesNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- CH 54 AmputationsDocument12 pagesCH 54 AmputationsUSC Upstate Nursing CoachesNo ratings yet
- Assessment of The Hematologic SystemDocument36 pagesAssessment of The Hematologic SystemUSC Upstate Nursing CoachesNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CH 53: Musculoskeletal Problems (Per Amendolair)Document32 pagesCH 53: Musculoskeletal Problems (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- Memory Pics: RenalDocument8 pagesMemory Pics: RenalUSC Upstate Nursing CoachesNo ratings yet
- Chapter 21Document4 pagesChapter 21USC Upstate Nursing CoachesNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Male Reproductive ProblemsDocument6 pagesMale Reproductive ProblemsUSC Upstate Nursing CoachesNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Chapter 19Document6 pagesChapter 19USC Upstate Nursing CoachesNo ratings yet
- CH 54: Musculoskeletal Trauma (Per Amendolair)Document54 pagesCH 54: Musculoskeletal Trauma (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- CH 41: Hematological Assessment (Per Amendolair)Document28 pagesCH 41: Hematological Assessment (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- Chapter 22: Crossword (Per Black)Document3 pagesChapter 22: Crossword (Per Black)USC Upstate Nursing CoachesNo ratings yet
- Interventions For Clients With Hematologic ProblemsDocument50 pagesInterventions For Clients With Hematologic ProblemsUSC Upstate Nursing CoachesNo ratings yet
- CH 52: Musculoskeletal Assessment (Per Amendolair)Document27 pagesCH 52: Musculoskeletal Assessment (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- White Blood Cells (WBC) TotalDocument1 pageWhite Blood Cells (WBC) TotalUSC Upstate Nursing CoachesNo ratings yet
- Influence of Single Nucleotide Polymorphisms (SNPS) in Genetic Susceptibility Towards Periprosthetic OsteolysisDocument13 pagesInfluence of Single Nucleotide Polymorphisms (SNPS) in Genetic Susceptibility Towards Periprosthetic OsteolysisLU LAM THIENNo ratings yet
- Understanding Bisphosphonates and Osteonecrosis of The JawDocument9 pagesUnderstanding Bisphosphonates and Osteonecrosis of The JawGabriela OlateNo ratings yet
- Molecular and Cellular Endocrinology: EditorialDocument2 pagesMolecular and Cellular Endocrinology: EditorialSheila GouveiaNo ratings yet
- Bone and Mineral Metabolism in Health and DiseaseDocument14 pagesBone and Mineral Metabolism in Health and Diseasebiniam MesfinNo ratings yet
- Apoptosis - An Introduction For The Endodontist PDFDocument9 pagesApoptosis - An Introduction For The Endodontist PDFRamona MateiNo ratings yet
- Intramembranous Ossification & Endochondral Ossification PDFDocument41 pagesIntramembranous Ossification & Endochondral Ossification PDFKayla Joezette100% (1)
- The Pathophysiology of Otosclerosis: Review of Current ResearchDocument6 pagesThe Pathophysiology of Otosclerosis: Review of Current ResearchFelipeAsenjoÁlvarezNo ratings yet
- HypercalcemiaDocument26 pagesHypercalcemiaPiya TangNo ratings yet
- Full PDFDocument6 pagesFull PDFChuco HarrisonNo ratings yet
- The Natural Bone Building HandbookDocument60 pagesThe Natural Bone Building HandbookSunpetal2No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Bone Formation and MetabolismDocument38 pagesBone Formation and MetabolismNovia RizqiNo ratings yet
- In Situ Accumulation of Advanced Glycation Endproducts (Ages) in Bone Matrix and Its Correlation With Osteoclastic Bone ResorptionDocument22 pagesIn Situ Accumulation of Advanced Glycation Endproducts (Ages) in Bone Matrix and Its Correlation With Osteoclastic Bone Resorptiondumboo21No ratings yet
- Calcium and Phosphorus Metabolism and Its Importance in OrthodonticsDocument56 pagesCalcium and Phosphorus Metabolism and Its Importance in OrthodonticsVijay ChinthaNo ratings yet
- Normal Bone Formation and RemodelingDocument4 pagesNormal Bone Formation and RemodelingFernando AnibanNo ratings yet
- Biomaterials in OrthepadicsDocument455 pagesBiomaterials in OrthepadicsDeva Raj100% (2)
- Reviews: Fracture Healing: Mechanisms and InterventionsDocument10 pagesReviews: Fracture Healing: Mechanisms and InterventionsFatrika DewiNo ratings yet
- Case Study ON Tibial Fracture: University of Saint LouisDocument50 pagesCase Study ON Tibial Fracture: University of Saint LouisJM RomiasNo ratings yet
- Essential Guide To Vita MindDocument204 pagesEssential Guide To Vita Mindnguyen thu trangNo ratings yet
- Osteoporosis A Guide To Prevention and Treatment Harvard HealthDocument57 pagesOsteoporosis A Guide To Prevention and Treatment Harvard HealthFenil Parekh100% (5)
- Gingival Absorption of Rat Periodontal Disease Model and Rat Tooth Movement ModelDocument7 pagesGingival Absorption of Rat Periodontal Disease Model and Rat Tooth Movement ModelLouis HutahaeanNo ratings yet
- Bone Fracture & RemodellingDocument39 pagesBone Fracture & Remodellingokware rodrickNo ratings yet
- FRAX ScoreDocument42 pagesFRAX ScoreDr SheetalNo ratings yet
- A211 Module 1 SkeletalDocument10 pagesA211 Module 1 Skeletalシファ ムスタファNo ratings yet
- Nutrition in OrthodonticsDocument51 pagesNutrition in OrthodonticsShweta DU80% (5)
- A Decade of Bisphosphonate Bone Complications: What It Has Taught Us About Bone PhysiologyDocument12 pagesA Decade of Bisphosphonate Bone Complications: What It Has Taught Us About Bone PhysiologyNatalia Camila Rodríguez LatorreNo ratings yet
- Assignment For Calcitonin HormoneDocument6 pagesAssignment For Calcitonin HormoneSAKARIYE MAXAMEDNo ratings yet
- Biochemical Markers of Bone Turnover: DR Jemil Makadia PG 3rd Year Biochemistry Dept. LHMCDocument26 pagesBiochemical Markers of Bone Turnover: DR Jemil Makadia PG 3rd Year Biochemistry Dept. LHMCJemil MakadiaNo ratings yet
- Membrane Transport: To Accompany Biochemistry, 2/e by Reginald Garrett and Charles GrishamDocument79 pagesMembrane Transport: To Accompany Biochemistry, 2/e by Reginald Garrett and Charles GrishamMarione Thea RodriguezNo ratings yet
- AwalMart Catalogue2Document146 pagesAwalMart Catalogue2zulmalc100% (3)
- Dendritic Cells and PD - Grupo 1Document22 pagesDendritic Cells and PD - Grupo 1Carlos Jimenez Carlos BossioNo ratings yet