You might also like
- Carol Anthony and Hanna Moog Healing Yourself The Cosmic WayDocument149 pagesCarol Anthony and Hanna Moog Healing Yourself The Cosmic WayRiccardo Escher100% (1)
- Test Bank Lutzs Nutrition and Diet Therapy 7th Edition Erin e MazurDocument104 pagesTest Bank Lutzs Nutrition and Diet Therapy 7th Edition Erin e MazurMicheal Singh100% (23)
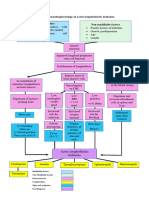
- Pathophysiology of Chronic Glomerulonephritis: LegendDocument1 pagePathophysiology of Chronic Glomerulonephritis: LegendGeorich Narciso50% (4)
- UntitledDocument380 pagesUntitledRaja Umar WaqarNo ratings yet
- ExcreDocument3 pagesExcreKristin Charm MascareñasNo ratings yet
- Pathology GlomerulonephritisDocument4 pagesPathology GlomerulonephritisGerardLum100% (2)
- Glomerulonephritis 2019Document31 pagesGlomerulonephritis 2019EsoklailNo ratings yet
- Renal DX Flowcharts & Trigger WordsDocument4 pagesRenal DX Flowcharts & Trigger WordsAmber LeJeuneNo ratings yet
- AUBF Lec - Renal DiseasesDocument6 pagesAUBF Lec - Renal Diseasescdsteenkamp18No ratings yet
- C370 Lecture 2 Lecture Notes Part 2Document45 pagesC370 Lecture 2 Lecture Notes Part 2Yan Mui ChanNo ratings yet
- Menigitis & EncephalitisDocument38 pagesMenigitis & EncephalitisKim GonzalesNo ratings yet
- Quality Assessment, Renal Disease & Urine ScreeningDocument15 pagesQuality Assessment, Renal Disease & Urine ScreeningAnya IgnacioNo ratings yet
- Patho MicroDocument17 pagesPatho Microjyothsna yarraNo ratings yet
- Renal Diseases NotesDocument4 pagesRenal Diseases NotesJanine CabreraNo ratings yet
- 7 Renal Disease Student CopyDocument34 pages7 Renal Disease Student Copyrbm121415chyNo ratings yet
- Dr. Dhian Endarwati, Spa Maret 2017Document60 pagesDr. Dhian Endarwati, Spa Maret 2017Diany LarasatiNo ratings yet
- อ.บัญชา Glomerular - disease - handoutพี่ดาวDocument142 pagesอ.บัญชา Glomerular - disease - handoutพี่ดาวNitaan TangsritrakulNo ratings yet
- PATH - Nephritic SyndromeDocument14 pagesPATH - Nephritic SyndromeMuhamad Zul ImanNo ratings yet
- 17 MedsurgDocument3 pages17 MedsurgLomocso Baron JudyNo ratings yet
- Activity On Renal DiseasesDocument6 pagesActivity On Renal DiseasesRicca Christyl SumalpongNo ratings yet
- Renal DiseaseDocument6 pagesRenal DiseaseyeonjiNo ratings yet
- Disorder Etiology: Acute GlomerulonephritisDocument1 pageDisorder Etiology: Acute GlomerulonephritisChynna Izzabelle Alcantara AbellanaNo ratings yet
- Nephritic SyndromeDocument2 pagesNephritic Syndromevalari8069No ratings yet
- Lecture 7.8.9 - Glomerulopathies (Including Nephritic, Nephrotic, Minimal Change, Focal Segmental Glomerulosclerosis and Membrane Nephropathy)Document92 pagesLecture 7.8.9 - Glomerulopathies (Including Nephritic, Nephrotic, Minimal Change, Focal Segmental Glomerulosclerosis and Membrane Nephropathy)mihalachemirelaNo ratings yet
- MHD Exam 5 MaterialDocument122 pagesMHD Exam 5 Materialnaexuis5467100% (1)
- Renal DiseasesDocument1 pageRenal DiseasesRebecca BernalNo ratings yet
- Streptococcus Infection, On TheDocument3 pagesStreptococcus Infection, On TheMonica DomingoNo ratings yet
- GLOMERULONEPHRITIS (Bright's Disease)Document8 pagesGLOMERULONEPHRITIS (Bright's Disease)Anjitha K. JNo ratings yet
- Clinical Presentation and Causes of Acute Renal FailureDocument27 pagesClinical Presentation and Causes of Acute Renal FailureradhiinathahirNo ratings yet
- Kahoots 8 - Renal Physiology PDFDocument3 pagesKahoots 8 - Renal Physiology PDFJoshua LanzonNo ratings yet
- Clin Path Lab 6 UrinalysisDocument5 pagesClin Path Lab 6 Urinalysisapi-3743217100% (6)
- SPIDER WEB ACUTE RENAL FAILURE (ARF/AKIDocument3 pagesSPIDER WEB ACUTE RENAL FAILURE (ARF/AKITien KartiniNo ratings yet
- Pathophysiology of Chronic Kidney Disease (CKDDocument5 pagesPathophysiology of Chronic Kidney Disease (CKDSteffi MurielNo ratings yet
- Patient Based Patho ALL Super Final Pro MaxDocument1 pagePatient Based Patho ALL Super Final Pro MaxMarc SorianoNo ratings yet
- Causes of an elevated serum lactate dehydrogenase levelDocument3 pagesCauses of an elevated serum lactate dehydrogenase levelSantiago IllarramendiNo ratings yet
- Nephrology Syndromes GuideDocument17 pagesNephrology Syndromes GuideCitra Wulandari SofyanNo ratings yet
- PathophysioDocument1 pagePathophysioJanine GarciaNo ratings yet
- Lecturio 3663 JaundiceDocument12 pagesLecturio 3663 JaundicePranjali WeladiNo ratings yet
- Casts Composition Associated ConditionsDocument1 pageCasts Composition Associated ConditionsPrativa RajbhandariNo ratings yet
- 2.2.3.1 Diathesis HemorragikDocument20 pages2.2.3.1 Diathesis HemorragikaiysahmirzaNo ratings yet
- Kidney: Term StatementDocument3 pagesKidney: Term Statementselam kalayuNo ratings yet
- Diagnosing and Managing Hematuria: A ReviewDocument7 pagesDiagnosing and Managing Hematuria: A Reviewfernanda garnicaNo ratings yet
- Renal DiseaseDocument4 pagesRenal DiseaseApril Lady Faith P. PaundogNo ratings yet
- Pathophysiology of Nephrotic SyndromeDocument1 pagePathophysiology of Nephrotic SyndromeKristian Karl Bautista Kiw-isNo ratings yet
- Week 7. Renal Pathology Continued.Document9 pagesWeek 7. Renal Pathology Continued.Amber LeJeuneNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Disseminated Intravascular CoagulationDocument2 pagesDisseminated Intravascular CoagulationGerardLum100% (1)
- NICOLE BLANCH BUENAVISTA - Module 6 Test IIDocument1 pageNICOLE BLANCH BUENAVISTA - Module 6 Test IINICOLE BLANCH BUENAVISTANo ratings yet
- Pathophysiology (Chronic Renal Failure)Document3 pagesPathophysiology (Chronic Renal Failure)marshmalou86% (7)
- 6. Kidney GM Eng 2020Document31 pages6. Kidney GM Eng 2020snowrose2609No ratings yet
- I. Pathophysiology A. Algorithm: Predisposing Factors: Etiology: Precipitating FactorsDocument3 pagesI. Pathophysiology A. Algorithm: Predisposing Factors: Etiology: Precipitating FactorsDane YelNo ratings yet
- Rina Ramayani Komplikasi SN KONIKA XVIIDocument26 pagesRina Ramayani Komplikasi SN KONIKA XVIIirene aureliaNo ratings yet
- Nephrotic synd (2)Document21 pagesNephrotic synd (2)238439904No ratings yet
- Chapter 7Document2 pagesChapter 7Mychelle MenesNo ratings yet
- Asuhan Keperawatan Pada Pasien Dengan Chronic Kidney DiseasesDocument24 pagesAsuhan Keperawatan Pada Pasien Dengan Chronic Kidney DiseasestidaktahudiriNo ratings yet
- Urogenital Imaging: A Problem-Oriented ApproachFrom EverandUrogenital Imaging: A Problem-Oriented ApproachS. MorcosRating: 3 out of 5 stars3/5 (1)
- Aldosterone: International Series of Monographs in Pure and Applied BiologyFrom EverandAldosterone: International Series of Monographs in Pure and Applied BiologyNo ratings yet
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- Database NormalizationDocument10 pagesDatabase NormalizationGlen David Efrenson SupangaNo ratings yet
- Community Health NursingDocument1 pageCommunity Health NursingGlen David Efrenson SupangaNo ratings yet
- Boxing Tip #1: Jab TapDocument39 pagesBoxing Tip #1: Jab TapGlen David Efrenson SupangaNo ratings yet
- Boxing Tip #1: Jab TapDocument39 pagesBoxing Tip #1: Jab TapGlen David Efrenson SupangaNo ratings yet
- 9447-Article Text-33080-1-10-20160306Document10 pages9447-Article Text-33080-1-10-20160306Nagib MuhammadNo ratings yet
- GASTRO Terminology & GlossaryDocument13 pagesGASTRO Terminology & GlossaryEugenia Lopez Delgado100% (1)
- Diagnosis and Management of Oral Candidosis: PracticeDocument7 pagesDiagnosis and Management of Oral Candidosis: PracticeYerly Ramirez MuñozNo ratings yet
- Nonulcerative Blepharitis - Definition of Nonulcerative Blepharitis in The Medical Dictionary - by The Free Online Medical Dictionary, Thesaurus and EncyclopediaDocument1 pageNonulcerative Blepharitis - Definition of Nonulcerative Blepharitis in The Medical Dictionary - by The Free Online Medical Dictionary, Thesaurus and EncyclopediaFerni ArmantiNo ratings yet
- Materia Medica For The Respiratory System: Anti-CatarrhalsDocument4 pagesMateria Medica For The Respiratory System: Anti-CatarrhalskobkunkarbNo ratings yet
- SRS For Trigeminal Neuralgia and Epilepsy: DR Pantaleo Romanelli Scientific Director, Brain Radiosurgery, CDI, MilanoDocument34 pagesSRS For Trigeminal Neuralgia and Epilepsy: DR Pantaleo Romanelli Scientific Director, Brain Radiosurgery, CDI, MilanoPanNo ratings yet
- Body Composition in Sports 6WCCDocument25 pagesBody Composition in Sports 6WCCr9610337316No ratings yet
- Ge 101Document65 pagesGe 101samorales92No ratings yet
- Shanz - Ent 1.07 NoseDocument4 pagesShanz - Ent 1.07 NosePetrina XuNo ratings yet
- Directors Duties Indg417Document12 pagesDirectors Duties Indg417Muhammad RidwanNo ratings yet
- Caglar H.B. - SBRT For Lung CancerDocument51 pagesCaglar H.B. - SBRT For Lung CancerÖzgür Kara (OncoHealth)No ratings yet
- DVH Limits 4Document1 pageDVH Limits 4Dioni SandovalNo ratings yet
- Transitional Care: DR - Vinoli.S.G Professor HOD Medical Surgical Nursing Dept Universal College of Nursing BangaloreDocument15 pagesTransitional Care: DR - Vinoli.S.G Professor HOD Medical Surgical Nursing Dept Universal College of Nursing BangalorevinoliNo ratings yet
- Bipolar Disorder Signs, Causes, Diagnosis and TreatmentsDocument16 pagesBipolar Disorder Signs, Causes, Diagnosis and TreatmentsDeasy Arindi PutriNo ratings yet
- Chest Tube Thoracostomy: Patient EducationDocument2 pagesChest Tube Thoracostomy: Patient EducationPhilippe Ceasar C. BascoNo ratings yet
- Peritoneal Carcinomatosis and Its Mimics - Review of CT Findings For Differential DiagnosisDocument6 pagesPeritoneal Carcinomatosis and Its Mimics - Review of CT Findings For Differential DiagnosisDumitru RadulescuNo ratings yet
- Ajol File Journals - 473 - Articles - 200776 - Submission - Proof - 200776 5581 503678 1 10 20201026Document7 pagesAjol File Journals - 473 - Articles - 200776 - Submission - Proof - 200776 5581 503678 1 10 20201026hammed nurudeenNo ratings yet
- Approach To Patient With Glucocorticoid Induced Adrenal InsufficiencyDocument11 pagesApproach To Patient With Glucocorticoid Induced Adrenal InsufficiencyBHUENDOCRINE SRNo ratings yet
- Medical Equipment GuideDocument2 pagesMedical Equipment GuideMarisabel EchegarayNo ratings yet
- Adm Modules Science 9 2021 Week 1 4 ValidatedDocument30 pagesAdm Modules Science 9 2021 Week 1 4 ValidatedJea RacelisNo ratings yet
- DR Lal Pathlabs ARDocument203 pagesDR Lal Pathlabs ARAkash DhimanNo ratings yet
- Acute lateral medullary syndrome (Wallenberg syndrome) secondary to lateral medullary infarctDocument64 pagesAcute lateral medullary syndrome (Wallenberg syndrome) secondary to lateral medullary infarctAlvin Germo PasuquinNo ratings yet
- Literatura 6Document4 pagesLiteratura 6Анастасія КарпенкоNo ratings yet
- Bone Mineral Density (BMD) Test 2Document1 pageBone Mineral Density (BMD) Test 2Rica adriani SantikaNo ratings yet
- 12 Steps of AA in 40 CharactersDocument11 pages12 Steps of AA in 40 Charactersmike9diaz-689513No ratings yet
- Caranto vs. Bergesen D.Y. Phils., Inc.Document3 pagesCaranto vs. Bergesen D.Y. Phils., Inc.Courtney TirolNo ratings yet
- Anthracinum. - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANTINE HERINGDocument17 pagesAnthracinum. - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANTINE HERINGHarrison DavidsonNo ratings yet