You might also like
- Surgery: by DR - Mohammad Z. Abu Sheikha@Document145 pagesSurgery: by DR - Mohammad Z. Abu Sheikha@صقر حورانNo ratings yet
- USMLE Step 1 Rapid Review Classic Presentations (FA) Flashcards - MemorangDocument8 pagesUSMLE Step 1 Rapid Review Classic Presentations (FA) Flashcards - MemorangMohamed AbbasNo ratings yet
- Divine Intervention Episode 22 Obgyn Shelf Review PDFDocument167 pagesDivine Intervention Episode 22 Obgyn Shelf Review PDFSwisskelly1100% (1)
- Maternity and Pediatric Nursing 3rd EditionDocument347 pagesMaternity and Pediatric Nursing 3rd EditionTaylor Talley80% (15)
- Usmle QDocument46 pagesUsmle QRoh Jiten100% (1)
- Paediatrics & Biostatistics Notes - USMLE Step 2CKDocument102 pagesPaediatrics & Biostatistics Notes - USMLE Step 2CKDuncan89No ratings yet
- HY NBME Psych Review: Some MS4Document114 pagesHY NBME Psych Review: Some MS4Swisskelly1100% (2)
- USMLE Step 2 CK 6 Months Study Plan For 240Document1 pageUSMLE Step 2 CK 6 Months Study Plan For 240DhritisdiaryNo ratings yet
- 0 BOSH FrameworkDocument18 pages0 BOSH Frameworkharold fontiveros100% (1)
- Skin and MSK EverythingDocument31 pagesSkin and MSK EverythingBernard HernandezNo ratings yet
- PTSD Checklist (PCL)Document1 pagePTSD Checklist (PCL)Manikanta Sai KumarNo ratings yet
- Helminth ChartsDocument4 pagesHelminth ChartsDrbee10No ratings yet
- Abas 3 Chapter 5Document62 pagesAbas 3 Chapter 5GF David SalasNo ratings yet
- IM Tips For Step 2 CKDocument6 pagesIM Tips For Step 2 CKMohsin FarooqNo ratings yet
- Risk Factors - Step 2 PDFDocument5 pagesRisk Factors - Step 2 PDFAmberNo ratings yet
- Aquifer Case - Summary - FamilyMedicine21 - 12-YDocument10 pagesAquifer Case - Summary - FamilyMedicine21 - 12-YHyunsoo EllisNo ratings yet
- Lung Development and Anatomy ExplainedDocument91 pagesLung Development and Anatomy ExplainedPrarthanaNo ratings yet
- My Study Plan Guide For AmcDocument7 pagesMy Study Plan Guide For Amc0d&H 8No ratings yet
- Nbme Medicine Shelf Review Session 2Document142 pagesNbme Medicine Shelf Review Session 2Swisskelly1100% (1)
- Nbme Medicine Shelf Review Session 2Document142 pagesNbme Medicine Shelf Review Session 2Swisskelly1100% (1)
- Medicowesome - AnatomyDocument19 pagesMedicowesome - AnatomySubhashNo ratings yet
- Divine Intervention Episode 21 Peds Shelf Review PDFDocument139 pagesDivine Intervention Episode 21 Peds Shelf Review PDFSwisskelly1No ratings yet
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- Derm CodingDocument8 pagesDerm CodingVinay100% (1)
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Tank Cleaning ConsiderationsDocument1 pageTank Cleaning ConsiderationsAdele PollardNo ratings yet
- Advances in Pathobiology and Management of Paget’s Disease of BoneFrom EverandAdvances in Pathobiology and Management of Paget’s Disease of BoneSakamuri V. ReddyNo ratings yet
- Hematologic Pathology p48-64Document17 pagesHematologic Pathology p48-64zeroun24100% (1)
- Obstetics Simplified El-MowafiDocument515 pagesObstetics Simplified El-Mowafiapi-370504650% (2)
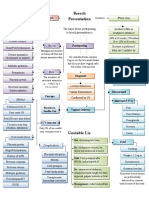
- BreechDocument1 pageBreechZiyadNo ratings yet
- A Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Fuel Gas Superheater 195-E-301 A/B: Mechanical - Data SheetDocument3 pagesFuel Gas Superheater 195-E-301 A/B: Mechanical - Data SheetZulfikar N JoelNo ratings yet
- A Presentation On Kit KatDocument9 pagesA Presentation On Kit KatRaju DoleyNo ratings yet
- Divine Intervention Episode 16 Bacterial Cases B: Some MS4Document11 pagesDivine Intervention Episode 16 Bacterial Cases B: Some MS4Swisskelly1No ratings yet
- Divine Intervention Episode 17 Diseases of The Pediatric Population Part 1Document14 pagesDivine Intervention Episode 17 Diseases of The Pediatric Population Part 1Swisskelly1No ratings yet
- Divine Intervention Episode 54 Comprehensive UsmleDocument69 pagesDivine Intervention Episode 54 Comprehensive UsmleWendy SierraNo ratings yet
- Divine Intervention Episode 5 Cardio A Physiology1Document18 pagesDivine Intervention Episode 5 Cardio A Physiology1Swisskelly1No ratings yet
- Divine Intervention Episode 13 Step 1 Metabolism Review A: Some MS4Document11 pagesDivine Intervention Episode 13 Step 1 Metabolism Review A: Some MS4Swisskelly1No ratings yet
- Divine Intervention Episode 6 20 Pharmacology CasesDocument21 pagesDivine Intervention Episode 6 20 Pharmacology CasesSwisskelly1No ratings yet
- Heme Testing Aid/APLS: Some PGY-1Document4 pagesHeme Testing Aid/APLS: Some PGY-1Swisskelly1No ratings yet
- Divine Intervention Episode 44 Usmle Anatomy Series Part 1Document11 pagesDivine Intervention Episode 44 Usmle Anatomy Series Part 1Swisskelly1No ratings yet
- Divine Intervention Episode 36 Usmle OphthalmologyDocument15 pagesDivine Intervention Episode 36 Usmle OphthalmologySwisskelly1No ratings yet
- Shoulder dystocia management and PPH treatmentDocument9 pagesShoulder dystocia management and PPH treatmentJeffrey HingNo ratings yet
- Med KeywordsDocument67 pagesMed KeywordsSwisskelly1No ratings yet
- Divine Intervention Episode 7 Viral Cases C2ffungal CasesDocument17 pagesDivine Intervention Episode 7 Viral Cases C2ffungal CasesSwisskelly1No ratings yet
- USMLE Step 1 Review in BiochemistryDocument18 pagesUSMLE Step 1 Review in BiochemistryDevindra 2k17No ratings yet
- Divine Intervention Episode 19 Neurology Shelf Review Part 1Document16 pagesDivine Intervention Episode 19 Neurology Shelf Review Part 1Swisskelly1No ratings yet
- HistCellBioUSMLEDocument25 pagesHistCellBioUSMLERushi ShahNo ratings yet
- Divine Intervention Episode 87 USMLE Step 1 Neuro ReviewDocument7 pagesDivine Intervention Episode 87 USMLE Step 1 Neuro ReviewSwisskelly1No ratings yet
- BIOL 215 - CWRU Final Exam Learning GoalsDocument32 pagesBIOL 215 - CWRU Final Exam Learning GoalsKesharaSSNo ratings yet
- Divine Intervention Episode 69 Usmle Anatomy Series Part 2Document9 pagesDivine Intervention Episode 69 Usmle Anatomy Series Part 2Swisskelly1No ratings yet
- Step1 Journey-To 271Document7 pagesStep1 Journey-To 271Nilay BhattNo ratings yet
- TAUS MethodDocument15 pagesTAUS MethodMyslife LyfNo ratings yet
- Anatomy and Behavioral Kaplan VIdeosDocument4 pagesAnatomy and Behavioral Kaplan VIdeosDiorella Marie López GonzálezNo ratings yet
- Councelling and History TakingDocument5 pagesCouncelling and History TakingbashingarNo ratings yet
- HHHHDocument36 pagesHHHHdger11No ratings yet
- Respiratory Physio UsmleDocument61 pagesRespiratory Physio UsmleDr.G.Bhanu Prakash100% (2)
- Brunner Step 2 CK Study PlanDocument2 pagesBrunner Step 2 CK Study PlanhellayeahNo ratings yet
- MEHLMANMEDICAL Microbiology Assessment 1 1Document75 pagesMEHLMANMEDICAL Microbiology Assessment 1 1Feroz RaZa SoomrOoNo ratings yet
- Pediatrics CMS form 3 key pointsDocument2 pagesPediatrics CMS form 3 key pointsusmleaddict proNo ratings yet
- Biliary Disorders and Pancreatic Conditions ExplainedDocument59 pagesBiliary Disorders and Pancreatic Conditions ExplainedErick Sioco InsertoNo ratings yet
- NBME 11 Answers To All Sections 2Document97 pagesNBME 11 Answers To All Sections 2hussainalmusawiNo ratings yet
- Goljan Respiratory NotesDocument21 pagesGoljan Respiratory Notesmedic2424100% (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Liquid Biopsy in Urogenital Cancers and its Clinical UtilityFrom EverandLiquid Biopsy in Urogenital Cancers and its Clinical UtilitySeyed Mohammad Kazem AghamirNo ratings yet
- Penis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPenis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Divine Intervention Episode 36 Usmle OphthalmologyDocument15 pagesDivine Intervention Episode 36 Usmle OphthalmologySwisskelly1No ratings yet
- Heme Testing Aid/APLS: Some PGY-1Document4 pagesHeme Testing Aid/APLS: Some PGY-1Swisskelly1No ratings yet
- Divine Intervention Episode 15 Metabolism Review BDocument18 pagesDivine Intervention Episode 15 Metabolism Review BSwisskelly1No ratings yet
- Divine Intervention Episode 6 20 Pharmacology CasesDocument21 pagesDivine Intervention Episode 6 20 Pharmacology CasesSwisskelly1No ratings yet
- Divine Intervention Episode 7 Viral Cases C2ffungal CasesDocument17 pagesDivine Intervention Episode 7 Viral Cases C2ffungal CasesSwisskelly1No ratings yet
- Divine Intervention Episode 19 Neurology Shelf Review Part 1Document16 pagesDivine Intervention Episode 19 Neurology Shelf Review Part 1Swisskelly1No ratings yet
- Divine Intervention Episode 87 USMLE Step 1 Neuro ReviewDocument7 pagesDivine Intervention Episode 87 USMLE Step 1 Neuro ReviewSwisskelly1No ratings yet
- Divine Intervention Episode 83 Heme-Onc ReviewDocument7 pagesDivine Intervention Episode 83 Heme-Onc ReviewSwisskelly1No ratings yet
- Medicine Keywords BDocument142 pagesMedicine Keywords BSwisskelly1No ratings yet
- Divine Intervention Episode 43 The Hy Medical StudentDocument25 pagesDivine Intervention Episode 43 The Hy Medical StudentSwisskelly1No ratings yet
- Divine Intervention Episode 44 Usmle Anatomy Series Part 1Document11 pagesDivine Intervention Episode 44 Usmle Anatomy Series Part 1Swisskelly1No ratings yet
- Divine Intervention Episode 46 Neurology Shelf Review Part 3Document11 pagesDivine Intervention Episode 46 Neurology Shelf Review Part 3Swisskelly1No ratings yet
- Divine Intervention Episode 44 Usmle Anatomy Series Part 1Document11 pagesDivine Intervention Episode 44 Usmle Anatomy Series Part 1Swisskelly1No ratings yet
- Divine Intervention Episode 69 Usmle Anatomy Series Part 2Document9 pagesDivine Intervention Episode 69 Usmle Anatomy Series Part 2Swisskelly1No ratings yet
- Divine Intervention Episode 19 Neurology Shelf Review Part 1Document16 pagesDivine Intervention Episode 19 Neurology Shelf Review Part 1Swisskelly1No ratings yet
- Divine Intervention Episode 7 Viral Cases C2ffungal CasesDocument17 pagesDivine Intervention Episode 7 Viral Cases C2ffungal CasesSwisskelly1No ratings yet
- Med KeywordsDocument67 pagesMed KeywordsSwisskelly1No ratings yet
- Divine Intervention Episode 15 Metabolism Review BDocument18 pagesDivine Intervention Episode 15 Metabolism Review BSwisskelly1No ratings yet
- Divine Intervention Episode 46 Neurology Shelf Review Part 3Document11 pagesDivine Intervention Episode 46 Neurology Shelf Review Part 3Swisskelly1No ratings yet
- Divine Intervention Episode 3 Viral Cases BDocument11 pagesDivine Intervention Episode 3 Viral Cases BSwisskelly1No ratings yet
- The DrunktionaryDocument239 pagesThe DrunktionaryRed Rex 2015No ratings yet
- Sohail KhanDocument3 pagesSohail KhanRashid Muhammad SarwarNo ratings yet
- Calculation of shell and dish thicknessDocument2 pagesCalculation of shell and dish thicknessThiru AnanthNo ratings yet
- MANUAL Health O Meter Scale 800KLDocument2 pagesMANUAL Health O Meter Scale 800KLElkin MaldonadoNo ratings yet
- Carbon Steel Alloys Steel, Pipe Dimension With Weight Test Pressures According To ANSI B36, 10 For ASTM A53/A 106/API 5L/A335/ SpecificationDocument6 pagesCarbon Steel Alloys Steel, Pipe Dimension With Weight Test Pressures According To ANSI B36, 10 For ASTM A53/A 106/API 5L/A335/ SpecificationsanjibkrjanaNo ratings yet
- Humiseal Thinner 73 MSDSDocument3 pagesHumiseal Thinner 73 MSDSibnu Groho Herry sampurnoNo ratings yet
- WILLIEEMS TIBLANI - NURS10 Student Copy Module 15 Part1Document32 pagesWILLIEEMS TIBLANI - NURS10 Student Copy Module 15 Part1Toyour EternityNo ratings yet
- Frontline ArticleDocument7 pagesFrontline Articleapi-548946265No ratings yet
- Observations of Children's Interactions With Teachers, PeersDocument25 pagesObservations of Children's Interactions With Teachers, PeersMazlinaNo ratings yet
- Catalogue of DDSY23S Energy Meter: Smart Metering and System Solution ProviderDocument2 pagesCatalogue of DDSY23S Energy Meter: Smart Metering and System Solution ProviderNadine MichaelsNo ratings yet
- ImpetigoDocument31 pagesImpetigoUmmu Insyirah100% (1)
- Advantest R3131 Spectrum Analyzer Operator ManualDocument277 pagesAdvantest R3131 Spectrum Analyzer Operator ManualMartin Argay100% (1)
- F6003 5W40 Synthetic Oil Technical Data SheetDocument1 pageF6003 5W40 Synthetic Oil Technical Data SheetValeriy ValkovetsNo ratings yet
- Quality and Functionality of Excipients-Art (Alumnos-S) PDFDocument14 pagesQuality and Functionality of Excipients-Art (Alumnos-S) PDFLaura PerezNo ratings yet
- Medray Letterhead TemplateDocument5 pagesMedray Letterhead TemplateSteve NjugiNo ratings yet
- AP000100 EngDocument9 pagesAP000100 EngLucas WrightNo ratings yet
- Deped Memo No. 165, S 2010: WastedDocument6 pagesDeped Memo No. 165, S 2010: WastedJayne InoferioNo ratings yet
- NTTM632 Anand Informatica-ETL Lead ResumeDocument8 pagesNTTM632 Anand Informatica-ETL Lead ResumeMohammed JawadNo ratings yet
- Champagne Making Process: Benjamin CochainDocument13 pagesChampagne Making Process: Benjamin CochainSrikanth ReddyNo ratings yet
- The Payment of Bonus Act 1965 PDFDocument30 pagesThe Payment of Bonus Act 1965 PDFappu kunda100% (1)
- A-Plus Beyond Critical Shield & A-Plus Beyond Early Critical ShieldDocument21 pagesA-Plus Beyond Critical Shield & A-Plus Beyond Early Critical ShieldGenevieve KohNo ratings yet