You might also like
- NEET ANATOMY One LinersDocument6 pagesNEET ANATOMY One LinersKirthikaRaghuraman100% (1)
- Science Class 8 Topic: Respiration and Circulation Reinforcement WorksheetDocument7 pagesScience Class 8 Topic: Respiration and Circulation Reinforcement WorksheetNuzhat Ibrahim100% (1)
- Cell Organelles WorksheetDocument8 pagesCell Organelles WorksheetJohn OsborneNo ratings yet
- 7 Adverse Reactions To TransfusionDocument8 pages7 Adverse Reactions To Transfusioncryztelle2720027476No ratings yet
- 7 Adverse Reactions ToDocument7 pages7 Adverse Reactions ToambadepravinNo ratings yet
- Adverse Effects of Blood TransfusionDocument3 pagesAdverse Effects of Blood TransfusionJosh ViosNo ratings yet
- Immediate Hemolytic Transfusion ReactionDocument2 pagesImmediate Hemolytic Transfusion ReactionleoNo ratings yet
- Dr. P.Karpagam Kiruba Rajeswari, M.B B.S, D.C.P., Blood Bank Medical Officer, MapimsDocument43 pagesDr. P.Karpagam Kiruba Rajeswari, M.B B.S, D.C.P., Blood Bank Medical Officer, MapimsKripa VijayNo ratings yet
- TENCHAVEZ, Duke Harvey - Assignment #2Document5 pagesTENCHAVEZ, Duke Harvey - Assignment #2Duke Harvey TenchavezNo ratings yet
- Transfusion ReactionsDocument2 pagesTransfusion ReactionsSamaahath ArifNo ratings yet
- Transfusion ReactionDocument6 pagesTransfusion ReactionHiraya ManawariNo ratings yet
- Transfusion Reactions: Within 24 Hours of TransfusionDocument6 pagesTransfusion Reactions: Within 24 Hours of TransfusionClaudette Jane SoNo ratings yet
- Hemolytic Anemia IIDocument18 pagesHemolytic Anemia IIArif MaulanaNo ratings yet
- Transfusion Reaction, Hemolytic: Basic InformationDocument3 pagesTransfusion Reaction, Hemolytic: Basic InformationEnrique Hernandez MartinezNo ratings yet
- HaematologyDocument62 pagesHaematologyManmeet SNo ratings yet
- Paroxysmal Cold Hemoglobinuria: Donath-Landstiener Screening TestDocument1 pageParoxysmal Cold Hemoglobinuria: Donath-Landstiener Screening TestMichelle San Miguel FeguroNo ratings yet
- Responsibilities of Nurse, Physician and Medical Technologies Nurse PhysicianDocument9 pagesResponsibilities of Nurse, Physician and Medical Technologies Nurse PhysicianJuan UmiwasNo ratings yet
- Adverse Reactions To Blood Transfusion1Document38 pagesAdverse Reactions To Blood Transfusion1Abby Liew100% (1)
- RLE - WK1 - Manarang, Kyla Mae SDocument1 pageRLE - WK1 - Manarang, Kyla Mae SKyla ManarangNo ratings yet
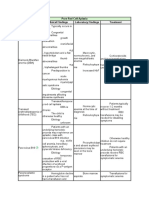
- Pure Red Cell Aplasia Cause Clinical Findings Laboratory Findings TreatmentDocument2 pagesPure Red Cell Aplasia Cause Clinical Findings Laboratory Findings TreatmentRushi ShahNo ratings yet
- BB Quick NotesDocument2 pagesBB Quick Notesrcnwzjk8r4No ratings yet
- Transfusion Hemolytic PDFDocument13 pagesTransfusion Hemolytic PDFMr. LNo ratings yet
- Pama - Joao Artemio Lorenzo PATHOLOGY LABORATORY CORRELATE ACTIVITY NO. 2Document5 pagesPama - Joao Artemio Lorenzo PATHOLOGY LABORATORY CORRELATE ACTIVITY NO. 2Enzo PamaNo ratings yet
- RJDocument2 pagesRJRj King AstreroNo ratings yet
- Aspekmimunologi - Transfusi Darah, 2014Document44 pagesAspekmimunologi - Transfusi Darah, 2014nellyNo ratings yet
- Clinpath-03b & 3c.-Leukocytic-DisordersDocument11 pagesClinpath-03b & 3c.-Leukocytic-DisordersCharisse Angelica MacedaNo ratings yet
- Abo DiscrepanciesDocument2 pagesAbo DiscrepanciesodysseypaulsilorioNo ratings yet
- Loki CH 1972Document4 pagesLoki CH 1972karemiaNo ratings yet
- Trisha Anne Real BSN 2-YB-8 Ncma219 Rle: Laboratory Course Task 1Document2 pagesTrisha Anne Real BSN 2-YB-8 Ncma219 Rle: Laboratory Course Task 1AnneNo ratings yet
- Blood Transfusion Notes..Document9 pagesBlood Transfusion Notes..queenethNo ratings yet
- Hemolytic Disease Newborn PDFDocument6 pagesHemolytic Disease Newborn PDFlokita_opdNo ratings yet
- App B Fact Sheet 0812 FinalDocument12 pagesApp B Fact Sheet 0812 FinalbeautifulbeastNo ratings yet
- Study Stack - MLT Table ReviewDocument3 pagesStudy Stack - MLT Table Review장주연No ratings yet
- Adverse Blood Reaction and HDNDocument34 pagesAdverse Blood Reaction and HDNAdeniran CharlesNo ratings yet
- Blood Groups and Blood TransfusionDocument18 pagesBlood Groups and Blood TransfusionAbdul HafeezNo ratings yet
- Acquired Hemolytic AnemiaDocument48 pagesAcquired Hemolytic AnemiaJeena RajNo ratings yet
- Hemolytic Disease of Newborn Class NotesDocument37 pagesHemolytic Disease of Newborn Class NotesElvisNo ratings yet
- Adverse Effects of TransfusionDocument5 pagesAdverse Effects of Transfusionlubna aloshibiNo ratings yet
- Adverse Effects of TransfusionDocument5 pagesAdverse Effects of Transfusionlubna aloshibiNo ratings yet
- Sepsis DoneDocument54 pagesSepsis DoneGiorgi PopiashviliNo ratings yet
- Anemia Hemolitik AutoimunDocument16 pagesAnemia Hemolitik AutoimunAnonymous lVfqKMlyXNo ratings yet
- DownloadDocument3 pagesDownloadbesttiktokfindsshopNo ratings yet
- Hemolytic Anemias: Common Findings in AllDocument4 pagesHemolytic Anemias: Common Findings in AllSamah KhanNo ratings yet
- Blood Transfusion - ClinconDocument22 pagesBlood Transfusion - ClinconRisah Mae SarinoNo ratings yet
- Antibiotic Hypersensitivity MechanismsDocument14 pagesAntibiotic Hypersensitivity Mechanismsrochmandrg dokter gigiNo ratings yet
- Maternal 2 - Blood TransfusionDocument5 pagesMaternal 2 - Blood TransfusionJuliana Anne RamosNo ratings yet
- Pathology SGD 4: Diseases-Of-The-Immune-System: Group-4Document23 pagesPathology SGD 4: Diseases-Of-The-Immune-System: Group-4Kalpana JenaNo ratings yet
- Probleme La TransfuziiDocument6 pagesProbleme La TransfuziiAdina TîrnoveanuNo ratings yet
- 74 Year Old Woman With Fatigue, Anorexia, and AbdoDocument6 pages74 Year Old Woman With Fatigue, Anorexia, and AbdoRamiro Arraya MierNo ratings yet
- Hazard and Management of Blood TransfusionDocument60 pagesHazard and Management of Blood TransfusionRejwanur Rahman MirazNo ratings yet
- Laboratory and Diagnostic ResultsDocument9 pagesLaboratory and Diagnostic ResultsHaru DogNo ratings yet
- Benign Disoders of WBCsDocument40 pagesBenign Disoders of WBCsaliabumrfghNo ratings yet
- Rotation5 SIC LarceñaDocument10 pagesRotation5 SIC LarceñanoemilauNo ratings yet
- Platelet Transfusion Refractoriness How Do IDocument6 pagesPlatelet Transfusion Refractoriness How Do IJuan Manuel Cano CalderónNo ratings yet
- 3讲义hematologyDocument96 pages3讲义hematologychongyu888xiongNo ratings yet
- Complete Blood CountDocument5 pagesComplete Blood CountShella CondezNo ratings yet
- ASH Guidlines On Platelet RefractorinessDocument6 pagesASH Guidlines On Platelet RefractorinessM Asif NaveedNo ratings yet
- Heamatology 3Document7 pagesHeamatology 3mcpaulfreemanNo ratings yet
- Reporte de Caso EmbaraoDocument3 pagesReporte de Caso EmbaraoPaola TabaresNo ratings yet
- Textbook of Clinical Paediatrics.Document1 pageTextbook of Clinical Paediatrics.عبد الله عبد اللهNo ratings yet
- Blood Grouping 1690574753Document30 pagesBlood Grouping 1690574753willowmaecayabyabNo ratings yet
- Blood Transfusion ReactionsDocument8 pagesBlood Transfusion ReactionsStephanie AngelaNo ratings yet
- Prenatal Diagnosis of Four-Vessel Umbilical Cord With Supernumerary Vein Varix - A Case Report and Literature ReviewDocument5 pagesPrenatal Diagnosis of Four-Vessel Umbilical Cord With Supernumerary Vein Varix - A Case Report and Literature ReviewMina zhouNo ratings yet
- Malignant Ovarian TumourDocument42 pagesMalignant Ovarian TumourJones MarinaNo ratings yet
- Benign Gestational Trophoblastic DiseaseDocument31 pagesBenign Gestational Trophoblastic Diseaseبسيل أبوهلالNo ratings yet
- Cysts of The Oral Cavity-3Document33 pagesCysts of The Oral Cavity-3Mostafa El GendyNo ratings yet
- Anatomy and Embryology of The Pharynx1.ppsDocument27 pagesAnatomy and Embryology of The Pharynx1.ppsНемосјановић ЋудмилаNo ratings yet
- ArchegoniateplantDocument21 pagesArchegoniateplantShubhamMalikNo ratings yet
- The A To Z of Peripheral NervesDocument230 pagesThe A To Z of Peripheral NervesAspenPharma95% (19)
- 4 Stages of Speech ProductionDocument3 pages4 Stages of Speech ProductionEve RulonaNo ratings yet
- Bleeding DisordersDocument4 pagesBleeding DisordersRitz CelsoNo ratings yet
- 2 NDLPDocument14 pages2 NDLPJennifer Lopez Guiao-Catacutan0% (1)
- Biota Quiz Bee Mock Test Part 1Document2 pagesBiota Quiz Bee Mock Test Part 1Ken Juliana Fe IsaacNo ratings yet
- Homeostasis Concept MapDocument1 pageHomeostasis Concept MapMarjorie RonquilloNo ratings yet
- WOAg B7 My 1 HJmy GGN EYOFDocument41 pagesWOAg B7 My 1 HJmy GGN EYOFandrewmanshionNo ratings yet
- Weight Training: Abs, Legs & Butt: Firm Up From The Waist DownDocument6 pagesWeight Training: Abs, Legs & Butt: Firm Up From The Waist Downbloom manelNo ratings yet
- GENBIO1 HandoutDocument2 pagesGENBIO1 HandoutZaza May VelascoSbNo ratings yet
- Local Media5289763584533511516Document8 pagesLocal Media5289763584533511516Haniya KhanNo ratings yet
- Class 5 Science Classwork 091020Document3 pagesClass 5 Science Classwork 091020Rakesh AgarwalNo ratings yet
- DIPASREE - ROYCHOWDHURYAnomalous Secondary Growth in Boerhaavia Stem2020!04!03Anomalous Secondary Growth in Boerhaavia StemDocument2 pagesDIPASREE - ROYCHOWDHURYAnomalous Secondary Growth in Boerhaavia Stem2020!04!03Anomalous Secondary Growth in Boerhaavia StemAkshay KannanNo ratings yet
- Digestive System: Unit IiDocument130 pagesDigestive System: Unit IiPRIYAM NET CENTER100% (1)
- The Inferior Olivary Nucleus of The Rat A Light and Electron Microscopic StudyDocument31 pagesThe Inferior Olivary Nucleus of The Rat A Light and Electron Microscopic StudyRafael GutierrezNo ratings yet
- Cytochemistry PrimerDocument2 pagesCytochemistry PrimerMunish Dogra100% (1)
- Erogenous Zones: Solitary BehaviorDocument7 pagesErogenous Zones: Solitary BehaviorMuzically InspiredNo ratings yet
- ImmunoglobulinDocument39 pagesImmunoglobulinReguird AllaeinniNo ratings yet
- Martini FAP7 ch1Document41 pagesMartini FAP7 ch1Muhammad Na'imNo ratings yet
- Case Pre DHFDocument15 pagesCase Pre DHFJeLai Lozano AbeciaNo ratings yet
- Physical Exam Vital SignsDocument4 pagesPhysical Exam Vital SignsmickeyNo ratings yet
- Mcq Exams Ent 3rd Edition الهيئة السعوديةDocument162 pagesMcq Exams Ent 3rd Edition الهيئة السعوديةHamada Hassan Alloq100% (1)