You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Cardiology: C B: A V L U: J 2019Document20 pagesCardiology: C B: A V L U: J 2019Owen AgnewNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- ExaminationofpulseDocument6 pagesExaminationofpulsePeter Paul GollamudiNo ratings yet
- Essential Basics of General Medicine Faculty of Dentistry Cairo UniversityDocument104 pagesEssential Basics of General Medicine Faculty of Dentistry Cairo Universitybavly waidyNo ratings yet
- JVP Measured at 3 CM Above The Sternal Angle, or 8 CM Above The Right Atrium, Is Considered Elevated or AbnormalDocument11 pagesJVP Measured at 3 CM Above The Sternal Angle, or 8 CM Above The Right Atrium, Is Considered Elevated or AbnormalRubie Ann TillorNo ratings yet
- Approach To DyspneaDocument9 pagesApproach To DyspneaMuhammad LukmanNo ratings yet
- Chest DiscomfortsDocument37 pagesChest DiscomfortsMUKESH SUNDARARAJANNo ratings yet
- Word Association PANCEDocument31 pagesWord Association PANCEnevmerka100% (1)
- Chestpain 150320061131 Conversion Gate01Document36 pagesChestpain 150320061131 Conversion Gate01Aisha AldosreyNo ratings yet
- ACC Jimmy AsafDocument152 pagesACC Jimmy AsafFikriYTNo ratings yet
- PANCE Word Associations PDFDocument27 pagesPANCE Word Associations PDFkatNo ratings yet
- Cardiology Plabable PDFDocument22 pagesCardiology Plabable PDFTirtha Taposh100% (1)
- Chest Pain - Investigation, Diagnosis and TreatmentDocument5 pagesChest Pain - Investigation, Diagnosis and Treatmentsoumabho paruiNo ratings yet
- Chapter 14 - Chest DiscomfortDocument15 pagesChapter 14 - Chest DiscomforthectorNo ratings yet
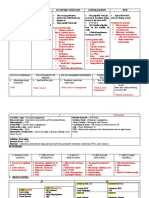
- 2.Dyspneu-Is It Pulmonary or Extrapulmonary Problem - Anna UyainahDocument24 pages2.Dyspneu-Is It Pulmonary or Extrapulmonary Problem - Anna UyainahmaryamNo ratings yet
- Sindromatologi DyspneuDocument18 pagesSindromatologi DyspneuMeylan TaebenuNo ratings yet
- Chest Pain Investigation Diagnosis and TreatmentDocument4 pagesChest Pain Investigation Diagnosis and TreatmentHadsabsaNo ratings yet
- Cvs - Clinical NotesDocument38 pagesCvs - Clinical NotessekaralingamNo ratings yet
- In The Name of ALLAH, The Most Beneficent, The Most Gracious, The Most Merciful !Document24 pagesIn The Name of ALLAH, The Most Beneficent, The Most Gracious, The Most Merciful !Wan HafizNo ratings yet
- 1 Chest PainDocument6 pages1 Chest Painnathanaellee92No ratings yet
- 5 Pericarditis and Its Complications ICMPDDocument22 pages5 Pericarditis and Its Complications ICMPDmus zaharaNo ratings yet
- Mumurs Summary PDFDocument6 pagesMumurs Summary PDFykteo323No ratings yet
- Acute Coronary SyndromeDocument8 pagesAcute Coronary Syndromerazan.girl.2010No ratings yet
- Cardiology HX - PEDocument34 pagesCardiology HX - PEjjNo ratings yet
- CVS Examination 2Document70 pagesCVS Examination 2TanveerHajiIqbalNo ratings yet
- Internal Medicine NotesDocument54 pagesInternal Medicine NotesKiara Govender100% (1)
- IIA - Altered Tissue PerfusionDocument14 pagesIIA - Altered Tissue PerfusionDharylle CariñoNo ratings yet
- Syncope E:Manag Afp (Dragged) 3Document1 pageSyncope E:Manag Afp (Dragged) 3M.DalaniNo ratings yet
- Approach To Chest PainDocument36 pagesApproach To Chest PainAbhay KumarNo ratings yet
- Supan-Clinical Case AnalysisDocument7 pagesSupan-Clinical Case AnalysisAjay SupanNo ratings yet
- PericarditisDocument120 pagesPericarditis18sn02nr059No ratings yet
- Mitral StenosisDocument2 pagesMitral StenosisitsmailbbkNo ratings yet
- Cardiac, Lungs, Pvs AssessmentDocument59 pagesCardiac, Lungs, Pvs AssessmentankurNo ratings yet
- Chest Pain: SV Hoàng Khương Duy Y2014dDocument32 pagesChest Pain: SV Hoàng Khương Duy Y2014dDavid WilliamNo ratings yet
- Problem Based Learning Cardiovascular System: 2nd GroupDocument47 pagesProblem Based Learning Cardiovascular System: 2nd GroupClaudia Narinda R. PNo ratings yet
- Drug Study AbulenciaaaDocument3 pagesDrug Study AbulenciaaaKsksksksNo ratings yet
- Tuberculous Pericardial EffusionDocument6 pagesTuberculous Pericardial EffusionLink BuiNo ratings yet
- Acut Heart FailureDocument20 pagesAcut Heart FailureCatherine MorrisNo ratings yet
- 4.cardivascular System ExaminationDocument60 pages4.cardivascular System ExaminationElvisNo ratings yet
- REVIEWER2Document6 pagesREVIEWER2Lorielyn Ashlee GaiteNo ratings yet
- Pembekalan Anamnesa Dan Pemeriksaan Fisik KardiologiDocument64 pagesPembekalan Anamnesa Dan Pemeriksaan Fisik KardiologiMirza Thaariq HapsitoNo ratings yet
- Sign and Symptom CardiovascularDocument26 pagesSign and Symptom CardiovascularDanang MustofaNo ratings yet
- Toronto Notes Respirology PDFDocument40 pagesToronto Notes Respirology PDFJaya Semara Putra67% (3)
- Cardiovascular SystemDocument205 pagesCardiovascular Systemizuku midoriyaNo ratings yet
- Internal Medicine NotesDocument54 pagesInternal Medicine NotesHayley Welsh75% (4)
- WK1 - Inflammatory Heart Failure Infectious DiseaseDocument4 pagesWK1 - Inflammatory Heart Failure Infectious DiseaseJhaji Mei Margarete CasiNo ratings yet
- Parameter 0 1 2 Activity Pulse GrimaceDocument2 pagesParameter 0 1 2 Activity Pulse GrimaceAnna BartolomeNo ratings yet
- Cardiovascular Disorders 2Document78 pagesCardiovascular Disorders 2Erlinda SagadsadNo ratings yet
- Introduction and Definition: Patients Use T Ms F Brea Le NeDocument10 pagesIntroduction and Definition: Patients Use T Ms F Brea Le NeAckNo ratings yet
- Management of Cardiovascular Emergency CaseDocument49 pagesManagement of Cardiovascular Emergency Caseesti.pujiastuti0107No ratings yet
- CVS and RespiratoryDocument29 pagesCVS and RespiratorysaifNo ratings yet
- MI SlidesDocument65 pagesMI SlidesJobelyn TunayNo ratings yet
- Hi-Yield Notes in Im & PediaDocument20 pagesHi-Yield Notes in Im & PediaJohn Christopher LucesNo ratings yet
- By: DR - Wesam AbdelazizDocument48 pagesBy: DR - Wesam AbdelazizTIRTH GANATRANo ratings yet
- Cardiac Sheet: Personal HistoryDocument7 pagesCardiac Sheet: Personal HistorySyximsh FPNo ratings yet
- Scenario NCPDocument3 pagesScenario NCPZanie CruzNo ratings yet
- SyncopeDocument6 pagesSyncopeIsmail Ali إسماعيل عليNo ratings yet
- Drug Study For Nsy DRDocument4 pagesDrug Study For Nsy DRLiza M. PurocNo ratings yet
- Kelompok 14 Skenario 2Document11 pagesKelompok 14 Skenario 2Rachmad SammuliaNo ratings yet
- AllergicDocument18 pagesAllergicChethranNo ratings yet
- Temporary - BbbhbRegistration - Non Schedule 7A FTPDocument8 pagesTemporary - BbbhbRegistration - Non Schedule 7A FTPChethranNo ratings yet
- 01 Integration of Primary Care and Oh ServicesDocument5 pages01 Integration of Primary Care and Oh ServicesChethranNo ratings yet
- SS Plastic - General Principles (2014)Document11 pagesSS Plastic - General Principles (2014)ChethranNo ratings yet
- New Doc 2019-10-23 15.15.15 - 20191023151531Document1 pageNew Doc 2019-10-23 15.15.15 - 20191023151531ChethranNo ratings yet
- Radiology Finals Pointers As Noted by Samira VDocument3 pagesRadiology Finals Pointers As Noted by Samira VChethranNo ratings yet
- New Doc 2019-10-23 15.16.57 - 20191023151720Document1 pageNew Doc 2019-10-23 15.16.57 - 20191023151720ChethranNo ratings yet
- A GYNE PrelimsuyguvuybDocument3 pagesA GYNE PrelimsuyguvuybChethranNo ratings yet
- Definitions:: Impotence Here Means Incapable of Having Sexual RelationDocument2 pagesDefinitions:: Impotence Here Means Incapable of Having Sexual RelationChethranNo ratings yet
- Answer: FDocument8 pagesAnswer: FChethranNo ratings yet
- Rvrtv5tgt5Abnormal Uterine BleedingDocument4 pagesRvrtv5tgt5Abnormal Uterine BleedingChethranNo ratings yet
- Rvrtv5tgt5Abnormal Uterine BleedingDocument4 pagesRvrtv5tgt5Abnormal Uterine BleedingChethranNo ratings yet
- Optha Midterm: Saturday, May 16, 2015 10:59 PMDocument7 pagesOptha Midterm: Saturday, May 16, 2015 10:59 PMChethranNo ratings yet
- BREECH 2nijnjinijnuihiuhDocument7 pagesBREECH 2nijnjinijnuihiuhChethranNo ratings yet
- Differential Diagnosis: Adenocarcinoma of Colon FOBT Positive Black Stool May Be Metastasis Has Gone To Form Liver AbcessDocument3 pagesDifferential Diagnosis: Adenocarcinoma of Colon FOBT Positive Black Stool May Be Metastasis Has Gone To Form Liver AbcessChethranNo ratings yet
- Chapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFDocument9 pagesChapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFChethranNo ratings yet
- Sunuohouhouhafari - 28 Feb 2019 at 11:19 Ouh0uhhDocument1 pageSunuohouhouhafari - 28 Feb 2019 at 11:19 Ouh0uhhChethranNo ratings yet
- Traumassee 2 Notes - 20171202083816850Document14 pagesTraumassee 2 Notes - 20171202083816850ChethranNo ratings yet
- Bakdjdjedjnk Receipt - 20180910223833350Document2 pagesBakdjdjedjnk Receipt - 20180910223833350ChethranNo ratings yet
- My Note (2) BB Gubtuvuvt7Document19 pagesMy Note (2) BB Gubtuvuvt7ChethranNo ratings yet
- Radiology in UrologyDocument39 pagesRadiology in UrologyUgan SinghNo ratings yet
- Miami Youth Football League Registration FormDocument1 pageMiami Youth Football League Registration FormMarley-Kojak CookNo ratings yet
- Maternal ReviewerDocument15 pagesMaternal ReviewerIvy DG100% (2)
- Isosorbide DinitrateDocument1 pageIsosorbide Dinitrate202110439No ratings yet
- Text CDocument1,100 pagesText CAli NofalNo ratings yet
- MS Wrep IIDocument51 pagesMS Wrep IIiana-almocera-6970No ratings yet
- Smart Facilities: Responding To 21st Century Challenges and Technological InnovationsDocument31 pagesSmart Facilities: Responding To 21st Century Challenges and Technological InnovationsADB Health Sector GroupNo ratings yet
- Patient Required Forms - Pasadena Cyberknife CenterDocument11 pagesPatient Required Forms - Pasadena Cyberknife CenterPasadena Cyberknife Center100% (1)
- Apollo Hospital Press Release 5 02 Sept 14Document2 pagesApollo Hospital Press Release 5 02 Sept 14LUKAZA2013No ratings yet
- AA Effectiveness - Faith Meets ScienceDocument68 pagesAA Effectiveness - Faith Meets SciencejgogekNo ratings yet
- 2007 Tweed ProfileDocument60 pages2007 Tweed ProfileYeny Valdivia AlbornozNo ratings yet
- Spurious Electrolyte Disorders: A Diagnostic Challenge For CliniciansDocument8 pagesSpurious Electrolyte Disorders: A Diagnostic Challenge For CliniciansWiwid SantikoNo ratings yet
- Lung - Cancer - Case - 1 of 80Document4 pagesLung - Cancer - Case - 1 of 80Mavra zNo ratings yet
- Daily Patient Assignment SheetDocument1 pageDaily Patient Assignment SheetSheferely BayauaNo ratings yet
- Skripsi Full Tanpa Bab PembahasanDocument53 pagesSkripsi Full Tanpa Bab Pembahasanfani akifaazriNo ratings yet
- APA - DSM5 - Severity Measure For Specific Phobia Adult PDFDocument3 pagesAPA - DSM5 - Severity Measure For Specific Phobia Adult PDFaasdfjlkNo ratings yet
- Euthanasia ThesisDocument11 pagesEuthanasia ThesisAyush MathurNo ratings yet
- Lesson 14 - Individual TaskDocument2 pagesLesson 14 - Individual TaskChristine CondrillonNo ratings yet
- Hyperemesis GravidarumDocument5 pagesHyperemesis GravidarumGladys Ocampo100% (5)
- Ashrae 170 2013 UpdateDocument75 pagesAshrae 170 2013 UpdateAhmed AbdelzaherNo ratings yet
- How to look 「皮疹」Document50 pagesHow to look 「皮疹」Satoshi KobayashiNo ratings yet
- UntitledDocument7 pagesUntitledGulfam ZamiNo ratings yet
- Typhoid 21Document9 pagesTyphoid 21Nanda Hikma LestariNo ratings yet
- Coding Notes - Billing & Coding Pocket GuideDocument238 pagesCoding Notes - Billing & Coding Pocket Guidealihadibaqir83% (6)
- HaadDocument13 pagesHaadMac FelicianoNo ratings yet
- CCJM HyperhidrosisDocument3 pagesCCJM HyperhidrosisBrian HarrisNo ratings yet
- BM Narrative Report - Medical Services IncDocument35 pagesBM Narrative Report - Medical Services Incjvb_buena2734No ratings yet
- Disorders of Acid Base BalanceDocument1 pageDisorders of Acid Base BalanceLyn Domingo EllaquezNo ratings yet
- AABB Red Blood Cell Transfusion Guidelines Something For Almost EveryoneDocument2 pagesAABB Red Blood Cell Transfusion Guidelines Something For Almost EveryonewilzmaxNo ratings yet
- Handout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisDocument2 pagesHandout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisValentina IerotheouNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainFrom EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainRating: 4 out of 5 stars4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (59)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)