You might also like
- Endocrine PathologyDocument13 pagesEndocrine Pathologysarguss14100% (1)
- EndoDocument8 pagesEndoSheryl Layne Lao-SebrioNo ratings yet
- Pathology Tests ExplainedDocument4 pagesPathology Tests ExplainedFabiola Fuentes RomeroNo ratings yet
- Feedback Mechanism: Positive FeedbackDocument17 pagesFeedback Mechanism: Positive FeedbackJanielle Medina FajardoNo ratings yet
- Endocrinology 2016Document52 pagesEndocrinology 2016Aman Singh RaoNo ratings yet
- EndocrinologyDocument39 pagesEndocrinologyJanelle RemorozaNo ratings yet
- Chapter 35 - Hypothalamic and Pituitary AgentsDocument4 pagesChapter 35 - Hypothalamic and Pituitary Agentskdayeon018No ratings yet
- Endo Pituitary ElhDocument24 pagesEndo Pituitary Elhodiodi57No ratings yet
- Anatomy and PhysiologyDocument14 pagesAnatomy and PhysiologyIssaiah Nicolle CeciliaNo ratings yet
- Dr. Raghu Prasada M S MBBS, MD Assistant Professor Dept. of Pharmacology Ssims & RCDocument27 pagesDr. Raghu Prasada M S MBBS, MD Assistant Professor Dept. of Pharmacology Ssims & RCNastase Daniela EcaterinaNo ratings yet
- Hormonii Axei Reproductive Andra CaragheorgheopolDocument70 pagesHormonii Axei Reproductive Andra CaragheorgheopolMadalina PavelNo ratings yet
- Poros Hpo Dalam Regulasi Sistem Reproduksi WanitaDocument49 pagesPoros Hpo Dalam Regulasi Sistem Reproduksi WanitaKzia YlujkNo ratings yet
- 10 - Hormonal AgentsDocument64 pages10 - Hormonal Agentsnica velanoNo ratings yet
- ENDOCRINE DISORDERS Ms HandoutsDocument14 pagesENDOCRINE DISORDERS Ms HandoutsCatherine FaithNo ratings yet
- HY EndocrineoeDocument62 pagesHY EndocrineoebrownsmilansNo ratings yet
- HY EndocrineDocument61 pagesHY EndocrineKiranNo ratings yet
- Endocrinology Pharmacology: Hormone Agonists, Antagonists & ModulatorsDocument151 pagesEndocrinology Pharmacology: Hormone Agonists, Antagonists & Modulatorsj.doe.hex_87100% (1)
- Endocrine Gland Hormone(s) Secreted Stimulus Effect of Hormone Inhibition PathologyDocument3 pagesEndocrine Gland Hormone(s) Secreted Stimulus Effect of Hormone Inhibition PathologySamuelNo ratings yet
- Pituitary Disorders (Final Draft)Document17 pagesPituitary Disorders (Final Draft)Kiprono Keitany TimothyNo ratings yet
- Science Reviewer LT1 - Q4Document2 pagesScience Reviewer LT1 - Q4Cara IsabelNo ratings yet
- Hypothalamic & Pituitary SHORTDocument9 pagesHypothalamic & Pituitary SHORTa.muhsinNo ratings yet
- Endocrine Day 1 TemplateDocument17 pagesEndocrine Day 1 TemplateMikeNo ratings yet
- Pituitary and Hypothalamic Hormones 2015Document19 pagesPituitary and Hypothalamic Hormones 2015High EducationNo ratings yet
- Clinical ChemistryDocument11 pagesClinical Chemistryangelwithoutwings321No ratings yet
- Hormones Synthesized and Secreted by The Anterior Pituitary and Their EffectsDocument15 pagesHormones Synthesized and Secreted by The Anterior Pituitary and Their EffectsAaron James RuedasNo ratings yet
- Describe Hormones and Their CompositionDocument7 pagesDescribe Hormones and Their CompositionShahzaib AhmedNo ratings yet
- Endocrine PDFDocument5 pagesEndocrine PDFRegina SantosNo ratings yet
- ENDOCRINOLOGYDocument8 pagesENDOCRINOLOGYshaairatogleNo ratings yet
- Diseases of The Pituitary GlandDocument10 pagesDiseases of The Pituitary Glandbalkrishna.narshaiNo ratings yet
- Maher Khdour, PHD: Associate Prof. Faculty of Pharmacy Al-Quds UniversityDocument52 pagesMaher Khdour, PHD: Associate Prof. Faculty of Pharmacy Al-Quds Universityتمارا عكاري.No ratings yet
- Endocrine DrugsDocument172 pagesEndocrine DrugsAlvim Tiel FactorNo ratings yet
- Pharmacology: EndocrineDocument210 pagesPharmacology: EndocrineSharifa Darayan100% (1)
- Anterior Pituitary GlandDocument33 pagesAnterior Pituitary Glandmarianne.erdooNo ratings yet
- Pcol Lec Book FinalsDocument61 pagesPcol Lec Book FinalsMarco Sta AnaNo ratings yet
- Review of Endocrine SystemDocument32 pagesReview of Endocrine SystemJames FNo ratings yet
- Pharmacology Finals ReviewerDocument29 pagesPharmacology Finals ReviewerbrxcygwynthNo ratings yet
- Male ReproductiveDocument10 pagesMale ReproductivevivekNo ratings yet
- Pituitary Gland: Click To Edit Master Subtitle StyleDocument14 pagesPituitary Gland: Click To Edit Master Subtitle StyleSuresh KumarNo ratings yet
- Phys 6.1 and 6.2 Ant Pituitary GH and Post Pituitary NOTESDocument7 pagesPhys 6.1 and 6.2 Ant Pituitary GH and Post Pituitary NOTESsine summsun PradhanNo ratings yet
- Endocrinology: Differences Between Nervous and Endocrine SystemDocument34 pagesEndocrinology: Differences Between Nervous and Endocrine SystemRezaul RazibNo ratings yet
- Coordination and Control Ch#17Document4 pagesCoordination and Control Ch#17Usman GhaniNo ratings yet
- Endocrine System: By: Trixie Rose E. CortezDocument144 pagesEndocrine System: By: Trixie Rose E. CortezTrixie Rose Ebona CortezNo ratings yet
- NCM 116 Case Analysis 2Document9 pagesNCM 116 Case Analysis 2Dominic DegraciaNo ratings yet
- Jardine Jade Albert C. Valdez, RMTDocument48 pagesJardine Jade Albert C. Valdez, RMTEj BersalonaNo ratings yet
- The Endocrine System: Presented By: 5th Group Feby Amalia Hardianty Suryana Syuaib Andi Nurul Virninda Debby Trisia SariDocument24 pagesThe Endocrine System: Presented By: 5th Group Feby Amalia Hardianty Suryana Syuaib Andi Nurul Virninda Debby Trisia SariAndi Nurhidayah100% (1)
- 9 - Toronto Notes 2011 - Endocrinology PDFDocument56 pages9 - Toronto Notes 2011 - Endocrinology PDFLalaNo ratings yet
- Gland: - Types of Glands:: EndocrinologyDocument45 pagesGland: - Types of Glands:: EndocrinologyCec DfNo ratings yet
- Endocrinology ROAMSDocument12 pagesEndocrinology ROAMSvkNo ratings yet
- Endocrine System DrugsDocument66 pagesEndocrine System DrugsRania HamamNo ratings yet
- Endo - TransesDocument8 pagesEndo - TransesMelanie ManuzonNo ratings yet
- ENDODocument141 pagesENDOearldem1996No ratings yet
- MSL Ec MidtermsDocument27 pagesMSL Ec Midtermsmendozajanice0601No ratings yet
- 13 Puberty1Document62 pages13 Puberty1valuevaNo ratings yet
- ENDOCRINE HORMONES and PeriodontiumDocument85 pagesENDOCRINE HORMONES and Periodontiumt sNo ratings yet
- Presentation1 (Mod)Document27 pagesPresentation1 (Mod)kateofeveryone9795No ratings yet
- MTAPDocument19 pagesMTAPCaressa Marie EstradaNo ratings yet
- 1 Endocrinology 1Document14 pages1 Endocrinology 1Jessa MayNo ratings yet
- Hypothalamus Pituitary and Gonad AxisDocument6 pagesHypothalamus Pituitary and Gonad Axisalok nayakNo ratings yet
- Endocrine PhysiologyDocument86 pagesEndocrine PhysiologySabbir AhmedNo ratings yet
- Postmedj00400 0048Document3 pagesPostmedj00400 0048TRIANDINI TRIANDININo ratings yet
- Diagnosis and Treatment of Ovarian Remnant Syndrome PDFDocument10 pagesDiagnosis and Treatment of Ovarian Remnant Syndrome PDFIaSoftNo ratings yet
- Lab 03 - The Integumentary SystemDocument3 pagesLab 03 - The Integumentary SystemRonyel Burias II0% (1)
- Anatomy and Physiology of Reproduction: Female Reproduction Male ReproductionDocument15 pagesAnatomy and Physiology of Reproduction: Female Reproduction Male ReproductionMhiahLine TolentinoNo ratings yet
- Homeostasis 2Document31 pagesHomeostasis 2Khayelihle WakaDingiswayo NtshakalaNo ratings yet
- DLL in Science5Document2 pagesDLL in Science5Elizabeth Santos100% (3)
- Normal Menstrual Cycle The ProcessDocument6 pagesNormal Menstrual Cycle The ProcessBrett StevensonNo ratings yet
- Assessment of HypokalaemiaDocument79 pagesAssessment of HypokalaemiaWildcane SalmeronNo ratings yet
- Test-02 - HR and RHDocument5 pagesTest-02 - HR and RHAkash GargNo ratings yet
- The Effect of Resistance Training On Thyroid HormonesDocument5 pagesThe Effect of Resistance Training On Thyroid Hormonesroyal_rahulNo ratings yet
- حالات سكرDocument13 pagesحالات سكرNada AliNo ratings yet
- Reportpdf1 PDFDocument3 pagesReportpdf1 PDFLifetime AbbeyNo ratings yet
- Anaphy Chapter 10 Endocrine SystemDocument6 pagesAnaphy Chapter 10 Endocrine SystemJohnNo ratings yet
- IfU ATG1010engl, DT, Es-18062014 Ab Lot 016Document23 pagesIfU ATG1010engl, DT, Es-18062014 Ab Lot 016f.baxyNo ratings yet
- Endocrine Physiology Case Study - BathshebaDocument6 pagesEndocrine Physiology Case Study - BathshebaMc Lindssey PascualNo ratings yet
- The BodyDocument4 pagesThe BodySheila G. DolipasNo ratings yet
- Pseudohypoparathyroidism-Literature Update 2018Document8 pagesPseudohypoparathyroidism-Literature Update 2018radu nicolaeNo ratings yet
- Asynchronous Activity Sheet FormsDocument8 pagesAsynchronous Activity Sheet FormsNur SanaaniNo ratings yet
- Diabetis 2Document33 pagesDiabetis 2Fercho MedNo ratings yet
- HypothyroidismDocument7 pagesHypothyroidismavinash dhameriyaNo ratings yet
- Skin ProjectDocument2 pagesSkin Projectapi-237316144No ratings yet
- Scie5 Q2 Mod2 ChangesThatOccurDuringPuberty v3Document17 pagesScie5 Q2 Mod2 ChangesThatOccurDuringPuberty v3DanielMatsunagaNo ratings yet
- Drug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineDocument4 pagesDrug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineEileenAquinoMacapagalNo ratings yet
- Adrenal Function TestDocument26 pagesAdrenal Function TestSaroja Veeresh83% (6)
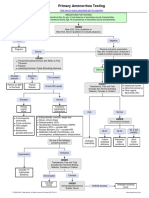
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Thyroid NeoplasmDocument11 pagesThyroid NeoplasmPravin KumarNo ratings yet
- Management of Diabetes Mellitus A ReviewDocument11 pagesManagement of Diabetes Mellitus A ReviewEditor IJTSRDNo ratings yet
- Chemical Coordination and IntegrationDocument6 pagesChemical Coordination and IntegrationpraveenrajnivethaNo ratings yet
- 2 HyperthyroidismDocument3 pages2 HyperthyroidismAisha MarieNo ratings yet
- Diabetes Insipidus Journal ReadingDocument13 pagesDiabetes Insipidus Journal ReadingnadiyasyadinaNo ratings yet