You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Pnle ReviewerDocument293 pagesPnle ReviewerAsniah Hadjiadatu Abdullah94% (18)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MOH DHA HAAD Dental Study Material Part 2Document33 pagesMOH DHA HAAD Dental Study Material Part 2Junaid Ramzan89% (37)
- Health EDUC Teaching Demo RubricsDocument4 pagesHealth EDUC Teaching Demo RubricsAsniah Hadjiadatu Abdullah100% (1)
- Beta Blocker ToxicityDocument15 pagesBeta Blocker ToxicitysmoggindakrakNo ratings yet
- Addiction: A Dysregulation of Satiety and Inflammatory ProcessesDocument27 pagesAddiction: A Dysregulation of Satiety and Inflammatory ProcessesAulas EspañolNo ratings yet
- CV 2023010319584829Document1 pageCV 2023010319584829Asniah Hadjiadatu AbdullahNo ratings yet
- FNCP PoorsanitationmarwahDocument3 pagesFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahNo ratings yet
- Application Forms (Fillable)Document2 pagesApplication Forms (Fillable)Asniah Hadjiadatu AbdullahNo ratings yet
- Credential Verification Form Non-Clinical (Without Signature Page)Document1 pageCredential Verification Form Non-Clinical (Without Signature Page)Asniah Hadjiadatu AbdullahNo ratings yet
- Daniel Saladas ResumeDocument2 pagesDaniel Saladas ResumeAsniah Hadjiadatu AbdullahNo ratings yet
- Poor Compliance With Treatment As Health Threat CuesDocument11 pagesPoor Compliance With Treatment As Health Threat CuesAsniah Hadjiadatu AbdullahNo ratings yet
- To Fill-Up Id-Atm FormDocument7 pagesTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahNo ratings yet
- Nursing Notes Maternal and Child Nursing CareDocument70 pagesNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahNo ratings yet
- Health Teaching Plan FinaleDocument4 pagesHealth Teaching Plan FinaleAsniah Hadjiadatu AbdullahNo ratings yet
- History: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentDocument4 pagesHistory: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentAsniah Hadjiadatu AbdullahNo ratings yet
- Or/Dr/Nicu/Pacu Requirements: Open Wound TypesDocument6 pagesOr/Dr/Nicu/Pacu Requirements: Open Wound TypesAsniah Hadjiadatu AbdullahNo ratings yet
- Family Case Study PresentationDocument1 pageFamily Case Study PresentationAsniah Hadjiadatu AbdullahNo ratings yet
- Poor Environmetal Sanitation As Health Threat CuesDocument11 pagesPoor Environmetal Sanitation As Health Threat CuesAsniah Hadjiadatu AbdullahNo ratings yet
- Mock ResumeDocument3 pagesMock ResumeAsniah Hadjiadatu AbdullahNo ratings yet
- Family Case Study On Pulmonary TuberculosisDocument4 pagesFamily Case Study On Pulmonary TuberculosisAsniah Hadjiadatu AbdullahNo ratings yet
- Family Case StudyDocument33 pagesFamily Case StudyAsniah Hadjiadatu AbdullahNo ratings yet
- Proposed Budget For The 17th Striping and Pinning Investiture CeremonyDocument1 pageProposed Budget For The 17th Striping and Pinning Investiture CeremonyAsniah Hadjiadatu AbdullahNo ratings yet
- Water RescueDocument7 pagesWater RescueAsniah Hadjiadatu AbdullahNo ratings yet
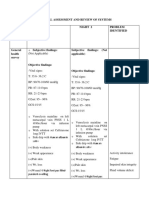
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDocument9 pagesPhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahNo ratings yet
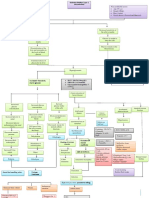
- Concept Map AtekharlssDocument3 pagesConcept Map AtekharlssAsniah Hadjiadatu AbdullahNo ratings yet
- Psychiatric-Mental Health NursingDocument6 pagesPsychiatric-Mental Health NursingAsniah Hadjiadatu AbdullahNo ratings yet
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDocument12 pagesAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNo ratings yet
- Final Nursing CareplanDocument7 pagesFinal Nursing CareplanAsniah Hadjiadatu AbdullahNo ratings yet
- Assessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationDocument11 pagesAssessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationAsniah Hadjiadatu Abdullah100% (1)
- Physiology MCQsDocument17 pagesPhysiology MCQsVikash KushwahaNo ratings yet
- Betelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesDocument37 pagesBetelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesMuh AqwilNo ratings yet
- Local Plants From Lom and Sawang Ethnics As Anti - DiahrezaDocument4 pagesLocal Plants From Lom and Sawang Ethnics As Anti - DiahrezaMuhammad Faiq FadhllurohmanNo ratings yet
- Therapy Selection For Tinea Corporis and Cruris With CommorbidityDocument9 pagesTherapy Selection For Tinea Corporis and Cruris With CommorbidityShimie Shimie KokobopNo ratings yet
- Nutrients: B12 As A Treatment For Peripheral Neuropathic Pain: A Systematic ReviewDocument16 pagesNutrients: B12 As A Treatment For Peripheral Neuropathic Pain: A Systematic ReviewDeproissantNo ratings yet
- 2NDDocument176 pages2NDArjay NasirinNo ratings yet
- Plants Used in Veterinary MedicineDocument297 pagesPlants Used in Veterinary MedicinefdfdfdfNo ratings yet
- Ointments: Chemical Properties Physical PropertiesDocument3 pagesOintments: Chemical Properties Physical PropertiesYunoNo ratings yet
- Analytical Method Development and Validation of Levofloxacin and Ornidazole Tablets by RP-HPLC MethodDocument8 pagesAnalytical Method Development and Validation of Levofloxacin and Ornidazole Tablets by RP-HPLC MethodMuhammad UbaidNo ratings yet
- Urtica Dioica: Botanical Name Common Name(s) : Plant Family: Parts Used: Active ConstituentsDocument4 pagesUrtica Dioica: Botanical Name Common Name(s) : Plant Family: Parts Used: Active ConstituentsgabsNo ratings yet
- Notice of Liability With AppendicesDocument38 pagesNotice of Liability With AppendicesAngela DuncalfNo ratings yet
- Tech LA and ComplicationsDocument43 pagesTech LA and ComplicationsPakistan Dental SocietyNo ratings yet
- Nadolol (RX) : Category: Beta-BlockersDocument6 pagesNadolol (RX) : Category: Beta-BlockersSerious BlackNo ratings yet
- Commonly Used Premedication Regimens: TaxanesDocument2 pagesCommonly Used Premedication Regimens: TaxanesnurulNo ratings yet
- Medication To Treat WithdrawalDocument2 pagesMedication To Treat WithdrawalRNStudent1No ratings yet
- AntibioticsDocument7 pagesAntibioticsCeleste Largo Arayan-LedesmaNo ratings yet
- Ijccm 23 S272Document6 pagesIjccm 23 S272Any MartNo ratings yet
- Pharmacy Study Plan2016eDocument41 pagesPharmacy Study Plan2016eأحمد العراقيNo ratings yet
- Effect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialDocument8 pagesEffect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialH Yudi IriantoNo ratings yet
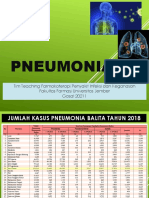
- Pneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Document67 pagesPneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Evie WulansariNo ratings yet
- Makalah Bahasa Inggris Dangers of DrugsDocument13 pagesMakalah Bahasa Inggris Dangers of DrugsSilvia LestariNo ratings yet
- 2005 Pleiotropic Effects of StatinsDocument9 pages2005 Pleiotropic Effects of StatinsK KNo ratings yet
- High AlertDocument180 pagesHigh AlertDewi MuthiahNo ratings yet
- Bacterial InfectionsDocument47 pagesBacterial InfectionsSNo ratings yet
- Chemical Composition Copper PDFDocument4 pagesChemical Composition Copper PDFtoppfartNo ratings yet
- SISTEMATIC REVIEW - I Nyoman Triaditya Kresna Putra - 71225050 - 10b.id - enDocument19 pagesSISTEMATIC REVIEW - I Nyoman Triaditya Kresna Putra - 71225050 - 10b.id - enTriaditya KresnaNo ratings yet
- Group A Streptococcus Antibiotic ResistanceDocument8 pagesGroup A Streptococcus Antibiotic Resistanceselandia nisrinaNo ratings yet