You might also like
- Bacteria ChartsDocument11 pagesBacteria ChartsFlowerNo ratings yet
- Infectious Disease - BoardsDocument8 pagesInfectious Disease - BoardsSoojung NamNo ratings yet
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- Swine 2Document40 pagesSwine 2Keegan McElroyNo ratings yet
- Gram Positive: CoccusDocument8 pagesGram Positive: CoccusLM MysNo ratings yet
- Food PoisoningDocument19 pagesFood PoisoningHemanathan PraemNo ratings yet
- Microbiology NotesDocument13 pagesMicrobiology NotesMalekNo ratings yet
- Chapter 43: Nursing Care of A Family When A Child Has An Infectious Disorder The Infectious Process #1 Infectious Disease in ChildrenDocument20 pagesChapter 43: Nursing Care of A Family When A Child Has An Infectious Disorder The Infectious Process #1 Infectious Disease in ChildrenMark oliver Gonzales100% (1)
- Thermobacteriology I: Food Microbiology and Public HealthDocument28 pagesThermobacteriology I: Food Microbiology and Public HealthHasan TheMcNo ratings yet
- YersiniosisDocument2 pagesYersiniosisMaisarah RepinNo ratings yet
- PertussisDocument13 pagesPertussisRhuthree Mabalacat100% (1)
- Approach To Patient With Diarrhea and VomitingDocument4 pagesApproach To Patient With Diarrhea and VomitingRed DevilNo ratings yet
- Digestive System InfectionsDocument30 pagesDigestive System InfectionsGoNo ratings yet
- Birao Sas 13 Microbiology and ParasitologyDocument9 pagesBirao Sas 13 Microbiology and ParasitologyFrancis Jacob Dejecacion GarcesNo ratings yet
- Daren G. Linatoc, RN, RM, LPT, Man, MaedDocument36 pagesDaren G. Linatoc, RN, RM, LPT, Man, MaedMike Faustino SolangonNo ratings yet
- Waterborne Diseases: Group 2Document21 pagesWaterborne Diseases: Group 2Jay RickNo ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- Infectious Diseases Tabelle (Examen 6. Jahr)Document34 pagesInfectious Diseases Tabelle (Examen 6. Jahr)Aastha SethNo ratings yet
- Infectious DocumentDocument8 pagesInfectious DocumentMohan SrinivasNo ratings yet
- Diarrhoea in MedicineDocument10 pagesDiarrhoea in MedicineMohd NadeemNo ratings yet
- Guidelines Emporical Antibiotic Therapy in AdultDocument2 pagesGuidelines Emporical Antibiotic Therapy in Adultgulf jobsNo ratings yet
- Approach To UTIDocument3 pagesApproach To UTIRochelle CionNo ratings yet
- PHARMA MIDTERM 2ndyrnsgDocument38 pagesPHARMA MIDTERM 2ndyrnsgquincy fajardoNo ratings yet
- Virus - SystemsDocument9 pagesVirus - SystemsHanunNo ratings yet
- Food Poisoning, Bacterial - ClinicalKeyDocument19 pagesFood Poisoning, Bacterial - ClinicalKeyclarestaNo ratings yet
- BenadrylDocument2 pagesBenadrylsamfandood10No ratings yet
- Beta-Lactams: Ampicillin, Amoxicillin, Third-Generation Cephalosporins (Cefixime, Ceftriaxone)Document2 pagesBeta-Lactams: Ampicillin, Amoxicillin, Third-Generation Cephalosporins (Cefixime, Ceftriaxone)Angelo MichaelNo ratings yet
- Staph. Aureus Staph. Epidermidis Staph. SaprophyticusDocument5 pagesStaph. Aureus Staph. Epidermidis Staph. SaprophyticusTom PedersonNo ratings yet
- Oxidase - : EnterobacteriaceaeDocument1 pageOxidase - : EnterobacteriaceaeTaylor EdgleyNo ratings yet
- Summarize Notes On ImciDocument6 pagesSummarize Notes On ImciI'm Just A BurgerNo ratings yet
- Clostridoides DifficileDocument2 pagesClostridoides Difficileyabhas chhetriNo ratings yet
- Pathologic and NonDocument11 pagesPathologic and NonAisha DoreenNo ratings yet
- DIPTHERIADocument2 pagesDIPTHERIADr KhatidjaNo ratings yet
- Diarrhea in The Elderly: Initial or 1 RecurrenceDocument1 pageDiarrhea in The Elderly: Initial or 1 Recurrencedewi wulandariNo ratings yet
- Infectious Diarrhea: Gail S. Itokazu, David T. Bearden, and Larry H. DanzigerDocument23 pagesInfectious Diarrhea: Gail S. Itokazu, David T. Bearden, and Larry H. DanzigerRismaAjhaNo ratings yet
- Diarrhea PEDSDocument10 pagesDiarrhea PEDSOasis LimitedNo ratings yet
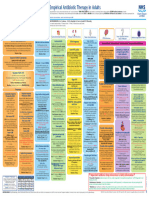
- 2021 Infection Management PosterDocument1 page2021 Infection Management PosterBosco WoodsNo ratings yet
- Gastroenteritis Dan DehidrasiDocument5 pagesGastroenteritis Dan DehidrasiSelly TiyaningrumNo ratings yet
- Micro by DR - Hesham (GIT)Document65 pagesMicro by DR - Hesham (GIT)abcde990075No ratings yet
- Food Microbiolog - Modified & CorrectedDocument25 pagesFood Microbiolog - Modified & CorrectedssalahNo ratings yet
- Pertemuan Ke-3 GASTRODocument36 pagesPertemuan Ke-3 GASTROwidya melianitaNo ratings yet
- Tuberculosis and CestodesDocument4 pagesTuberculosis and CestodesRizalyn Padua ReyNo ratings yet
- Foodborne Illness: Members: Nguy Minh Hoang Pham Nhat Thao Linh Le Thi Huyen Trang Instructor: Vo Le Dinh TamDocument13 pagesFoodborne Illness: Members: Nguy Minh Hoang Pham Nhat Thao Linh Le Thi Huyen Trang Instructor: Vo Le Dinh TamThảo LinhNo ratings yet
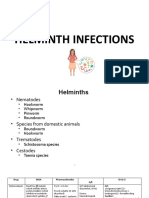
- HelminthsDocument11 pagesHelminthsTienneNo ratings yet
- Tinywow Communicable-Diseases 48897647 15Document1 pageTinywow Communicable-Diseases 48897647 15JULIUS CEZAR QUINAYNo ratings yet
- Diarrhea UpdatedDocument66 pagesDiarrhea UpdatedAna KarlaNo ratings yet
- FBD 2021Document99 pagesFBD 2021Ruth Mary PadaNo ratings yet
- 0506hoENTEROVIRAL INFECTIONSDocument57 pages0506hoENTEROVIRAL INFECTIONSAmandeep SinghNo ratings yet
- Infectious Disease of The Gastro Intestinal TractDocument12 pagesInfectious Disease of The Gastro Intestinal TractCj PajarillagaNo ratings yet
- Test 2 ChartDocument29 pagesTest 2 Chartapi-26938624No ratings yet
- PEDIA Bacterial Infections Part 2 Dr. E. Lim FinalDocument5 pagesPEDIA Bacterial Infections Part 2 Dr. E. Lim FinalClaire DuNo ratings yet
- OrganismDocument3 pagesOrganismJoanne Alyssa Hernandez LascanoNo ratings yet
- DIPTHERIADocument1 pageDIPTHERIAGrace StephanieNo ratings yet
- FST-602 Food Safety Bacterial Food Infections (Part-3) Lecture # 5Document18 pagesFST-602 Food Safety Bacterial Food Infections (Part-3) Lecture # 5muqaddasNo ratings yet
- Micro Part 3Document180 pagesMicro Part 3Perlie CNo ratings yet
- NCM116 CDN Gastrointestinal LECDocument18 pagesNCM116 CDN Gastrointestinal LECMilcah NuylesNo ratings yet
- Common Foodborne PathogensDocument3 pagesCommon Foodborne PathogensO PNo ratings yet
- Summary Final 2022Document12 pagesSummary Final 2022Rana zaatrehNo ratings yet
- Biology Investigatory Project Viral DiseasesDocument16 pagesBiology Investigatory Project Viral DiseasesAman MujeebNo ratings yet
- Ampicillin Sodium (Polypen)Document3 pagesAmpicillin Sodium (Polypen)Charlene Serino JavierNo ratings yet
- Foodborne IllnessDocument13 pagesFoodborne IllnessThảo LinhNo ratings yet
- Week 5 Past Perfect Practice 2Document4 pagesWeek 5 Past Perfect Practice 2Soldjair Mantari SotoNo ratings yet
- Staphylococci 18 StudentDocument42 pagesStaphylococci 18 StudentJulia MartinezNo ratings yet
- Compilation of Infectious Diseases: A Project in Community and Public HealthDocument8 pagesCompilation of Infectious Diseases: A Project in Community and Public HealthAbigail VirataNo ratings yet
- 61Document205 pages61Carlos HernándezNo ratings yet
- Pharmacology II Sem V Question BankDocument11 pagesPharmacology II Sem V Question BankabcNo ratings yet
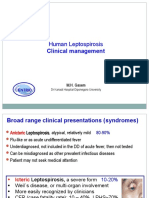
- Lepto Clinical Management GLEAN 2019 - M GasemDocument42 pagesLepto Clinical Management GLEAN 2019 - M GasemSelfie C RijalNo ratings yet
- Cause and Effects of PneumoniaDocument1 pageCause and Effects of PneumoniaAlmer OstreaNo ratings yet
- Diseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HDocument29 pagesDiseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HSuleman MuhammadNo ratings yet
- Background: Pediatric Chickenpox Next Section: PathophysiologyDocument12 pagesBackground: Pediatric Chickenpox Next Section: PathophysiologyRachel Johann Aquinto100% (1)
- Hamester: Submitted To: DR - Waqas Ahmed Submitted By: Shahbaz Ahmed Registration No:2017-Dvmn-040Document43 pagesHamester: Submitted To: DR - Waqas Ahmed Submitted By: Shahbaz Ahmed Registration No:2017-Dvmn-040Shahbaz AhmedNo ratings yet
- Bacterial Skin InfectionsDocument73 pagesBacterial Skin InfectionsAnthony Bravo CortezNo ratings yet
- COVID 19 Bharat India Report November09 2022 DailyCases 1116 Deaths 5 Based 781 DaysAnalysis Fbclid IwAR2orDocument225 pagesCOVID 19 Bharat India Report November09 2022 DailyCases 1116 Deaths 5 Based 781 DaysAnalysis Fbclid IwAR2orP Eng Suraj SinghNo ratings yet
- Humaniora Ii - 26 Maret 20 - 1 Jam - Endah - Kebudayaan Dan KesehatanDocument70 pagesHumaniora Ii - 26 Maret 20 - 1 Jam - Endah - Kebudayaan Dan KesehatanpkmsoboNo ratings yet
- Whooping CoughDocument72 pagesWhooping Coughwengie100% (1)
- 2011 - 4 Annual Report Detail Idsp Banaskantha 2011Document63 pages2011 - 4 Annual Report Detail Idsp Banaskantha 2011Pankaj ModhNo ratings yet
- 1 - Norovirus Care Home Poster 2018Document1 page1 - Norovirus Care Home Poster 2018GarryNo ratings yet
- ID4013 - SPW103 - Assessment - 2 - Response Template - 230321 2Document20 pagesID4013 - SPW103 - Assessment - 2 - Response Template - 230321 2SUCHETA DASNo ratings yet
- SeqdumpDocument7 pagesSeqdumpAnayantzin AyalaNo ratings yet
- JBNJN - Docx ENGLISHDocument2 pagesJBNJN - Docx ENGLISHمحسن حدوان عليخانNo ratings yet
- UntitledDocument5 pagesUntitledCresensia ElkesiaNo ratings yet
- Reference PDFDocument5 pagesReference PDFWina BudiartiNo ratings yet
- 16/09/2015 1 Mujtaba AshrafDocument44 pages16/09/2015 1 Mujtaba Ashrafதீரன் சக்திவேல்No ratings yet
- DHQ HPC Cord Questionnairev1Document3 pagesDHQ HPC Cord Questionnairev1DalokeshNo ratings yet
- BF Builders and Construction Corporation Hiv/Aids Workplace Policy and ProgramDocument4 pagesBF Builders and Construction Corporation Hiv/Aids Workplace Policy and Programglenn dalesNo ratings yet
- MCM Fact Sheet 191009Document6 pagesMCM Fact Sheet 191009Ruth CandorNo ratings yet
- Icd 10 CM Pcs Coding Theory and Practice 2017 Edition 1st Edition Lovaasen Test BankDocument12 pagesIcd 10 CM Pcs Coding Theory and Practice 2017 Edition 1st Edition Lovaasen Test Bankgisellephongejs100% (36)
- Avion FluDocument1 pageAvion FluImaan RiazNo ratings yet
- Limitations Results: Congenital Syphilis: Management Dilemmas Using Reverse ScreeningDocument1 pageLimitations Results: Congenital Syphilis: Management Dilemmas Using Reverse ScreeningFaye Cabotaje LinganNo ratings yet