You might also like
- OET Writing and Speaking Made Easy For NursesDocument143 pagesOET Writing and Speaking Made Easy For NursesLiju K Oommen97% (32)
- Hotel Design Planning and DevelopmentDocument30 pagesHotel Design Planning and DevelopmentTio Yogatma Yudha14% (7)
- Performing An A-G Patient Assessment: A Step-By-Step GuideDocument3 pagesPerforming An A-G Patient Assessment: A Step-By-Step GuidenasimhsNo ratings yet
- Pharmacology Review For NursesDocument11 pagesPharmacology Review For Nursesisabel_avancena100% (4)
- Pharmacology Review For NursesDocument11 pagesPharmacology Review For Nursesisabel_avancena100% (4)
- Korba - BAH Online Temp MonitoringDocument7 pagesKorba - BAH Online Temp Monitoringrama jenaNo ratings yet
- It Is What It IsDocument9 pagesIt Is What It IsWU CHANGNo ratings yet
- Nurse Caring Behaviors From Patients' and Nurses' Perspective: A Comparative StudyDocument8 pagesNurse Caring Behaviors From Patients' and Nurses' Perspective: A Comparative StudyYohana hale heretNo ratings yet
- 37 Erzincanli Original 14 1Document8 pages37 Erzincanli Original 14 1Tarandam INo ratings yet
- Research ForumDocument34 pagesResearch ForumJustine May GervacioNo ratings yet
- Nurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesDocument5 pagesNurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesShiee Nevhie ParaDinata WapersNo ratings yet
- 9 Soriano Original 10 2Document7 pages9 Soriano Original 10 2AllamaNo ratings yet
- Negar and Eh 2014Document4 pagesNegar and Eh 2014vindhiNo ratings yet
- Caring Efficacy and Nurse Caring Behavior in Taking Care of Critical PatientsDocument7 pagesCaring Efficacy and Nurse Caring Behavior in Taking Care of Critical PatientssryNo ratings yet
- Nursing Open - 2020 - Akansel - Nurses Perceptions of Caring Activities in NursingDocument11 pagesNursing Open - 2020 - Akansel - Nurses Perceptions of Caring Activities in NursingAhmad SyaripudinNo ratings yet
- Patient ParticipationDocument8 pagesPatient ParticipationJumania SeptarianiNo ratings yet
- Handover Paper Final 22 3 16 BJNDocument13 pagesHandover Paper Final 22 3 16 BJNsisaraaah12No ratings yet
- Sample - Critical Review of ArticleDocument11 pagesSample - Critical Review of Articleacademicproffwritter100% (1)
- Nurses Education and Motivation Towards Nursing DocumentationDocument5 pagesNurses Education and Motivation Towards Nursing DocumentationEdwardoNo ratings yet
- Nurse Education Today: Joelle Yan Xin Chua, Shefaly ShoreyDocument9 pagesNurse Education Today: Joelle Yan Xin Chua, Shefaly ShoreyflorenceNo ratings yet
- A Psychometric Analysis of TheDocument10 pagesA Psychometric Analysis of TheEva Yuliana YulianaNo ratings yet
- Ncoaj 05 00123Document7 pagesNcoaj 05 00123Afka SajaNo ratings yet
- Jurnal Paliatif AdhityaDaiskyYanuarDocument5 pagesJurnal Paliatif AdhityaDaiskyYanuarDaisky Rafif MaulanaNo ratings yet
- Am I Doing The Right Thing Provider Perspectives On Improving Palliative Care in The Emergency Department 2009 Annals of Emergency MedicineDocument9 pagesAm I Doing The Right Thing Provider Perspectives On Improving Palliative Care in The Emergency Department 2009 Annals of Emergency MedicineTUTIK SISWATINo ratings yet
- Patient Satisfaction With Nursing Care Quality and Patient Safety Culture in The Medical-Surgical UnitDocument10 pagesPatient Satisfaction With Nursing Care Quality and Patient Safety Culture in The Medical-Surgical UnitNurunnisa yrNo ratings yet
- Revised Research Study NCM111Document23 pagesRevised Research Study NCM111Arvin PenalosaNo ratings yet
- Integrative Review of The LiteratureDocument21 pagesIntegrative Review of The Literatureapi-507822143No ratings yet
- Medical Record-Keeping and PatDocument14 pagesMedical Record-Keeping and PatMathilda UllyNo ratings yet
- Intensive & Critical Care Nursing: Research ArticleDocument9 pagesIntensive & Critical Care Nursing: Research ArticleNur MiladiyahNo ratings yet
- Patient Satisfaction With Nursing Care in Jordan: Correspondence Raeda Fawzi Abualrub Po Box 1894 Irbid JordanDocument10 pagesPatient Satisfaction With Nursing Care in Jordan: Correspondence Raeda Fawzi Abualrub Po Box 1894 Irbid JordantimesNo ratings yet
- Professional Med J Q 2013 20 6 973 980Document8 pagesProfessional Med J Q 2013 20 6 973 980Vikram AripakaNo ratings yet
- Role of Critical Care Nurses in End-of-Life CareDocument32 pagesRole of Critical Care Nurses in End-of-Life Carejohn christopher JimenezNo ratings yet
- ArticleDocument11 pagesArticleKirubel TesfayeNo ratings yet
- Jurnal InternasionalDocument7 pagesJurnal InternasionalDina AryaniNo ratings yet
- An Analysis of The Concept of Patient ParticipationDocument10 pagesAn Analysis of The Concept of Patient ParticipationVpkChat Twitterchat Voor Verpleegkundigen100% (1)
- 17 ManarDocument14 pages17 Manarheba abd elazizNo ratings yet
- Selvin 2021Document8 pagesSelvin 2021Stella GašparušNo ratings yet
- Being Respected by Nurses: Measuring Older Patients' PerceptionsDocument12 pagesBeing Respected by Nurses: Measuring Older Patients' PerceptionsAurora Violeta Zapata RuedaNo ratings yet
- MENJ - Volume 2 - Issue 1 - Pages 27-42Document16 pagesMENJ - Volume 2 - Issue 1 - Pages 27-42منوعات قرآن واحاديث واخبار وكرة قدمNo ratings yet
- Akbas (2019) Patient Satisfaction On Nursing Care The Case of Gynecology and Obstetrics ClinicsDocument10 pagesAkbas (2019) Patient Satisfaction On Nursing Care The Case of Gynecology and Obstetrics ClinicsDiego RiveraNo ratings yet
- Aziz IDocument5 pagesAziz InasimhsNo ratings yet
- Physician Nurse RelationshipDocument59 pagesPhysician Nurse RelationshipJoana RomeiroNo ratings yet
- Knowledge, Attitude, Performance and Associated Factors Towards Nursing Documentation Among Nurses in Public Hospitals, Sana'a City, YemenDocument6 pagesKnowledge, Attitude, Performance and Associated Factors Towards Nursing Documentation Among Nurses in Public Hospitals, Sana'a City, YemenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Persepsi Caring Case-JurnalDocument7 pagesPersepsi Caring Case-JurnalYuni PurwatiNo ratings yet
- The Effect of Structured Nursing Rounds On The Level Nursing Care Satisfaction of Patient in A Selected Tertiary Care Hospital, PuducherryDocument15 pagesThe Effect of Structured Nursing Rounds On The Level Nursing Care Satisfaction of Patient in A Selected Tertiary Care Hospital, PuducherryIJAR JOURNALNo ratings yet
- Patient Awareness and Role in Attaining Health - 2021 - International Journal ofDocument6 pagesPatient Awareness and Role in Attaining Health - 2021 - International Journal ofRonald QuezadaNo ratings yet
- 1.pdf JsessionidDocument39 pages1.pdf JsessionidAlvin Josh CalingayanNo ratings yet
- Knowledge and Practice of Documentation Among Nurses in Ahmadu Bello University Teaching Hospital (Abuth) Zaria, Kaduna State.Document6 pagesKnowledge and Practice of Documentation Among Nurses in Ahmadu Bello University Teaching Hospital (Abuth) Zaria, Kaduna State.IOSRjournalNo ratings yet
- Socko Low 2014Document8 pagesSocko Low 2014Tri Monarita JohanNo ratings yet
- Senior Capstone Scholarly PaperDocument8 pagesSenior Capstone Scholarly Paperapi-653708698No ratings yet
- Anaba (2020) Patient Satisfaction With Perioperative Nursing Care in A Tertiary Hospital in GhanaDocument13 pagesAnaba (2020) Patient Satisfaction With Perioperative Nursing Care in A Tertiary Hospital in GhanaDiego RiveraNo ratings yet
- 4.arif WidodoDocument6 pages4.arif WidodoAri AzhariNo ratings yet
- International Journal of Africa Nursing Sciences: Hailemichael Kindie Abate, Yeneabat Birhanu, Mignote Hailu GebrieDocument7 pagesInternational Journal of Africa Nursing Sciences: Hailemichael Kindie Abate, Yeneabat Birhanu, Mignote Hailu Gebrieاحمد العايديNo ratings yet
- European Journal of Oncology Nursing: A B C ADocument8 pagesEuropean Journal of Oncology Nursing: A B C AfitrilihawaNo ratings yet
- Critical Care Nurses' Experiences of End-of-Life Care: A Qualitative StudyDocument15 pagesCritical Care Nurses' Experiences of End-of-Life Care: A Qualitative StudyHendri PurwadiNo ratings yet
- Infeksi Nifas PublisherDocument4 pagesInfeksi Nifas PublisherYayha AgathaaNo ratings yet
- NursingDocument10 pagesNursinglshani KhannaNo ratings yet
- Evaluation of Chronic Patient Nursing Care by The Patients - A University Hospital CaseDocument13 pagesEvaluation of Chronic Patient Nursing Care by The Patients - A University Hospital CaseGlobal Research and Development ServicesNo ratings yet
- Exploring Islamic Based Caring Practice in Intensive Care Unit: A Qualitative StudyDocument10 pagesExploring Islamic Based Caring Practice in Intensive Care Unit: A Qualitative StudyineNo ratings yet
- Health Notions, Volume 1 Issue 4 (October-December 2017) ISSN 2580-4936Document7 pagesHealth Notions, Volume 1 Issue 4 (October-December 2017) ISSN 2580-4936Muhammad DzikrullohNo ratings yet
- Self-Leadership in A Critical Care Outreach Service For Quality Patient CareDocument19 pagesSelf-Leadership in A Critical Care Outreach Service For Quality Patient CareKamila AmmarNo ratings yet
- Tugas Bahasa Inggris - Temu 1 - KLP 8 - A12 BDocument8 pagesTugas Bahasa Inggris - Temu 1 - KLP 8 - A12 BErina NiluhNo ratings yet
- Article in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudyDocument7 pagesArticle in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudySimson TameonNo ratings yet
- Differences Between Patients' Expectations and Satisfaction With Nursing Care in A Private Hospital in JordanDocument7 pagesDifferences Between Patients' Expectations and Satisfaction With Nursing Care in A Private Hospital in JordantimesNo ratings yet
- Findings Done in Falgun 3Document32 pagesFindings Done in Falgun 3Bhageshwar ChaudharyNo ratings yet
- Correctional Nursing: Scope and Standards of Practice, Third EditionFrom EverandCorrectional Nursing: Scope and Standards of Practice, Third EditionRating: 5 out of 5 stars5/5 (1)
- Job Description / Competency Profile: Job Title Payband/Grade Directorate Job Description ReferenceDocument5 pagesJob Description / Competency Profile: Job Title Payband/Grade Directorate Job Description ReferencenasimhsNo ratings yet
- Acute Kidney Injury: Chapter ContentsDocument22 pagesAcute Kidney Injury: Chapter ContentsnasimhsNo ratings yet
- PT - and NursesDocument7 pagesPT - and NursesnasimhsNo ratings yet
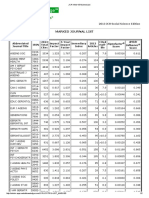
- Marked Journal List: 2013 JCR Social Science EditionDocument2 pagesMarked Journal List: 2013 JCR Social Science EditionnasimhsNo ratings yet
- 14.4 MSDocument14 pages14.4 MSnasimhsNo ratings yet
- Acute Decompensated Heart Failure: A Study of Nursing CareDocument12 pagesAcute Decompensated Heart Failure: A Study of Nursing CarenasimhsNo ratings yet
- Using A Systematic Approach To Assess An Acutely Unwell Patient With Catatonia: A Case StudyDocument9 pagesUsing A Systematic Approach To Assess An Acutely Unwell Patient With Catatonia: A Case StudynasimhsNo ratings yet
- Acute Kidney Injury: Mark BevanDocument42 pagesAcute Kidney Injury: Mark BevannasimhsNo ratings yet
- Accelerated Idioventricular RhythmDocument4 pagesAccelerated Idioventricular RhythmnasimhsNo ratings yet
- Marked Journal List: 2013 JCR Social Science EditionDocument2 pagesMarked Journal List: 2013 JCR Social Science EditionnasimhsNo ratings yet
- Marked Journal List: 2013 JCR Social Science EditionDocument2 pagesMarked Journal List: 2013 JCR Social Science EditionnasimhsNo ratings yet
- Which of The Following Statements About The Human Nervous System Is True?Document12 pagesWhich of The Following Statements About The Human Nervous System Is True?nasimhsNo ratings yet
- Marked Journal List: 2013 JCR Social Science EditionDocument2 pagesMarked Journal List: 2013 JCR Social Science EditionnasimhsNo ratings yet
- (IELTSMaterial - Com) 100 IELTS Speaking Part 2 Topics in 2016 & 2017 & Sample Answers PDFDocument135 pages(IELTSMaterial - Com) 100 IELTS Speaking Part 2 Topics in 2016 & 2017 & Sample Answers PDFUyenNo ratings yet
- Media PDFDocument21 pagesMedia PDFlethuhaiNo ratings yet
- AirwayDocument2 pagesAirwaynasimhsNo ratings yet
- Accelerated Idioventricular RhythmDocument4 pagesAccelerated Idioventricular RhythmnasimhsNo ratings yet
- Role of Observational Medicine in EmergencyDocument13 pagesRole of Observational Medicine in EmergencyazhaabazNo ratings yet
- Blood TubesDocument1 pageBlood TubesnasimhsNo ratings yet
- Nclex Lab ValuesDocument6 pagesNclex Lab ValuesnasimhsNo ratings yet
- Weight Box SHOTDocument1 pageWeight Box SHOTnasimhsNo ratings yet
- Lex-Mental HealthDocument49 pagesLex-Mental HealthnasimhsNo ratings yet
- Common Laboratory Values PDF GreenDocument11 pagesCommon Laboratory Values PDF GreennasimhsNo ratings yet
- λεξ ψ υγειαDocument87 pagesλεξ ψ υγειαnasimhsNo ratings yet
- Unexpected Transfusion blc6991p FinalDocument2 pagesUnexpected Transfusion blc6991p FinalnasimhsNo ratings yet
- Nerve SynapseDocument2 pagesNerve SynapsenasimhsNo ratings yet
- DNT Audit Cash CountDocument2 pagesDNT Audit Cash CountAnonymous Pu7TnbCFC0No ratings yet
- Technical File D13-MH, MG IMO Tier 11 GLDocument18 pagesTechnical File D13-MH, MG IMO Tier 11 GLsfsdffdsdfsdfsdfNo ratings yet
- LAC-Documentation-Tool Session 2Document4 pagesLAC-Documentation-Tool Session 2DenMark Tuazon-RañolaNo ratings yet
- 256267a1Document5,083 pages256267a1Елизавета ШепелеваNo ratings yet
- The Graduation Commencement Speech You Will Never HearDocument4 pagesThe Graduation Commencement Speech You Will Never HearBernie Lutchman Jr.No ratings yet
- Power Bi ProjectsDocument15 pagesPower Bi ProjectssandeshNo ratings yet
- Learning Online: Veletsianos, GeorgeDocument11 pagesLearning Online: Veletsianos, GeorgePsico XavierNo ratings yet
- DANZIG, Richard, A Comment On The Jurisprudence of The Uniform Commercial Code, 1975 PDFDocument17 pagesDANZIG, Richard, A Comment On The Jurisprudence of The Uniform Commercial Code, 1975 PDFandresabelrNo ratings yet
- AIATS 2021 (OYMCF) Test 01 Offline - Code A - SolutionsDocument34 pagesAIATS 2021 (OYMCF) Test 01 Offline - Code A - Solutionsbhavyakavya mehta100% (1)
- LLM DissertationDocument94 pagesLLM Dissertationjasminjajarefe100% (1)
- R4 User GuideDocument48 pagesR4 User GuideAaron SmithNo ratings yet
- Masonry Brickwork 230 MMDocument1 pageMasonry Brickwork 230 MMrohanNo ratings yet
- Phys114 Ps 1Document11 pagesPhys114 Ps 1Reine Amabel JarudaNo ratings yet
- Classification of Textile Testing - OrDNURDocument6 pagesClassification of Textile Testing - OrDNURKazi ShorifNo ratings yet
- Form 1 ADocument2 pagesForm 1 ARohit Jain100% (1)
- Ipo Exam Revised SyllabusDocument1 pageIpo Exam Revised Syllabusজ্যোতিৰ্ময় বসুমতাৰীNo ratings yet
- Test SessionDocument2 pagesTest SessionMuhammad Fiaz AslamNo ratings yet
- Malaysia Year 2011 Calendar: Translate This PageDocument3 pagesMalaysia Year 2011 Calendar: Translate This PageStorgas FendiNo ratings yet
- 99 181471 - Sailor System 6000b 150w Gmdss MFHF - Ec Type Examination Module B - Uk TuvsudDocument6 pages99 181471 - Sailor System 6000b 150w Gmdss MFHF - Ec Type Examination Module B - Uk TuvsudPavankumar PuvvalaNo ratings yet
- January 2013 Igcse Timetable 22-06-2012Document2 pagesJanuary 2013 Igcse Timetable 22-06-2012Rizwanur RahmanNo ratings yet
- Nature and Scope of Marketing Marketing ManagementDocument51 pagesNature and Scope of Marketing Marketing ManagementFeker H. MariamNo ratings yet
- CV Abdalla Ali Hashish-Nursing Specialist.Document3 pagesCV Abdalla Ali Hashish-Nursing Specialist.Abdalla Ali HashishNo ratings yet
- Presentation On Ich Topics & Guidelines With A Special Reference ToDocument79 pagesPresentation On Ich Topics & Guidelines With A Special Reference ToVidyaNo ratings yet
- BỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔDocument5 pagesBỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔPhạm Thu NgaNo ratings yet
- Dr. Malik's Farms BrochureDocument18 pagesDr. Malik's Farms BrochureNeil AgshikarNo ratings yet
- Prof. Michael Murray - Some Differential Geometry ExercisesDocument4 pagesProf. Michael Murray - Some Differential Geometry ExercisesAnonymous 9rJe2lOskxNo ratings yet
- Impact of Recruitment & Selection on Employee RetentionDocument39 pagesImpact of Recruitment & Selection on Employee RetentiongizawNo ratings yet
- ThesisDocument250 pagesThesislax mediaNo ratings yet