You might also like
- Jurnal 2Document6 pagesJurnal 2RizkyNo ratings yet
- Bremond Gignac2010Document5 pagesBremond Gignac2010Muhammad Imam NoorNo ratings yet
- Research Article: Detection of Diabetic Retinopathy Using Bichannel Convolutional Neural NetworkDocument7 pagesResearch Article: Detection of Diabetic Retinopathy Using Bichannel Convolutional Neural NetworkMuhammad Imam NoorNo ratings yet
- Shabto 2020Document8 pagesShabto 2020Muhammad Imam NoorNo ratings yet
- Acanthamoeba Keratitis in Noncompliant Soft Contact Lenses UsersDocument7 pagesAcanthamoeba Keratitis in Noncompliant Soft Contact Lenses UsersMuhammad Imam NoorNo ratings yet
- Jurnal Mata 1Document4 pagesJurnal Mata 1Muhammad Imam NoorNo ratings yet
- Ophthalmologic Manifestations and Retinal Findings in Children With Down SyndromeDocument6 pagesOphthalmologic Manifestations and Retinal Findings in Children With Down SyndromeMuhammad Imam NoorNo ratings yet
- The Role of Head Elevation in Treatment of Vitreous HaemorrhageDocument7 pagesThe Role of Head Elevation in Treatment of Vitreous HaemorrhageMuhammad Imam NoorNo ratings yet
- Assessment of Tear-Evaporation Rate in Thyroid-Gland PatientsDocument5 pagesAssessment of Tear-Evaporation Rate in Thyroid-Gland PatientsMuhammad Imam NoorNo ratings yet
- Management of KeratitisDocument12 pagesManagement of KeratitisSeptian Harry WibowoNo ratings yet
- Jurnal Reading 3Document11 pagesJurnal Reading 3Muhammad Imam NoorNo ratings yet
- Research Article: The Adverse Impact of Glaucoma On Psychological Function and Daily Physical ActivityDocument8 pagesResearch Article: The Adverse Impact of Glaucoma On Psychological Function and Daily Physical ActivityMuhammad Imam NoorNo ratings yet
- Jurnal Mata 3Document6 pagesJurnal Mata 3Muhammad Imam NoorNo ratings yet
- Jurnal Reading 2Document6 pagesJurnal Reading 2Muhammad Imam NoorNo ratings yet
- Efficacy of 0.5% Levofloxacin and 5.0% Povidone-Iodine Eyedrops in Reducing Conjunctival Bacterial FloraDocument9 pagesEfficacy of 0.5% Levofloxacin and 5.0% Povidone-Iodine Eyedrops in Reducing Conjunctival Bacterial FloraMuhammad Imam NoorNo ratings yet
- Reoperations For Complications Within 90 Days After Glaucoma SurgeryDocument3 pagesReoperations For Complications Within 90 Days After Glaucoma SurgeryMuhammad Imam NoorNo ratings yet
- E-Cigarettes Use Behavior and Experience of AdultsDocument7 pagesE-Cigarettes Use Behavior and Experience of AdultsMuhammad Imam NoorNo ratings yet
- Clinical Manifestations, Diagnosis, and Surgery of Inferior Oblique Muscle EctopiaDocument5 pagesClinical Manifestations, Diagnosis, and Surgery of Inferior Oblique Muscle EctopiaMuhammad Imam NoorNo ratings yet
- A Comparison of Daily Versus Weekly Electronic Cigarette Users in Treatment For Substance AbuseDocument7 pagesA Comparison of Daily Versus Weekly Electronic Cigarette Users in Treatment For Substance AbuseMuhammad Imam NoorNo ratings yet
- Vent Rig Lio 2017Document2 pagesVent Rig Lio 2017Muhammad Imam NoorNo ratings yet
- Clinical Study: Systemic Factors Associated With Treatment Response in Diabetic Macular EdemaDocument6 pagesClinical Study: Systemic Factors Associated With Treatment Response in Diabetic Macular EdemaMuhammad Imam NoorNo ratings yet
- Research Article: Detection of Diabetic Retinopathy Using Bichannel Convolutional Neural NetworkDocument7 pagesResearch Article: Detection of Diabetic Retinopathy Using Bichannel Convolutional Neural NetworkMuhammad Imam NoorNo ratings yet
- Social Media Use and Conduct Problems in Emerging Adults: Apid OmmunicationsDocument5 pagesSocial Media Use and Conduct Problems in Emerging Adults: Apid OmmunicationsindahNo ratings yet
- Punia 2019Document2 pagesPunia 2019Muhammad Imam NoorNo ratings yet
- Psychiatric Comorbidity in Adolescent Electronic and Conventional Cigarette UseDocument19 pagesPsychiatric Comorbidity in Adolescent Electronic and Conventional Cigarette UseMuhammad Imam NoorNo ratings yet
- Association Between Electronic Cigarette Use and Smoking Reduction in FranceDocument8 pagesAssociation Between Electronic Cigarette Use and Smoking Reduction in FranceMuhammad Imam NoorNo ratings yet
- Bidirectional Associations Between Child Sleep Problems and Internalizing and Externalizing Difficulties From Preschool To Early AdolescenceDocument8 pagesBidirectional Associations Between Child Sleep Problems and Internalizing and Externalizing Difficulties From Preschool To Early AdolescenceMuhammad Imam NoorNo ratings yet
- 878Wag2015MS Urosepsis OverviewDocument20 pages878Wag2015MS Urosepsis OverviewMuhammad Imam NoorNo ratings yet
- Diagnosis and Management For UrosepsisDocument8 pagesDiagnosis and Management For UrosepsisMuhammad Imam NoorNo ratings yet
- Urosepsis-Etiology, Diagnosis, and Treatment: Continuing Medical EducationDocument14 pagesUrosepsis-Etiology, Diagnosis, and Treatment: Continuing Medical EducationMuhammad Imam NoorNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- January Month - Seva 2023Document3 pagesJanuary Month - Seva 2023saisri salesNo ratings yet
- Personality Profile 320Document3 pagesPersonality Profile 320api-404607062No ratings yet
- AngelsPart1 PDFDocument169 pagesAngelsPart1 PDFHayley MunguiaNo ratings yet
- Bridge Over Troubled Water - Brass BandDocument17 pagesBridge Over Troubled Water - Brass Banddudaxavier100% (2)
- 58-98HP C-MAX TRACTOR RANGE TECHNICAL SPECSDocument2 pages58-98HP C-MAX TRACTOR RANGE TECHNICAL SPECShuskerchampsNo ratings yet
- Orchestral Audition Training Article + Warm-Up Exercises For MusclesDocument9 pagesOrchestral Audition Training Article + Warm-Up Exercises For MusclesK.L.100% (2)
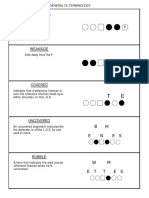
- OL TERMINOLOGY PRIMERDocument23 pagesOL TERMINOLOGY PRIMERJB Wells100% (1)
- Main Switch Cab: TKB 00801-033 According DrawingDocument1 pageMain Switch Cab: TKB 00801-033 According DrawingMiller Andres ArocaNo ratings yet
- Code GTA San AndreasDocument6 pagesCode GTA San AndreasKhaled AmalurNo ratings yet
- Nutrition for Exercise and Sports PerformanceDocument4 pagesNutrition for Exercise and Sports PerformanceAudrie Allyson GabalesNo ratings yet
- Reading Week 23Document4 pagesReading Week 23api-263759920No ratings yet
- 700 Diagrams of Chess Tactics Training Shumilin PDFDocument117 pages700 Diagrams of Chess Tactics Training Shumilin PDFKenaouia Bahaa0% (1)
- MED17.1.1 - Esquema ElétricoDocument29 pagesMED17.1.1 - Esquema ElétricoLucasNo ratings yet
- Current Affairs PDF July 16 31 2018Document106 pagesCurrent Affairs PDF July 16 31 2018Vineet SinghNo ratings yet
- The Jam - Start ChordsDocument5 pagesThe Jam - Start ChordsKat YaNo ratings yet
- Channel Lineup: 1-800-XFINITYDocument2 pagesChannel Lineup: 1-800-XFINITYLizbeth HerreraNo ratings yet
- Full Results & PositionsDocument6 pagesFull Results & Positionsgavin_holburnNo ratings yet
- 4tnv106t GgehcDocument22 pages4tnv106t GgehcDzmitryNo ratings yet
- Httpswww.tpss.Euresults2586drawsheets20juniors.pdfDocument20 pagesHttpswww.tpss.Euresults2586drawsheets20juniors.pdflanames1706No ratings yet
- Kawasaki Ninja 250 SL Standard 158468Document1 pageKawasaki Ninja 250 SL Standard 158468EKO FITRIYANTONo ratings yet
- Character SheetDocument1 pageCharacter SheetSteve Moseley100% (1)
- Zippo 2011 Spring Collection deDocument10 pagesZippo 2011 Spring Collection deKristiantoTulakNo ratings yet
- Character SheetDocument3 pagesCharacter SheetBarghus100% (1)
- Toyota Wigo 1.0 G AT Vs Honda Brio 1.2 V CVT Vs Suzuki Swift 1.2 GL CVT - AutoDealDocument7 pagesToyota Wigo 1.0 G AT Vs Honda Brio 1.2 V CVT Vs Suzuki Swift 1.2 GL CVT - AutoDealMaiNe KEhNo ratings yet
- Inspect escalator safety and performanceDocument3 pagesInspect escalator safety and performanceHong Leong KuNo ratings yet
- PRICE-LIST PREMIU deDocument46 pagesPRICE-LIST PREMIU deRevisate PanamaNo ratings yet
- Peru National Football Team: Blanquirroja ("The White-And-Red")Document16 pagesPeru National Football Team: Blanquirroja ("The White-And-Red")SashimiTourloublancNo ratings yet
- A MomentsDocument14 pagesA MomentsMartha DE Gama100% (2)
- Cablofil Wire Cable Tray TechnicalDocument4 pagesCablofil Wire Cable Tray TechnicalDaniel GranateNo ratings yet
- Maintain SF6 Circuit BreakersDocument5 pagesMaintain SF6 Circuit BreakerskienNo ratings yet