You might also like
- Cerebral PalsyDocument27 pagesCerebral PalsyJohn Paul Parungao CrisostomoNo ratings yet
- Reva Frozen ShoulderDocument6 pagesReva Frozen ShoulderVincent de CastroNo ratings yet
- College of Physical Therapy Sem2Document10 pagesCollege of Physical Therapy Sem2karen magallanesNo ratings yet
- Initial Evaluation General InformationDocument8 pagesInitial Evaluation General InformationJoanna EdenNo ratings yet
- Initial Evaluation I. General InformationDocument8 pagesInitial Evaluation I. General InformationJoanna EdenNo ratings yet
- Group 2 - IeDocument14 pagesGroup 2 - IeGabriel RagasaNo ratings yet
- Inpatient Group Case PreDocument7 pagesInpatient Group Case PreEarll Justin N. DataNo ratings yet
- PHC Ankle SprainDocument5 pagesPHC Ankle SprainMin WajeNo ratings yet
- Sample IE SOAP FormatDocument8 pagesSample IE SOAP Formatjamie mutucNo ratings yet
- IE Humeral Neck FractureDocument9 pagesIE Humeral Neck FractureEarll Justin N. DataNo ratings yet
- Sample Initial Evaluation PhysiotherapyDocument10 pagesSample Initial Evaluation PhysiotherapyWenzy CruzNo ratings yet
- CP ChartDocument17 pagesCP Chart林良駿No ratings yet
- Initial Evaluation For PoliomyelitisDocument5 pagesInitial Evaluation For PoliomyelitisVanessa Yvonne GurtizaNo ratings yet
- CDUH TBI GosarinDocument7 pagesCDUH TBI GosarinSergi Lee OrateNo ratings yet
- Initial Evaluation Case ConDocument8 pagesInitial Evaluation Case ConMichel BlueNo ratings yet
- Myelopathy: Clinical Clerkship of Neurology DepartmentDocument59 pagesMyelopathy: Clinical Clerkship of Neurology DepartmentWahyu PermataNo ratings yet
- MR Geri 20072023 FixDocument79 pagesMR Geri 20072023 FixIka Ayu ParamitaNo ratings yet
- Lateral EpicondylitisDocument8 pagesLateral EpicondylitismrwntrrNo ratings yet
- Farmakologi Pada Kasus TraumaDocument31 pagesFarmakologi Pada Kasus TraumajikhNo ratings yet
- Physical Therapy Evaluation / Plan of Care FormDocument8 pagesPhysical Therapy Evaluation / Plan of Care Formapi-551757456No ratings yet
- 5.2 Scoliosis - SoapDocument18 pages5.2 Scoliosis - SoapCeline Kyla MalloNo ratings yet
- 5.2 Scoliosis - SoapDocument18 pages5.2 Scoliosis - SoapCeline Kyla MalloNo ratings yet
- Saint Louis Hospital of The Sacred Department of Physical Medicine and Rehabilitation Baguio City PT Initial Evaluation General InformationDocument6 pagesSaint Louis Hospital of The Sacred Department of Physical Medicine and Rehabilitation Baguio City PT Initial Evaluation General InformationJoanna EdenNo ratings yet
- 見習模板最終版複製Document10 pages見習模板最終版複製林良駿No ratings yet
- Initial Evaluation General InformationDocument7 pagesInitial Evaluation General InformationJoanna EdenNo ratings yet
- Cerebral PalsyDocument7 pagesCerebral Palsyangel bolfriNo ratings yet
- PTMSK Case Write Up Example 2Document8 pagesPTMSK Case Write Up Example 2Tan Zhen XinNo ratings yet
- Morning ReportDocument56 pagesMorning ReportngurahNo ratings yet
- Case 3: Jalea, Moreno, RamosDocument29 pagesCase 3: Jalea, Moreno, RamosJemie JaleaNo ratings yet
- Objective Ie. QualimedDocument10 pagesObjective Ie. QualimedPhiliaMelAbarquezNo ratings yet
- Soap Note Sub-Acute TkaDocument6 pagesSoap Note Sub-Acute Tkaapi-3719716000% (1)
- Jimenez, Walter (Cdo)Document7 pagesJimenez, Walter (Cdo)Nichole Canoy AbrasaldoNo ratings yet
- Ie GR 1Document15 pagesIe GR 1NNMCNo ratings yet
- Ankle SprainDocument9 pagesAnkle SprainmrwntrrNo ratings yet
- PT Initial Evaluation For MSDocument3 pagesPT Initial Evaluation For MSKarolle Alyssa100% (1)
- IE Format 1Document9 pagesIE Format 1Alyssa GicaroNo ratings yet
- Ie ArthDocument10 pagesIe ArthVanessa Yvonne GurtizaNo ratings yet
- Chronic Restrictive Pulmonary DiseaseDocument17 pagesChronic Restrictive Pulmonary DiseaseBaz DomNo ratings yet
- Musculoskeletal System Examination For Neck and Shoulder StiffnessDocument4 pagesMusculoskeletal System Examination For Neck and Shoulder StiffnessnyeeperNo ratings yet
- BellsDocument6 pagesBellsMae NocheNo ratings yet
- Liskhairia - Spondilitis TuberculosaDocument25 pagesLiskhairia - Spondilitis TuberculosaFiki FerindraNo ratings yet
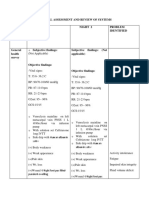
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDocument9 pagesPhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahNo ratings yet
- ORTHO Booklet 427-B1 FinalDocument226 pagesORTHO Booklet 427-B1 FinalMandisa Ndlovu Tenego0% (1)
- Interpretation: VS Are WNLDocument4 pagesInterpretation: VS Are WNLSteve ColbertNo ratings yet
- Hypothetical IE of Spinal Cord Injury (SCI)Document12 pagesHypothetical IE of Spinal Cord Injury (SCI)MIKEE MEDRANONo ratings yet
- Rom MMT Trunk Study Sheet 1Document3 pagesRom MMT Trunk Study Sheet 1api-242889989No ratings yet
- Acl ReconstructionDocument9 pagesAcl ReconstructionmrwntrrNo ratings yet
- Visual Disturbance Et Parese of Left Temporal BranchDocument6 pagesVisual Disturbance Et Parese of Left Temporal BranchRahmanda TaqwaNo ratings yet
- Ilmu Penyakit Saraf Case Report "Myeloradikulopati Torakolumbal E.C Fraktur Kompres"Document20 pagesIlmu Penyakit Saraf Case Report "Myeloradikulopati Torakolumbal E.C Fraktur Kompres"Hanif LatifNo ratings yet
- Status Can 270323Document6 pagesStatus Can 270323Putri AyuNo ratings yet
- Physiotherapy Neurological Assesment Form: JH RehabilitationDocument9 pagesPhysiotherapy Neurological Assesment Form: JH RehabilitationSureaka PonnusamyNo ratings yet
- Hypothetical IE For CVA/StrokeDocument19 pagesHypothetical IE For CVA/StrokeMIKEE MEDRANONo ratings yet
- Itb SyndromeDocument15 pagesItb SyndromemrwntrrNo ratings yet
- DKA PPT Report SidDocument70 pagesDKA PPT Report SidSid FlavierNo ratings yet
- Spinal Cord Assesment Form PTDocument8 pagesSpinal Cord Assesment Form PTSureaka PonnusamyNo ratings yet
- Manual TherapyDocument16 pagesManual TherapylecturioNo ratings yet
- 1.CASE Study Group-CDocument19 pages1.CASE Study Group-CNazmul HossainNo ratings yet
- CASE REPORT Vertigo PutriDocument20 pagesCASE REPORT Vertigo PutriRizqina PutriNo ratings yet
- Low Back Pain: General InfoDocument4 pagesLow Back Pain: General InfoErlinda RamosNo ratings yet
- Text For NoDocument3 pagesText For NoMasita NazalinNo ratings yet
- Psychiatry EmergencyDocument121 pagesPsychiatry EmergencyDr. Jayesh Patidar67% (6)
- Counterfeit DrugsDocument2 pagesCounterfeit DrugsfreeBlidaman0967% (3)
- NCP For Dizziness and HeadacheDocument4 pagesNCP For Dizziness and Headachekarthi karthi100% (1)
- OSH Manual Medium Risk EntitiesDocument122 pagesOSH Manual Medium Risk EntitiesNitika SinhaNo ratings yet
- EtikaDocument15 pagesEtikaWidya PratiwiNo ratings yet
- Design Brief PDFDocument8 pagesDesign Brief PDFNur Shahmira Ahmad ShahNo ratings yet
- Thesis SynopsisDocument14 pagesThesis SynopsisPooja BasavarajNo ratings yet
- Anticoagulant ReversalDocument4 pagesAnticoagulant Reversalapi-647779956No ratings yet
- Review Article: Common Periodontal Diseases of Children and AdolescentsDocument8 pagesReview Article: Common Periodontal Diseases of Children and AdolescentsGea Akalili SabrinaNo ratings yet
- How To Be A Business OwnerDocument34 pagesHow To Be A Business Ownersimbarashe mukondo100% (2)
- Peptan General BrochureDocument12 pagesPeptan General BrochurenadyaNo ratings yet
- Economics For Pharmaceutical ManagementDocument29 pagesEconomics For Pharmaceutical ManagementTifa IstiwaNo ratings yet
- Pathfit 2: Exercise Myths and FallaciesDocument7 pagesPathfit 2: Exercise Myths and FallaciesKeen Jude CaminosNo ratings yet
- Prevention of Postpartum Psychosis PDFDocument7 pagesPrevention of Postpartum Psychosis PDFAjengNo ratings yet
- Guidelines For DNR Policies in Nursing FacilitiesDocument2 pagesGuidelines For DNR Policies in Nursing Facilitiesmichelle marquezNo ratings yet
- (Main Manuscript) Clinical Practice Guidelines For The Screening, Diagnosis, Treatment and Prevention of Neonatal SepsisDocument69 pages(Main Manuscript) Clinical Practice Guidelines For The Screening, Diagnosis, Treatment and Prevention of Neonatal Sepsiskaydee.arNo ratings yet
- Literature Review On Hypertension and DiabetesDocument8 pagesLiterature Review On Hypertension and Diabetesafmabhxbudpljr100% (1)
- M.pharm SyllabusDocument47 pagesM.pharm SyllabustusharphaleNo ratings yet
- Yoga ScopusDocument6 pagesYoga ScopusAtikah AbayNo ratings yet
- Management of The Short Bowel Syndrome in Adults - UpToDateDocument10 pagesManagement of The Short Bowel Syndrome in Adults - UpToDateyessyNo ratings yet
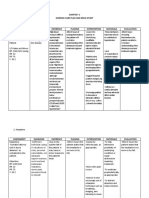
- NURSING CARE PLAN (Ineffective Breathing Pattern)Document4 pagesNURSING CARE PLAN (Ineffective Breathing Pattern)annie kolandjianNo ratings yet
- Handwashinglessonsk 6thgradeDocument25 pagesHandwashinglessonsk 6thgradeWi MaryNo ratings yet
- Postoperative Phase 2021Document56 pagesPostoperative Phase 2021Jmarie Brillantes PopiocoNo ratings yet
- Disaster Management at Site and at HospitalDocument21 pagesDisaster Management at Site and at HospitalAlmasNo ratings yet
- 封面Document5 pages封面xiaoxin zhang100% (1)
- NCCN Antiemesis Guideline 2018 v3 PDFDocument68 pagesNCCN Antiemesis Guideline 2018 v3 PDFholdonpainendsNo ratings yet
- Law and MedicineDocument2 pagesLaw and MedicineCP Ispat Unit IINo ratings yet
- BookDocument193 pagesBookFran SeptaNo ratings yet
- The Universal Health Coverage Ambition Faces A Critical Test.Document2 pagesThe Universal Health Coverage Ambition Faces A Critical Test.Brianna Vivian Rojas TimanaNo ratings yet
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayFrom EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo ratings yet
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (784)
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicFrom EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicRating: 5 out of 5 stars5/5 (1)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (96)
- Whole Body Barefoot: Transitioning Well to Minimal FootwearFrom EverandWhole Body Barefoot: Transitioning Well to Minimal FootwearRating: 4 out of 5 stars4/5 (16)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (111)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Weight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantFrom EverandWeight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantRating: 4.5 out of 5 stars4.5/5 (38)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.From EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Rating: 4.5 out of 5 stars4.5/5 (124)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- Structural Integration and Energy Medicine: A Handbook of Advanced BodyworkFrom EverandStructural Integration and Energy Medicine: A Handbook of Advanced BodyworkRating: 4 out of 5 stars4/5 (1)
- The Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandThe Yamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (19)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- Fascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)From EverandFascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)Rating: 5 out of 5 stars5/5 (3)
- The Power of Now by Eckhart Tolle: Summary and AnalysisFrom EverandThe Power of Now by Eckhart Tolle: Summary and AnalysisRating: 4.5 out of 5 stars4.5/5 (12)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingFrom EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingRating: 4.5 out of 5 stars4.5/5 (132)
- Body by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekRating: 4 out of 5 stars4/5 (38)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsFrom EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsRating: 4.5 out of 5 stars4.5/5 (7)
- Buteyko Breathing Course Manual: For use with the Advanced Buteyko CourseFrom EverandButeyko Breathing Course Manual: For use with the Advanced Buteyko CourseRating: 5 out of 5 stars5/5 (1)