You might also like
- AI in HealthcareDocument45 pagesAI in HealthcareMahmoud EladawiNo ratings yet
- Artificial Intelligence in HealthcareDocument14 pagesArtificial Intelligence in HealthcareorionUPC100% (1)
- (IJCST-V10I5P42) :mrs R Jhansi Rani, Manchinti Pavan Kumar ReddyDocument8 pages(IJCST-V10I5P42) :mrs R Jhansi Rani, Manchinti Pavan Kumar ReddyEighthSenseGroupNo ratings yet
- CFD ThesisDocument117 pagesCFD ThesisKumarecitNo ratings yet
- Artificial Intelligence in Healthcare: A Mastery: Biotechnology & Genetic Engineering Reviews April 2023Document52 pagesArtificial Intelligence in Healthcare: A Mastery: Biotechnology & Genetic Engineering Reviews April 2023panasonic92No ratings yet
- A Study On Artificial Intelligence in HCL Info SystemDocument67 pagesA Study On Artificial Intelligence in HCL Info Systempiyushsharma_231093No ratings yet
- Presentation ON Artificial Intelligence (AI)Document13 pagesPresentation ON Artificial Intelligence (AI)Aman SinghNo ratings yet
- Artificial Intelligence in HealthcareDocument27 pagesArtificial Intelligence in Healthcareava939100% (1)
- A Project Report On: Management Information System at ACC LTDDocument67 pagesA Project Report On: Management Information System at ACC LTDMadhuresh GuptaNo ratings yet
- Disease Prediction Using Machine LearningDocument10 pagesDisease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Report On Big DataDocument23 pagesReport On Big DataJasmine WaraichNo ratings yet
- Artificial Intelligence and Machine Learning For Medical ImagingDocument15 pagesArtificial Intelligence and Machine Learning For Medical ImagingHeriberto AguirreNo ratings yet
- 2020 Artificial Intelligence For Brain Diseases A Systematic ReviewDocument36 pages2020 Artificial Intelligence For Brain Diseases A Systematic ReviewMarcilio MeiraNo ratings yet
- Artificial Intelligence in MedicineDocument10 pagesArtificial Intelligence in Medicinedhiraj kumarNo ratings yet
- EtiDocument45 pagesEtiSuyash MusaleNo ratings yet
- Artificial Intelligence1Document11 pagesArtificial Intelligence1dentureNo ratings yet
- Artificial Intelligence in The Intensive CareDocument9 pagesArtificial Intelligence in The Intensive CareAlex Franco da CostaNo ratings yet
- Artificial Intelligence in Oncology: Hideyuki Shimizu - Keiichi I. NakayamaDocument9 pagesArtificial Intelligence in Oncology: Hideyuki Shimizu - Keiichi I. NakayamaNBME testNo ratings yet
- Artificial Intelligence in Oncology: Hideyuki Shimizu - Keiichi I. NakayamaDocument9 pagesArtificial Intelligence in Oncology: Hideyuki Shimizu - Keiichi I. NakayamaNBME testNo ratings yet
- Oncología IADocument9 pagesOncología IALuis Eduardo Santaella PalmaNo ratings yet
- Practical Training - Trend ResearchDocument13 pagesPractical Training - Trend ResearchMohammed AbdulreamNo ratings yet
- AI in Healthcare. Review and Prediction Case StudiesDocument11 pagesAI in Healthcare. Review and Prediction Case StudiesChannabasavaraju TumkurNo ratings yet
- J Amjmed 2017 10 035Document11 pagesJ Amjmed 2017 10 035Windu KumaraNo ratings yet
- Engineering: Guoguang Rong, Arnaldo Mendez, Elie Bou Assi, Bo Zhao, Mohamad SawanDocument11 pagesEngineering: Guoguang Rong, Arnaldo Mendez, Elie Bou Assi, Bo Zhao, Mohamad SawanNitesh LaguriNo ratings yet
- Futurehealth 9 1 75Document4 pagesFuturehealth 9 1 75christopher.lovejoy1No ratings yet
- Integrating Artificial and Human Intelligence: A Partnership For Responsible Innovation in Biomedical Engineering and MedicineDocument18 pagesIntegrating Artificial and Human Intelligence: A Partnership For Responsible Innovation in Biomedical Engineering and Medicinemaitrayee karNo ratings yet
- Research of Artificial Intelligence in MedicineDocument6 pagesResearch of Artificial Intelligence in MedicineInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AI in SurgeryDocument16 pagesAI in SurgerySuhail KhurooNo ratings yet
- Jean - Paredes@udea - Edu.co Kevin - Caicedo@udea - Edu.co Luis - Mejia5@udea - Edu.coDocument4 pagesJean - Paredes@udea - Edu.co Kevin - Caicedo@udea - Edu.co Luis - Mejia5@udea - Edu.coJean CarlosNo ratings yet
- Bjro 20190037Document8 pagesBjro 20190037GPTV AdmissionsNo ratings yet
- DownloadDocument36 pagesDownloads pradhanNo ratings yet
- Artificial Intelligance Write UpDocument4 pagesArtificial Intelligance Write UpAlishba KhalidNo ratings yet
- Theoretical Review On Artificial Intelligence Used in The Medical SectorDocument6 pagesTheoretical Review On Artificial Intelligence Used in The Medical SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S0020025524001257 MainDocument17 pages1 s2.0 S0020025524001257 MainAbdullah AbdullahNo ratings yet
- Artificial Intelegence in Biomedical EngineeringDocument34 pagesArtificial Intelegence in Biomedical EngineeringAsmaa Mohamed HassanNo ratings yet
- Applications of Artificial Intelligence in HealthcareJournal of Experimental Biology and Agricultural SciencesDocument16 pagesApplications of Artificial Intelligence in HealthcareJournal of Experimental Biology and Agricultural SciencesAditya ShuklaNo ratings yet
- Ai PDFDocument4 pagesAi PDFÖmer Faruk KaraNo ratings yet
- XAI105Document12 pagesXAI105Njehia MwauraNo ratings yet
- Use of Ai in Pharma CompaniesDocument34 pagesUse of Ai in Pharma CompaniesRishabh AnandNo ratings yet
- College of Computer and Information Sciences: Polytechnic University of The UniversityDocument15 pagesCollege of Computer and Information Sciences: Polytechnic University of The UniversityRrjer Jahj Rollon CuevasNo ratings yet
- Eng Review Paper 2Document6 pagesEng Review Paper 2HNo ratings yet
- Wa0004.Document19 pagesWa0004.Ikram EljaiNo ratings yet
- Fourcade 2019Document10 pagesFourcade 2019morganNo ratings yet
- Artificial Intelligence Full Seminar Report Way2project inDocument10 pagesArtificial Intelligence Full Seminar Report Way2project inShalini Tiwari100% (2)
- Ai White Paper UpdatedDocument21 pagesAi White Paper UpdatedRegulatonomous OpenNo ratings yet
- AI Case Study FormatDocument8 pagesAI Case Study FormatSaumen DasNo ratings yet
- How Do Machines LearnDocument22 pagesHow Do Machines LearnPMSRNo ratings yet
- ABSTRACT IEEE PAPER N Science DirectDocument3 pagesABSTRACT IEEE PAPER N Science DirectPadala HarshithaNo ratings yet
- Effects of Artificial Intelligence & Machine Learning On MankindDocument4 pagesEffects of Artificial Intelligence & Machine Learning On MankindInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Transformative Potential of AI in Healthcare - Definitions, Applications, and Navigating The Ethical Landscape and Public PerspectivesDocument31 pagesTransformative Potential of AI in Healthcare - Definitions, Applications, and Navigating The Ethical Landscape and Public Perspectivescerberus thanatosNo ratings yet
- 1 s2.0 S2414644720300208 MainDocument4 pages1 s2.0 S2414644720300208 MainWindu KumaraNo ratings yet
- Artificial Intelligence Within The Interplay Between Natural and ArtificialDocument34 pagesArtificial Intelligence Within The Interplay Between Natural and ArtificialLUZ KARIME TORRES LOZADANo ratings yet
- Medical Heart DiseaseDocument8 pagesMedical Heart Diseaseaditya bNo ratings yet
- From Blackbox To Explainable AI in Healthcare: Existing Tools and Case StudiesDocument20 pagesFrom Blackbox To Explainable AI in Healthcare: Existing Tools and Case StudiesStephanie Jane DacerNo ratings yet
- Artificial Intelligence in Clinical and Genomic DiagnosticsDocument12 pagesArtificial Intelligence in Clinical and Genomic DiagnosticsÖzge TunalıNo ratings yet
- AI in Nuclear MedicineDocument9 pagesAI in Nuclear Medicinevito calendaNo ratings yet
- Artificial Intelligence in BioinformaticsDocument4 pagesArtificial Intelligence in BioinformaticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- KBS Assignment Group7Document4 pagesKBS Assignment Group7kasitiNo ratings yet
- Exploiting Artificial Intelligence To Enhance Healthcare SectorDocument7 pagesExploiting Artificial Intelligence To Enhance Healthcare SectorSrinivas ANo ratings yet
- Neuroimaging of The Dopaminereward System in Adolescent Drug UseDocument27 pagesNeuroimaging of The Dopaminereward System in Adolescent Drug UseJenner FeijoóNo ratings yet
- Scope of Iso Standards ArticDocument9 pagesScope of Iso Standards ArticJenner FeijoóNo ratings yet
- Clarifying The Complexities of Inpatient Geriatric Rehab: February 2007Document56 pagesClarifying The Complexities of Inpatient Geriatric Rehab: February 2007Jenner FeijoóNo ratings yet
- Max N. Yoder Auth., Dr. Robert E. Clausing, Dr. Linda L. Horton, Prof. John C. Angus, Prof. Peter Koidl Eds. Diamond and Diamond-Like Films andDocument893 pagesMax N. Yoder Auth., Dr. Robert E. Clausing, Dr. Linda L. Horton, Prof. John C. Angus, Prof. Peter Koidl Eds. Diamond and Diamond-Like Films andJenner Feijoó0% (1)
- 01Document10 pages01Jenner FeijoóNo ratings yet
- Wearable Movement Sensors For Rehabilitation A Focused Reviewof Technological and Clinical AdvancesDocument13 pagesWearable Movement Sensors For Rehabilitation A Focused Reviewof Technological and Clinical AdvancesJenner FeijoóNo ratings yet
- Medical Applications of Diamond Particles and SurfacesDocument10 pagesMedical Applications of Diamond Particles and SurfacesJenner FeijoóNo ratings yet
- II Latin American Conference On Bioimpedance: Franco Simini Pedro Bertemes-Filho (Eds.)Document98 pagesII Latin American Conference On Bioimpedance: Franco Simini Pedro Bertemes-Filho (Eds.)Jenner FeijoóNo ratings yet
- Biomedical Applications of Diamond-Like Carbon (DLC) Coatings: A ReviewDocument7 pagesBiomedical Applications of Diamond-Like Carbon (DLC) Coatings: A ReviewJenner FeijoóNo ratings yet
- IBM Yachay Workshop Plan 2017 PreviousDocument4 pagesIBM Yachay Workshop Plan 2017 PreviousJenner FeijoóNo ratings yet
- DV0316 Final WebDocument44 pagesDV0316 Final WebJenner FeijoóNo ratings yet
- NIH Public AccessDocument12 pagesNIH Public AccessJenner FeijoóNo ratings yet
- Where Words Leave OffMARIAPAULADocument1 pageWhere Words Leave OffMARIAPAULAJenner FeijoóNo ratings yet
- Report These Statements: Direct Speech Indirect/Reported SpeechDocument3 pagesReport These Statements: Direct Speech Indirect/Reported SpeechJenner FeijoóNo ratings yet
- Research Paper Peer ReviewDocument4 pagesResearch Paper Peer ReviewJenner FeijoóNo ratings yet
- Report These Statements: Direct Speech Indirect/Reported SpeechDocument3 pagesReport These Statements: Direct Speech Indirect/Reported SpeechJenner FeijoóNo ratings yet
- Swaziland's Absolute Monarchy and Its Bad Working On People WellnessDocument5 pagesSwaziland's Absolute Monarchy and Its Bad Working On People WellnessJenner FeijoóNo ratings yet
- Case Study On Green MarketingDocument7 pagesCase Study On Green MarketingAnonymous WucWqwNo ratings yet
- What Are The Good Research QuestionDocument26 pagesWhat Are The Good Research Questionkavindukarunarathna100% (2)
- Sky Spark White PaperDocument7 pagesSky Spark White PaperJohn KablerNo ratings yet
- Adopter CategoriesDocument6 pagesAdopter CategoriesCaroline Mputhia100% (1)
- CatalogDocument5 pagesCataloglangtu2011No ratings yet
- MN5200 Issue1.1 APR2009Document2 pagesMN5200 Issue1.1 APR2009Roger ReisNo ratings yet
- Taking Your Pump System Efficiency To New Heights: CU 352 Multi-Pump ControllerDocument4 pagesTaking Your Pump System Efficiency To New Heights: CU 352 Multi-Pump Controllersushant moreyNo ratings yet
- PC Platform Compilers For PSS®E - Smart Grid Solutions - SiemensDocument2 pagesPC Platform Compilers For PSS®E - Smart Grid Solutions - SiemensSarah JenkinsNo ratings yet
- Quality Related QuestionsDocument22 pagesQuality Related QuestionsHotPriyu OnlyforgalsNo ratings yet
- 200+ Network Management Tools - Open Source, Free and Commercial SoftwareDocument29 pages200+ Network Management Tools - Open Source, Free and Commercial SoftwarenscintaNo ratings yet
- Oral Presentations Ormrod 2015 06Document23 pagesOral Presentations Ormrod 2015 06Miguel GonzalezNo ratings yet
- List of International and National Professional Bodies - PECDocument4 pagesList of International and National Professional Bodies - PECerumerNo ratings yet
- Acquisition (Pagtamo) Meaning-Making (Pag-Unawa) Transfer (Paglilipat)Document2 pagesAcquisition (Pagtamo) Meaning-Making (Pag-Unawa) Transfer (Paglilipat)MAY BEVERLY MORALES100% (8)
- Lista Preturi Linhai 300 2014 PDFDocument25 pagesLista Preturi Linhai 300 2014 PDFSimonaVătafuNo ratings yet
- Thyristor PDFDocument10 pagesThyristor PDFMihir HembramNo ratings yet
- LC 2539Document16 pagesLC 2539Kelly JonesNo ratings yet
- Gen Target-2017Document22 pagesGen Target-2017SundeepNo ratings yet
- CCI Control Valves For Fossil ApplicationsDocument2 pagesCCI Control Valves For Fossil ApplicationsGabrieldiazNo ratings yet
- Tesys T Ltmr100pbdDocument3 pagesTesys T Ltmr100pbdsimbamikeNo ratings yet
- Make A Project of Calculator in Visual BasicDocument9 pagesMake A Project of Calculator in Visual BasicCHITRA MINI96% (23)
- QA/QC Filling INDEX: North Gas Compression Plants (NGCP) Pipelines Index File Name File #Document3 pagesQA/QC Filling INDEX: North Gas Compression Plants (NGCP) Pipelines Index File Name File #deva017No ratings yet
- Superb 2 Aditional HeaterDocument2 pagesSuperb 2 Aditional Heaterpalle larsenNo ratings yet
- 14 Bernardo Soustruhy deDocument40 pages14 Bernardo Soustruhy deTanase Constantin0% (1)
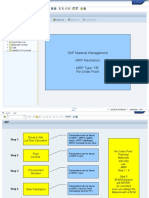
- SAP Material Management MRP Mechanics MRP Type "VB" Re-Order PointDocument15 pagesSAP Material Management MRP Mechanics MRP Type "VB" Re-Order PointmohhitNo ratings yet
- Ref: Bboneblk - SRM Beaglebone Black System Reference Manual Rev BDocument125 pagesRef: Bboneblk - SRM Beaglebone Black System Reference Manual Rev BhernangycNo ratings yet
- Subsea Pipeline Engineering (Indonesia) - ElisaDocument5 pagesSubsea Pipeline Engineering (Indonesia) - ElisaMheErdiantoNo ratings yet
- Mason Melito: EducationDocument2 pagesMason Melito: Educationapi-568517799No ratings yet
- Biochemical Oxygen DemandDocument18 pagesBiochemical Oxygen DemandUnputdownable Bishwarup100% (1)
- Canalta Parts CatalogueDocument25 pagesCanalta Parts Cataloguellando1No ratings yet
- 990 Vibration Transmitter Datasheet-141612mDocument14 pages990 Vibration Transmitter Datasheet-141612mloopkkNo ratings yet
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Defensive Cyber Mastery: Expert Strategies for Unbeatable Personal and Business SecurityFrom EverandDefensive Cyber Mastery: Expert Strategies for Unbeatable Personal and Business SecurityRating: 5 out of 5 stars5/5 (1)
- Digital Gold: Bitcoin and the Inside Story of the Misfits and Millionaires Trying to Reinvent MoneyFrom EverandDigital Gold: Bitcoin and the Inside Story of the Misfits and Millionaires Trying to Reinvent MoneyRating: 4 out of 5 stars4/5 (51)
- The Future of Geography: How the Competition in Space Will Change Our WorldFrom EverandThe Future of Geography: How the Competition in Space Will Change Our WorldRating: 4 out of 5 stars4/5 (6)
- Cyber War: The Next Threat to National Security and What to Do About ItFrom EverandCyber War: The Next Threat to National Security and What to Do About ItRating: 3.5 out of 5 stars3.5/5 (66)
- Scary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldFrom EverandScary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldRating: 4.5 out of 5 stars4.5/5 (55)
- ChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveFrom EverandChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveNo ratings yet
- Generative AI: The Insights You Need from Harvard Business ReviewFrom EverandGenerative AI: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (2)
- Chaos Monkeys: Obscene Fortune and Random Failure in Silicon ValleyFrom EverandChaos Monkeys: Obscene Fortune and Random Failure in Silicon ValleyRating: 3.5 out of 5 stars3.5/5 (111)
- ChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindFrom EverandChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindNo ratings yet
- The Intel Trinity: How Robert Noyce, Gordon Moore, and Andy Grove Built the World's Most Important CompanyFrom EverandThe Intel Trinity: How Robert Noyce, Gordon Moore, and Andy Grove Built the World's Most Important CompanyNo ratings yet
- The Infinite Machine: How an Army of Crypto-Hackers Is Building the Next Internet with EthereumFrom EverandThe Infinite Machine: How an Army of Crypto-Hackers Is Building the Next Internet with EthereumRating: 3 out of 5 stars3/5 (12)
- Solutions Architect's Handbook: Kick-start your career as a solutions architect by learning architecture design principles and strategiesFrom EverandSolutions Architect's Handbook: Kick-start your career as a solutions architect by learning architecture design principles and strategiesNo ratings yet
- AI Superpowers: China, Silicon Valley, and the New World OrderFrom EverandAI Superpowers: China, Silicon Valley, and the New World OrderRating: 4.5 out of 5 stars4.5/5 (398)
- The E-Myth Revisited: Why Most Small Businesses Don't Work andFrom EverandThe E-Myth Revisited: Why Most Small Businesses Don't Work andRating: 4.5 out of 5 stars4.5/5 (709)
- Four Battlegrounds: Power in the Age of Artificial IntelligenceFrom EverandFour Battlegrounds: Power in the Age of Artificial IntelligenceRating: 5 out of 5 stars5/5 (5)
- ChatGPT Millionaire 2024 - Bot-Driven Side Hustles, Prompt Engineering Shortcut Secrets, and Automated Income Streams that Print Money While You Sleep. The Ultimate Beginner’s Guide for AI BusinessFrom EverandChatGPT Millionaire 2024 - Bot-Driven Side Hustles, Prompt Engineering Shortcut Secrets, and Automated Income Streams that Print Money While You Sleep. The Ultimate Beginner’s Guide for AI BusinessNo ratings yet
- Reality+: Virtual Worlds and the Problems of PhilosophyFrom EverandReality+: Virtual Worlds and the Problems of PhilosophyRating: 4 out of 5 stars4/5 (24)
- The Manager's Path: A Guide for Tech Leaders Navigating Growth and ChangeFrom EverandThe Manager's Path: A Guide for Tech Leaders Navigating Growth and ChangeRating: 4.5 out of 5 stars4.5/5 (99)
- Chip War: The Quest to Dominate the World's Most Critical TechnologyFrom EverandChip War: The Quest to Dominate the World's Most Critical TechnologyRating: 4.5 out of 5 stars4.5/5 (228)
- Mini Farming: Self-Sufficiency on 1/4 AcreFrom EverandMini Farming: Self-Sufficiency on 1/4 AcreRating: 4 out of 5 stars4/5 (76)
- The Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldFrom EverandThe Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldRating: 4.5 out of 5 stars4.5/5 (107)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)From EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)No ratings yet