You might also like
- Final Exam in Topographical AnatomyDocument50 pagesFinal Exam in Topographical Anatomytastyk100% (2)
- Essential Tissue Healing of the Face and NeckFrom EverandEssential Tissue Healing of the Face and NeckRating: 5 out of 5 stars5/5 (2)
- Surgical Anatomy of The Skull BaseDocument62 pagesSurgical Anatomy of The Skull BaseNatesan_Damodara_59350% (2)
- Anatomy of The CamelDocument62 pagesAnatomy of The Cameligorgalopp100% (4)
- Maxillary NerveDocument17 pagesMaxillary NerveSharan SamyNo ratings yet
- Anatomy of The Larynx: General DescriptionDocument38 pagesAnatomy of The Larynx: General DescriptionDr-Firas Nayf Al-ThawabiaNo ratings yet
- Maxillary NerveDocument26 pagesMaxillary NerveHanaMajeedNo ratings yet
- Arterial Supply of Head and NeckDocument41 pagesArterial Supply of Head and NeckKhadija VasiNo ratings yet
- PGMEEnotes ENTnotes ENT Occasionally Asked TopicsDocument11 pagesPGMEEnotes ENTnotes ENT Occasionally Asked TopicskishorechandraNo ratings yet
- PPP LarynxDocument65 pagesPPP LarynxAnkur MittalNo ratings yet
- Osteology of MandibleDocument40 pagesOsteology of MandibleYamini RampriyaNo ratings yet
- Maxillary SinusDocument67 pagesMaxillary SinusDR. NEETI TATIYANo ratings yet
- 300 Fcps Mcq's SolvedDocument16 pages300 Fcps Mcq's SolvedFarazNo ratings yet
- Salivary GlandsDocument36 pagesSalivary GlandsNithish Reddy100% (1)
- Anatomy of The EarDocument8 pagesAnatomy of The EarDarkAngelNo ratings yet
- Presented By: DR - Satyabrata Patnaik 1 Yr P.GDocument71 pagesPresented By: DR - Satyabrata Patnaik 1 Yr P.GPingy ChompunuchNo ratings yet
- Aiims Nov 2010 Review by Tanmay MehtaDocument56 pagesAiims Nov 2010 Review by Tanmay MehtaGIST (Gujarat Institute of Science & Technology)No ratings yet
- SkullDocument48 pagesSkulldavid100% (1)
- General ENT EmergenciesDocument90 pagesGeneral ENT EmergenciesOkami P100% (1)
- Dams - Last Look - AnatomyDocument9 pagesDams - Last Look - Anatomysk100% (1)
- Tracheobronchial TreeDocument51 pagesTracheobronchial TreeravishNo ratings yet
- VENOUS DRAINAGE OoF HEAD AND NECKDocument66 pagesVENOUS DRAINAGE OoF HEAD AND NECKBhanu PraseedhaNo ratings yet
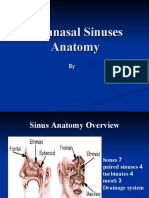
- Paranasal Sinuses AnatomyDocument55 pagesParanasal Sinuses AnatomyVictor EnachiNo ratings yet
- Headand NeckNeck and Head RadiologyDocument69 pagesHeadand NeckNeck and Head RadiologyvsignatureNo ratings yet
- Paranasal Sinus (Repaired) EntDocument48 pagesParanasal Sinus (Repaired) EntDr-Firas Nayf Al-ThawabiaNo ratings yet
- Local Anaesthesia BasicsDocument89 pagesLocal Anaesthesia BasicsDrRudra Chakraborty100% (1)
- Otorhinolaryngology 10 YearsDocument4 pagesOtorhinolaryngology 10 YearsSarbashis HazraNo ratings yet
- My Lecture NEMEC Temporal Bone CourseDocument37 pagesMy Lecture NEMEC Temporal Bone CourseAileen Delos Santos-GarciaNo ratings yet
- Maxillary ArteryDocument30 pagesMaxillary ArteryMeriam AntonyNo ratings yet
- Approach To The Dental Patient With Haematologic DiseaseDocument52 pagesApproach To The Dental Patient With Haematologic DiseaseFatima AbdallaNo ratings yet
- Nasal Septal Hematoma DrainageDocument21 pagesNasal Septal Hematoma DrainageRaja AlfatihNo ratings yet
- 1-Anatomy of NoseDocument46 pages1-Anatomy of NoseNurul Wandasari S100% (1)
- InstrumentsDocument60 pagesInstrumentsDina M100% (15)
- Surgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDocument32 pagesSurgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDr Prashant Kumar100% (1)
- Anatomy of Ear 1Document18 pagesAnatomy of Ear 1VikrantNo ratings yet
- Anatomy of LarynxDocument46 pagesAnatomy of LarynxMayur Ingale100% (1)
- Keratosis ObturansDocument2 pagesKeratosis ObturansAnish RajNo ratings yet
- Recent Advances in OtorhinolaryngologyDocument22 pagesRecent Advances in OtorhinolaryngologyInderdeep Arora100% (1)
- Basic Sinus AnatomyDocument71 pagesBasic Sinus AnatomyTalal AlanzyNo ratings yet
- Swellings of The JawDocument36 pagesSwellings of The JawSumaNo ratings yet
- Dr. Praveen PresentationDocument63 pagesDr. Praveen PresentationPraveen KumarNo ratings yet
- Intestinal Obstruction: Zeeshan Razzaq MRCS Ire, MRCS Ed, MRCS Eng Colorectal RegistrarDocument61 pagesIntestinal Obstruction: Zeeshan Razzaq MRCS Ire, MRCS Ed, MRCS Eng Colorectal Registraraini natashaNo ratings yet
- Upper Respiratory Tract AnatomyDocument61 pagesUpper Respiratory Tract Anatomyيحيى اسماعيل الجميليNo ratings yet
- Sphenopalatine Artery - SPA - LigationDocument5 pagesSphenopalatine Artery - SPA - LigationHossam Elden Helmy HaridyNo ratings yet
- CongenitalcholesteatomaDocument20 pagesCongenitalcholesteatomaMeilina Elin WardhaniNo ratings yet
- Head and Neck Arterial SystemDocument30 pagesHead and Neck Arterial SystemArifa parveenNo ratings yet
- Cholinergics and Anticholinergics DrugsDocument50 pagesCholinergics and Anticholinergics Drugsjoeyjose18No ratings yet
- Access Cavity Preparation PDFDocument94 pagesAccess Cavity Preparation PDFtomdienya100% (2)
- 2022 OlfactionDocument46 pages2022 OlfactionRam LakshmanNo ratings yet
- Mastoidectomy Indications, Types, ProcedureDocument60 pagesMastoidectomy Indications, Types, ProcedurePrasanna Datta100% (1)
- Revision Ent Instruments StyDocument3 pagesRevision Ent Instruments StylubnatawilNo ratings yet
- Gauidlines of BooksDocument37 pagesGauidlines of BooksShankar Shahi0% (1)
- Neck Mass ProtocolDocument8 pagesNeck Mass ProtocolCharlene FernándezNo ratings yet
- Lec 39 - Osteology of The SkullDocument25 pagesLec 39 - Osteology of The Skullleahbay100% (1)
- SCLP N FaceDocument43 pagesSCLP N FaceharshiniNo ratings yet
- AIPG 2005 (Dental)Document26 pagesAIPG 2005 (Dental)DENTALORG.COM100% (2)
- Thyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandThyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Logan Turner's Diseases of the Nose, Throat and EarFrom EverandLogan Turner's Diseases of the Nose, Throat and EarRating: 3.5 out of 5 stars3.5/5 (4)
- Head and Neck Cancer Care in a Pandemic: Prioritizing Safe CareFrom EverandHead and Neck Cancer Care in a Pandemic: Prioritizing Safe CareNo ratings yet
- Diseases of the Nose, Throat and Ear: For Practitioners and StudentsFrom EverandDiseases of the Nose, Throat and Ear: For Practitioners and StudentsA. Logan TurnerNo ratings yet
- Dr. El Fiky Atlas Head & Neck Anatomy Mahmoud Abd AltawabDocument79 pagesDr. El Fiky Atlas Head & Neck Anatomy Mahmoud Abd AltawabHeba Hesham100% (11)
- SkullDocument15 pagesSkullGynewNo ratings yet
- Origin InsertionDocument10 pagesOrigin InsertionPATRICE ANNE ALCOREZANo ratings yet
- Anatomy - Scalp PDFDocument3 pagesAnatomy - Scalp PDFAngel Kim100% (1)
- Pocket Atlas of Radiographic Anatomy 41-50Document10 pagesPocket Atlas of Radiographic Anatomy 41-50Ivan Alejandro Gonzalez DiazNo ratings yet
- Bones of The Skull Author Department of Oral and Maxillofacial SurgeryDocument17 pagesBones of The Skull Author Department of Oral and Maxillofacial Surgeryمدونة الأحترافNo ratings yet
- Summary of Head DR - Ihab - 3Document41 pagesSummary of Head DR - Ihab - 3ايمان عبد الشافىNo ratings yet
- Tentorial IncisuraDocument23 pagesTentorial Incisurabodeadumitru9261100% (1)
- The Foramen Magnum: Albert L. Rhoton, JR., M.DDocument39 pagesThe Foramen Magnum: Albert L. Rhoton, JR., M.Dbodeadumitru9261100% (1)
- 4 6021775789463175331Document163 pages4 6021775789463175331Muhammad Farrukh ul IslamNo ratings yet
- Temporal Bone and EarDocument76 pagesTemporal Bone and EarGuo YageNo ratings yet
- Lecture 4 Human Anatomy Dr. Mohammed WasnanDocument12 pagesLecture 4 Human Anatomy Dr. Mohammed Wasnanspo9equtabaNo ratings yet
- Operative Surgery LectureDocument115 pagesOperative Surgery LectureStar Plus OnahNo ratings yet
- Bones & Joints of Head & NeckDocument91 pagesBones & Joints of Head & NeckSalman KhanNo ratings yet
- Dural Venous Sinuses PDFDocument3 pagesDural Venous Sinuses PDFSuprit SnNo ratings yet
- Anatomy Midterm 2Document92 pagesAnatomy Midterm 2Cassandra DavisNo ratings yet
- Anatomi TelingaDocument15 pagesAnatomi Telingaerika indrajayaNo ratings yet
- SkullmethodDocument3 pagesSkullmethodJoeriz BartolomeNo ratings yet
- Retrosigmoid Intradural Suprameatal Approach To Meckel's Cave and The Middle Fossa Surgical Technique and Outcome, Tatagiba, 2000Document7 pagesRetrosigmoid Intradural Suprameatal Approach To Meckel's Cave and The Middle Fossa Surgical Technique and Outcome, Tatagiba, 2000CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- Abushara Temporal Bone Dissection ManualDocument62 pagesAbushara Temporal Bone Dissection ManualDavid3813100% (3)
- FormatDocument3 pagesFormatJo Hn Vengz0% (1)
- Aa AnatomyDocument109 pagesAa AnatomyshailendraNo ratings yet
- Ll6mn Temporal Bone CT and MRI Anatomy A Guide To 3D Volumetric AcquisitionsDocument220 pagesLl6mn Temporal Bone CT and MRI Anatomy A Guide To 3D Volumetric AcquisitionsPJ Sandhu100% (1)
- Skull ProjectionsDocument66 pagesSkull Projectionsron reteracionNo ratings yet
- Utmb-Glomus Tumors of The Temporal BoneDocument11 pagesUtmb-Glomus Tumors of The Temporal BoneAnoop SinghNo ratings yet
- Cranial CavityDocument49 pagesCranial CavityEastma MeiliNo ratings yet
- The Posterior Fossa VeinsDocument24 pagesThe Posterior Fossa Veinsbodeadumitru9261100% (2)
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (4)