You might also like
- Hope 4 Edited1Document8 pagesHope 4 Edited1Honibel CapaNo ratings yet
- PEreviewerDocument92 pagesPEreviewertherenz gerald olazoNo ratings yet
- Physical Education 11Document54 pagesPhysical Education 11Em Em Rosales OroNo ratings yet
- Basic Warm Up & Stretching Exercise: - Marching in Place - Jog in Place - High Knee - Jumping JackDocument44 pagesBasic Warm Up & Stretching Exercise: - Marching in Place - Jog in Place - High Knee - Jumping JackPorquez cantoNo ratings yet
- Lesson 4Document8 pagesLesson 4Sheena Mae Po100% (1)
- Lesson 1 Health FitnessDocument9 pagesLesson 1 Health FitnessIt's RyNo ratings yet
- Quarter 3Document29 pagesQuarter 3Ariel MohamadNo ratings yet
- Searching For The Best Exercise To Increase Height?Document1 pageSearching For The Best Exercise To Increase Height?mohiniNo ratings yet
- PE 1 Physical FitnessDocument13 pagesPE 1 Physical FitnessMa. Emely PondareNo ratings yet
- Introductio N: Chapter I - Lesson 1Document7 pagesIntroductio N: Chapter I - Lesson 1Via Mae VirtousaNo ratings yet
- H.O.P.E 3 Module 1 (Jenny Mae D. Otto Grade 12 Abm-Yen)Document8 pagesH.O.P.E 3 Module 1 (Jenny Mae D. Otto Grade 12 Abm-Yen)Jenny Mae OttoNo ratings yet
- Portfolio in Hope Group 4Document26 pagesPortfolio in Hope Group 4Mark Edwin DavidNo ratings yet
- Lesson 1Document15 pagesLesson 1Nicole LopezNo ratings yet
- Physical Education Week 1-2Document7 pagesPhysical Education Week 1-2Sarah Santiago ParalejasNo ratings yet
- Workplace Wellness: Keeping Fit at Work: Lohindren V. Adorable, MD, FPARMDocument75 pagesWorkplace Wellness: Keeping Fit at Work: Lohindren V. Adorable, MD, FPARMalexes24No ratings yet
- Pe 7 PresentationDocument70 pagesPe 7 PresentationMarj PogoyNo ratings yet
- Module 6 Physical Fitness ActivitiesDocument28 pagesModule 6 Physical Fitness ActivitiesErica IsidroNo ratings yet
- Get Fit To Apply RMDocument1 pageGet Fit To Apply RMGlobalStrategyNo ratings yet
- Field Test ApDocument3 pagesField Test Apapi-641177207No ratings yet
- Module 4-8weeksDocument8 pagesModule 4-8weeksJEWEL LUCKY LYN GUINTONo ratings yet
- Physical DimensionDocument5 pagesPhysical DimensionEddie AlcazarNo ratings yet
- Activity 2.: 1.1 Answer The Question DirectlyDocument9 pagesActivity 2.: 1.1 Answer The Question DirectlyISABEL GASESNo ratings yet
- Benefits of Intentional ExercisingDocument22 pagesBenefits of Intentional ExercisingJohn AiyenikoNo ratings yet
- Bodyweight Exercise Cardio IntervalsDocument25 pagesBodyweight Exercise Cardio IntervalsFrank Porcelli100% (3)
- What Is Muscular Endurance and Exercises To Improve ItDocument18 pagesWhat Is Muscular Endurance and Exercises To Improve ItEmbassy and NGO jobsNo ratings yet
- Kanupriya TrainingDocument32 pagesKanupriya TrainingVishesh AgarwalNo ratings yet
- Self-Assessment-Body Composition and Cardiovascular EnduranceDocument43 pagesSelf-Assessment-Body Composition and Cardiovascular EnduranceCyrus BustoneraNo ratings yet
- Pe and Health Mod 1Document9 pagesPe and Health Mod 1Krismark IsraelNo ratings yet
- PE NotesDocument17 pagesPE NotesMaylannie TauyanNo ratings yet
- Resistance TrainingDocument164 pagesResistance TrainingPratima Patel100% (9)
- Mapeh Presentation Group 4Document16 pagesMapeh Presentation Group 4Bon Suriz L. LimpiadaNo ratings yet
- Fitness Tests: Measure Your Health and Physical AbilityDocument54 pagesFitness Tests: Measure Your Health and Physical AbilityNeil Jasper B. DucutNo ratings yet
- Developing Components of Health-Related FitnessDocument28 pagesDeveloping Components of Health-Related Fitnesstoni tesoroNo ratings yet
- Physical Education - Ppt. Lesson 3Document28 pagesPhysical Education - Ppt. Lesson 3toni tesoroNo ratings yet
- Philippine Society of Endocrinology and MetabolismDocument23 pagesPhilippine Society of Endocrinology and MetabolismNinz MaeNo ratings yet
- Spear ModuleDocument2 pagesSpear ModuleAllysa Nhor RetonioNo ratings yet
- Pe 10 Q4 Module 7Document10 pagesPe 10 Q4 Module 7KyleNo ratings yet
- Just WalkDocument42 pagesJust WalkVenkatesh Bharadwaj SrinivasanNo ratings yet
- Fitness TestDocument4 pagesFitness TestorthomedNo ratings yet
- HOPE 1 Lesson 2.2 Learning TaskDocument2 pagesHOPE 1 Lesson 2.2 Learning TaskColein FranleighNo ratings yet
- How To Lose Belly Fat and Gain Butt Muscle LivestrongDocument1 pageHow To Lose Belly Fat and Gain Butt Muscle Livestrongjogiyo3154No ratings yet
- Concepts and Components of Physical Fitness: Pe01 Module 03Document63 pagesConcepts and Components of Physical Fitness: Pe01 Module 03chingNo ratings yet
- Physical Activity: A Tu Salud ¡Sí Cuenta! Educational ModuleDocument44 pagesPhysical Activity: A Tu Salud ¡Sí Cuenta! Educational ModuletmarsiccNo ratings yet
- Hope 2 Module 2 3rd QDocument11 pagesHope 2 Module 2 3rd QLynette LicsiNo ratings yet
- Physical Education (1ST Sem - Module 1 Dance)Document18 pagesPhysical Education (1ST Sem - Module 1 Dance)mary roseNo ratings yet
- Par QDocument5 pagesPar QJomar CarabotNo ratings yet
- One Hundred Push Ups Training ProgramDocument19 pagesOne Hundred Push Ups Training ProgramMihalis PitsiNo ratings yet
- Active and Pain Free PregnancyDocument30 pagesActive and Pain Free PregnancyNimra AzharNo ratings yet
- Beginner Calisthenic S: WWW - Oldschool-CalisthenicDocument18 pagesBeginner Calisthenic S: WWW - Oldschool-CalisthenicGamer's PrideNo ratings yet
- The Body-Balance Workout by Marc LebertDocument5 pagesThe Body-Balance Workout by Marc Lebertwaxguru100% (1)
- Chair Based Exercises For Older AdultsDocument38 pagesChair Based Exercises For Older AdultsPascha ParamurthiNo ratings yet
- Moms Into Fitness Ab Rehab Exercise GuideDocument19 pagesMoms Into Fitness Ab Rehab Exercise GuideAditya ArdianiNo ratings yet
- Script For Brochure PresentationDocument7 pagesScript For Brochure PresentationAllycel ChiucoNo ratings yet
- Exercises For Better Sexual StaminaDocument9 pagesExercises For Better Sexual StaminaAkifNo ratings yet
- Hope1 Module5 q1 v5 Final VersionDocument12 pagesHope1 Module5 q1 v5 Final VersionBlink G.No ratings yet
- Handouts For PFTDocument8 pagesHandouts For PFTJamessNo ratings yet
- PEH1 - 1st Semester (Midterm)Document5 pagesPEH1 - 1st Semester (Midterm)Francine Chalcy CanlasNo ratings yet
- Creating the Ultimate Martial Artist: Learn the Secrets and Tricks Used By the Best Professional Martial Artists and Coaches to Improve Your Fitness, Conditioning, Nutrition, and Mental ToughnessFrom EverandCreating the Ultimate Martial Artist: Learn the Secrets and Tricks Used By the Best Professional Martial Artists and Coaches to Improve Your Fitness, Conditioning, Nutrition, and Mental ToughnessNo ratings yet
- PAR-Q Physical Activity Readiness QuestionnaireDocument5 pagesPAR-Q Physical Activity Readiness QuestionnaireSarah DecenaNo ratings yet
- The 15-Minute Standing Abs Workout Plan: Ten Simple Core Exercises to Firm, Tone, and Tighten Your MidsectionFrom EverandThe 15-Minute Standing Abs Workout Plan: Ten Simple Core Exercises to Firm, Tone, and Tighten Your MidsectionNo ratings yet
- Design 6 Major Plate No.1 ARCHITECTURALDocument4 pagesDesign 6 Major Plate No.1 ARCHITECTURALJayson PobarNo ratings yet
- ADIME Note: Hypertension: AssessmentDocument2 pagesADIME Note: Hypertension: AssessmentJasperl Niña Malabuyoc100% (1)
- 174 - 13 UREA PDF - 28-Euro Procedure SheetDocument2 pages174 - 13 UREA PDF - 28-Euro Procedure SheetP VijayaNo ratings yet
- Naskah Pdgk4304 Tmk2 1Document2 pagesNaskah Pdgk4304 Tmk2 1Gina Lis15No ratings yet
- Marathon Race StrategiesDocument13 pagesMarathon Race StrategiesJay WilkinsonNo ratings yet
- Understanding HypoglycemiaDocument8 pagesUnderstanding Hypoglycemianurizzah_885541No ratings yet
- The Nutrition: ChallengeDocument12 pagesThe Nutrition: ChallengeFrancis Joseph C. ArongNo ratings yet
- Food and Nutrition: Paper 6065/01 TheoryDocument7 pagesFood and Nutrition: Paper 6065/01 Theorymstudy123456No ratings yet
- Kligler Iron AgarDocument3 pagesKligler Iron AgarOsama BakheetNo ratings yet
- Casas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionDocument2 pagesCasas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionCasas, Jo-an Pauline A.No ratings yet
- Protocolo Da BombaDocument52 pagesProtocolo Da BombaEmerson SaNo ratings yet
- Lesson 3 - ProteinsDocument28 pagesLesson 3 - ProteinslaarnieNo ratings yet
- Drew DreilingDocument2 pagesDrew DreilingMicNo ratings yet
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDocument67 pagesDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyNo ratings yet
- SampleDocument30 pagesSampleazlizaNo ratings yet
- 07 23 14Document24 pages07 23 14grapevineNo ratings yet
- Magnesium L Threonate For Depression and Anxiety PDFDocument6 pagesMagnesium L Threonate For Depression and Anxiety PDFRocco LamponeNo ratings yet
- Keto Chicken ParmesanDocument1 pageKeto Chicken ParmesanJW Custom LeatherNo ratings yet
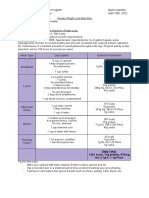
- Obesity Weight Loss Meal PlanDocument1 pageObesity Weight Loss Meal Planapi-607536364No ratings yet
- Food and Nutrition - 1Document29 pagesFood and Nutrition - 1cheny presbiteroNo ratings yet
- Hematology, Immunology & OncologyDocument10 pagesHematology, Immunology & Oncologyjennaaahhh67% (3)
- Approach To Severe Acute MalnutritionDocument49 pagesApproach To Severe Acute MalnutritionAlbertina Aipinge NandjilaNo ratings yet
- Heavy Metal ProtocolDocument2 pagesHeavy Metal ProtocolvytoNo ratings yet
- The Dnt15: A Shortened Version of The Diabetes Numeracy Test (DNT)Document13 pagesThe Dnt15: A Shortened Version of The Diabetes Numeracy Test (DNT)zomorda kammounNo ratings yet
- Cinemark Nutritional Information: POPCORN (Finished Popcorn W/ Butteral Salt, Canola Oil)Document4 pagesCinemark Nutritional Information: POPCORN (Finished Popcorn W/ Butteral Salt, Canola Oil)Felipe YepesNo ratings yet
- SOC101 Research PaperDocument30 pagesSOC101 Research PaperJannatul Ferdousi PrïtyNo ratings yet
- 5 Keys To Exploding Numbers in Weight Room PDFDocument11 pages5 Keys To Exploding Numbers in Weight Room PDFGarmint Hung100% (2)
- Estrogenic Foods To AvoidDocument2 pagesEstrogenic Foods To AvoidAlfred YangaoNo ratings yet
- Reebok RL900 User ManualDocument28 pagesReebok RL900 User ManualMeriNo ratings yet
- Chatper 7. Nursing Care of The Older Adult in Chronic Illness ModuleDocument17 pagesChatper 7. Nursing Care of The Older Adult in Chronic Illness ModuleAriane-Gay Cristobal DuranNo ratings yet