International Journal of Advanced Engineering Research and Science (IJAERS) [Vol -6, Issue-5, May- 2019]
https://dx.doi.org/10.22161/ijaers.6.5.31 ISSN: 2349-6495(P) | 2456-1908(O)
Prevalence of Mental Disorder in Adults and
Elderly
Arielly Rayanne Amaral Alves Santana1, Beatriz Rocha Sousa2, Arianna
Oliveira Santana Lopes2, Maria Clara Pereira Teixeira1, Neuza Ana Fagundes
Moreira1, Ísis Silveira Dias2, Ravena Madalena Nascimento 2, Felipe Oliveira
Bittencourt1,2, Iaggo Raphael David2 and Stenio Fernando Pimentel
Duarte1,2,3,4.*
1 Independent Faculty of the Northeast – Bahia, Brazil.
2 Public Health Foundation of Vitória da Conquista – Bahia, Brazil.
3 Faculty of Technologies and Sciences – Bahia, Brazil.
4 Faculty of Santo Agostinho – Bahia, Brasil
*Corresponding author
Rua Dely Viera Silva 675, Felicia - CEP: 45055-605. Vitória da Conquista, Bahia, Brazil.
Abstract— These functional loses can be quantified at the I. INTRODUCTION
population level by multiplying the prevalence of those According to data from the World Health
disorders by the average level of disability associated Organization, in 2015 the estimated prevalence of people
with them, it is estimated that 50 million years of life are with common mental disorders was of 4,4% for
lost because of these disabling morbidities. It is a cross- depression and 3,6% for anxiety. Representing 322
sectional and descriptive epidemiological research. The million of people affected by the morbidities [1,2]. Since
sample consisted of 1356 individuals. For the evaluation many people experience both conditions simultaneously
on mental disorders - stress, anxiety and depression - When people experience both conditions simultaneously
BECK’s inventory and Lipp’s stress questionnaire were it is called comorbidities (diseases that coexist in the same
utilized. It was verified that adults are more stressed subject), that can be more serious versions of the diseases.
(64.5%) than the elderly (60.1%). Regarding the anxiety The prevalence rates vary according to age, with a peak in
and depression levels, adults had higher diagnostic older adulthood (above 7,5% among women aged 55-75
numbers, with 27% and 17,8%, respectively, against years and above 5,5% among man the same age group)
24,9% and 16,4% among the elderly. With high global [1,3].
prevalence, being considered a public health problem. Common mental disorders can lead to
It’s worth pointing out that in our finding, the highest considerable health and organic functioning loses. These
prevalence was of stress in adult population, however, it functional loses can be quantified at the populational level
was verified in data analysis a linearity in relation to the by multiplying the prevalence of those disorders by the
proportions between adults and the elderly, leading to the average level of disability associated with them, it is
understanding that adults with mental disorders tend to estimated that 50 million years of life are lost because of
be elders with mental disorders. The incentive of healthy these disabling morbidities [4,5]. Beyond that, researchers
habits, a favorable environment for the practice of leisure have shown that people with some sort of mental disorder
and social life, are responsible factors for the most have a higher mortality level than their peers without
effective prevention in order to reduce the morbidity clinical presentation [6–8].
burden of mental disorders. This is a multifactorial psychosomatic disorder,
Keywords— Mental Disorders. Major Depressive that needs time to be installed and is therefore considered
Disorder, Anxiety, Psychological Stress, Epidemiology. a chronic disease, without a well-defined etiology, that is
more prevalent in adults and the elderly than in children
and adolescents [9]. The risk factors are diverse, ranging
from socioeconomic background, genetic and
www.ijaers.com Page | 240
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol -6, Issue-5, May- 2019]
https://dx.doi.org/10.22161/ijaers.6.5.31 ISSN: 2349-6495(P) | 2456-1908(O)
physiological dysfunctions [10] to pre-existing diseases. Incomplete
151 56,8
Directly influencing the onset of mental disorder [11]. Elementary
These factors add up, leading to a favorable Complete Elementary 18 6,8
environment to the emergence of mental disorder [12,13]. Incomplete High
13 4,9
Its morbidity is perceived at the moment the person is School
Scholarity 266
incapable of performing their instrumental activities of Complete High
34 12,8
daily life, being limited to restricted and inmate School
environments and little contact with other people, having Incomplete College 3 1,1
a direct impact on health and life quality [14, 15]. Complete College 12 4,5
In view of the above, given the magnitude and No scholarity 35 13,2
impact of mental disorders, this study has the goal of Type of Public 210 94,2
223
identifying the prevalence of common mental disorders in education Private 13 5,8
adults and elderly from the city of Vitória da Conquista, Source: Own research 2018.
Bahia.
Table 2 – Adult Characterization.
II. METHODOLOGY
This is a cross-sectional and descriptive Variables n % Total
epidemiological research, realized in the city of Vitória da (n)
Conquista - BA, located in the Southwest of Bahia, Brazil Male 288 28,6
(geographical coordinates latitude -14º 53' and longitude - Gender 1006
Female 718 71,4
40º 48'). The city is part of the Southwest economic Single 485 48,5
region and is 509 km away from the capital - Salvador. It Marital Married 446 44,6
has a Gross Domestic Product (GDP) of 3.469 billion and 1001
Status Divorced 59 5,9
a Human Development Index (HDI) of 0.708. This is a Windower 11 1,1
cut from a larger project, entitled “Epidemiological Yes 675 67,2
profile of obesity in the city of Vitória da Conquista/BA”. Occupation 1005
No 330 32,8
The sample consisted of 1356 subjects, of whom 350 B 49 5,5
were elderly and 1006 were adults, from both genders. All Social C 270 30
participants were educated about the risks and benefits 901
Class D 440 48,8
and all signed the Informed Consent Form (ICF). E 141 15,6
To obtain the data the socioeconomic Incomplete 119 12,1
questionnaire was used for the variables: gender, Elementary
scholarity, type of education, marital status, social class, Complete 32 3,2
occupation. It was part of the characterization of the Elementary
sample and will be presented in table 1 and 2. Incomplete 57 5,8
High School
Table 1 – Elder Characterization. Complete 234 23,7
Scholarity 987
High School
Variables n % Total Incomplete 302 30,6
(n) College
Male 108 30,9 Complete 217 22,0
Gender 350
Female 242 69,1 College
Single 54 15,9 No 26 2,6
Marital Married 169 49,9 scholarity
339
Status Divorced 29 8,6 Type of Public 732 75,3
Widower 87 25,7 972
Education Private 240 24,7
Yes 49 14 Source: Own research 2018.
Occupation 350
No 301 86
B 1 0,3 To obtain the evaluation of mental disorders -
C 24 8,3 stress, anxiety and depression - BECK’s anxiety
Social Class 288
D 164 56,9 inventory questionnaire (BAI - Beck Anxiety inventory),
E 99 34,4 BECK’s depression inventory (BDI - Beck Depression
www.ijaers.com Page | 241
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol -6, Issue-5, May- 2019]
https://dx.doi.org/10.22161/ijaers.6.5.31 ISSN: 2349-6495(P) | 2456-1908(O)
Inventory) andLipp’s stress questionnaire were utilized III. RESULTS AND DISCUSSION
[16-18]. In our study, we obtained 1356 individuals,
The BAI is a self-report scale, consisting of 21 adults and seniors from both genders, some of whom
items, that measures the intensity of anxiety and contains didn’t answer all questionings and therefore we had lost
descriptive claims of anxiety symptoms. The items should in some of the questionings, however, these loses don’t
be evaluated by the subject with reference to himself, in a diminish the importance of the presented data.
scale of 4 points, according to the Portuguese version As shown in sample characterization table 1 and
manual of the Beck Scales, which reflects levels of 2, in our study the majority of the collected individuals
increasing severity of each symptom as: 1) “Absolutely were adults and the female audience was higher in both
no”; 2) “Lightly: did not bother me much”; 3) age categories. The majority were married. Regarding
“Moderately: It was very unpleasant, but I could bear it”; work, the majority of adults claimed to work, which was
4) “Severely: I could hardly bear it” [19, 20]. inversely verified among the elderly, something we
The BDI is a self-report scale, consisting of 21 predicted, since a good part of the elderly are retired [23].
items, each with four alternatives, implying increasing Both groups have similar social classes , which shows a
degrees of severity of depression, with scores ranging linearity among the adults who are of classes B, C, D and
from 0 to 3. The items were selected based on E in relation to aging. Adults had a higher average
observations and reports of symptoms and attitudes in scholarly level than the elderly, whose majority had an
psychiatric patients with depressive disorders and weren’t incomplete elementary school. Most of them also claimed
chosen to reflect any theory of depression in particular to have studied in public education institutions.
[21]. According to the World Health Organization, all
The Lipp’s Inventory of Symptoms of Stress for the factors that characterize the sample are also
Adults (ISSL) intends to identify symptoms of stress in a considered important risk factors for the onset of chronic
objective manner according to the symptomatology the diseases and among them, mental disorders (stress,
patient presents, evaluating the types of symptoms anxiety, depression) [1, 23, 24]. The socioeconomic
(somatic or psychological) and the phase he’s in. It profile of the subject reflects their basics characteristics,
presents a four-phase stress model (alert, resistance, near having a strong influence on their way of life [25, 26].
exhaustion and exhaustion) based initially on Selye’s Good health also requires a good educational level, as it is
three-phase model (alert, resistance and exhaustion), but verified in literature that people who have a low level of
doesn’t invalidate it, being only an improvement of the scholarity are also more likely to have chronic diseases
first proposed model [22]. [19, 27]. As well as staying in a lower social class, having
The treatment and tabulation of the data were only cheaper and high in fat food available. Their leisure
realized with the aid of the Excel program and the is generally reduced either by low economic power or by
descriptive analysis, presenting the percentage and the environmental factors [28–30].
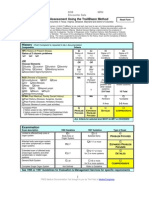
“n” of the sample, was made with the assistance of In our samples, the number of adults was higher
Statistical Package for Social Sciences- SPSS, version than that of the elderly, but in relation to mental disorders,
25.0 software. The participants were educated on the the two populations presented similar values in
utilized methods according to the Resolution 466/12 percentage. It was verified that adults are more stressed
(National Health Council), which is composed of (64.5%) than the elderly (60.1%). Regarding the anxiety
international research documents that involve human and depression levels, adults had higher diagnostic
beings. It should be noted that the project was approved numbers, with 27% and 17,8%, respectively, against
by the Research Ethics Committee of the Independent 24,9% and 16,4% among the elderly. The high number of
Faculty of the Northeast (Legal Advice nº 1.859.545). adults compared to those of the elderly may justify the
higher prevalence of mental disorders in adults.
Table 3. Prevalence of Stress, Anxiety and Depression in adults and elders.
Adults Elders
Variables n % n %
Without 292 35,5 110 39,1
Stress
With 530 64,5 171 60,1
www.ijaers.com Page | 242
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol -6, Issue-5, May- 2019]
https://dx.doi.org/10.22161/ijaers.6.5.31 ISSN: 2349-6495(P) | 2456-1908(O)
Without 587 73,0 208 75,1
Anxiety
With 217 27,0 69 24,9
Without 699 82,2 249 83,6
Depression
With 151 17,8 49 16,4
Source: Own research, 2018.
Linearity in relation to the number of adults and effective prevention in order to reduce the morbidity
elderly with a mental disorder is evident. However, there burden of mental disorders.
is a major difference between mental disorders and
mental illness [31]. The use of the term “illness” implies REFERENCES
an elaborate etiology in which symptoms arise from a [1] World Health Organization. Depression and other
common pathogenic pathway, while the term “mental common mental disorders: global health estimates.
disorder” refers to a syndromic constellation of symptoms World Heal Organ 2017:1–24. doi:CC BY-NC-SA
that fit empirically, often for unknown reasons [14,31]. 3.0 IGO.
Demonstrating that these psychosomatic [2] Pinto JC, Martins P, Pinheiro TB, Oliveira AC.
symptoms are multifactorial and can lead to greater Ansiedade, Depressão e Stresse: Um Estudo com
problems during the course of organic aging [32]. JovensAdultos e AdultosPortugueses.
Demonstrating that the care for the reduction of mental PsicolSaúdeDoenças2015;16:148–63.
disorders must be immediate, always aiming at a better doi:10.15309/15psd160202.
quality of life and healthier habits [31, 33]. [3] Lund C, Brooke-Sumner C, Baingana F, Baron
The magnitude of these environmental factors EC, Breuer E, Chandra P, et al. Social
and their unequal distribution among the population could determinants of mental disorders and the
provide a unique perspective. Regarding poverty, studies Sustainable Development Goals: a systematic
have explored the reversibility of brain changes upon review of reviews. The Lancet Psychiatry
improvements on economic status, unraveling the 2018;5:357–69. doi:10.1016/S2215-
potential role of relative and absolute poverty and 0366(18)30060-9.
examining how poverty could modulate the underlying [4] Wang Z, Lin C, Ma B, Bian Y. Activities of daily
biology of mental disorders [3]. living in hospitalized patients with mental
Stress from day to day, social and family life, disorders. Asian J Psychiatr2018;32:77–8.
work, financial issues, have been satisfactory bridges to doi:10.1016/ j.ajp.2017.11.038.
achieve success in correlating with the symptoms of [5] Mograbi DC, Morris RG, Fichman HC, Faria CA,
anxiety and also depression, showing how they may Sanchez MA, Ribeiro PCC, et al. The impact of
intervene in physical and, especially, psychological dementia, depression and awareness on activities
wellbeing of individuals. Today, mental disorders are of daily living in a sample from a middle-income
being considered as one of the biggest disabling country. Int J Geriatr Psychiatry 2018;33:807–13.
morbidities in the world [1, 34]. Thus, there is a great doi:10.1002/gps.4765.
need for directing attention to these diseases in order to [6] Walker ER, McGee RE, Druss BG. Mortality in
mitigate negative impacts, modeling preventive health Mental Disorders and Global Disease Burden
actions [15]. Implications. JAMA Psychiatry 2015;72:334.
doi:10.1001/ jamapsychiatry.2014.2502.
IV. FINAL CONSIDERATIONS [7] Diab DL, Yerian L, Schauer P, Kashyap SR,
Therefore, it’s verified that mental disorders Lopez R, Hazen SL, et al. Cytokeratin 18
don’t have simple etiology elucidated. With high global Fragment Levels as a Noninvasive Biomarker for
prevalence, being considered a public health problem. It’s Nonalcoholic Steatohepatitis in Bariatric Surgery
worth pointing out that in our finding, the highest Patients. Clin Gastroenterol Hepatol2008;6:1249–
prevalence was of stress in adult population, however, it 54. doi:10.1016/ j.cgh.2008.07.016.
was verified in data analysis a linearity in relation to the [8] Chesney, Edward, Goodwind, Guy M., Fazel,
proportions between adults and the elderly, leading to the Seena. Risks of all-cause and suicide mortality in
understanding that adults with mental disorders tend to be mental disorders: a meta-review. World Psychiatry
elders with mental disorders. The incentive of healthy 2014;13:153– 60.
habits and a favorable environment for the practice of [9] Crossley NA, Alliende LM, Ossandon T,
leisure and social life are responsible factors for the most Castañeda CP, González-Valderrama A,
www.ijaers.com Page | 243
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol -6, Issue-5, May- 2019]
https://dx.doi.org/10.22161/ijaers.6.5.31 ISSN: 2349-6495(P) | 2456-1908(O)
Undurraga J, et al. Imaging Social and [20] Ferreira AH, Godoy PBG, Oliveira NRC de, Diniz
Environmental Factors as Modulators of Brain RAS, Diniz REAS, Padovani R da C, et al.
Dysfunction: Time to Focus on Developing Non- Investigação da ansiedade, depressão e qualidade
Western Societies. Biol Psychiatry CognNeurosci de vidaempacientesportadores de osteoartrite no
Neuroimaging 2019;4:8–15. joelho: um estudocomparativo. Rev Bras
doi:10.1016/ j.bpsc.2018.09.005. Reumatol2015;55:434–8.
[10] Iwata K. Mitochondrial Involvement in Mental doi:10.1016/ j.rbr.2015.03.001.
Disorders; Energy Metabolism, Genetic, and [21] Rantanen AT, Korkeila JJA, Löyttyniemi ES,
Environmental Factors. vol. 1916. New York, NY: Saxén UKM, Korhonen PE. Awareness of
Springer New York; 2019. doi:10.1007/978-1- hypertension and depressive symptoms: a cross -
4939-8994-2. sectional study in a primary care population. Scand
[11] Keller MC. Evolutionary Perspectives on Genetic J Prim Health Care 2018;0:1–6.
and Environmental Risk Factors for Psychiatric doi:10.1080/02813432.2018.1499588.
Disorders. Ssrn 2018:1–23. doi:10.1146/annurev- [22] Lima ACR, Oliveira AB. FatoresPsicológicos da
clinpsy-050817-084854. Obesidade e AlgunsApontamentosSobre a
[12] Kim DJ, Davis EP, Sandman CA, Glynn L, Sporns TerapiaCognitivo-Comportamental. Mudanças -
O, O’Donnell BF, et al. Childhood poverty and the Psicol Da Saúde2016;24:1–14.
organization of structural brain connectome. doi:10.15603/2176-1019/ mud.v24n1p 1-14.
Neuroimage 2019;184:409–16. [23] Silva L, Sousa BR, David IR, Silva DS, Soares D,
doi:10.1016/ j.neuroimage.2018.09.041. Gonçalves PF, et al. New Perspectives for Age
[13] Panahi S, Tremblay A. Sedentariness and Health: Groupings for Older People. Int J Dev Res
Is Sedentary Behavior More Than Just Physical 2018;08:22462–6.
Inactivity? Front Public Heal 2018;6:1–7. [24] Cohen BE, Edmondson D, Kronish IM. State of
doi:10.3389/fpubh.2018.00258. the art review: Depression, stress, anxiety, and
[14] Jones, P.J; Heren, A.; McNally R. A network cardiovascular disease. Am J
theory of mental disorders. World Psychiatry Hypertens2015;28:1295–302.
2017;16:5–13. doi:10.1002/wps.20375. doi:10.1093/ajh/hpv047.
[15] Pridmore S. Mental disorder and suicide: A faulty [25] Pedersen SS, Andersen CM. Minding the heart:
connection. Aust N Z J Psychiatry 2015;49:18–20. Why are we still not closer to treating depression
doi:10.1177/0004867414548904. and anxiety in clinical cardiology practice? Eur J
[16] Rodrigues N, Arruda JM, Aguiar MO, David IR, PrevCardiol2018;25:244–6.
Dias ÍS, Teles MF, et al. Research Article doi:10.1177/2047487317744367.
Anxiolytics Use of Association and Alcohol With [26] Leal JS, Almeida E, Raphael I, Dantas D. Quality
Beck Anxiety Diagnosis. Int J Curr Res of life for practitioners of strength of two cities in
2018;10:74259–62. southern Brazil n.d.:52–65.
[17] Arruda M, Brito MF, Rodrigues KN, Soares D, [27] Ulrich-Lai YM, Fulton S, Wilson M, Petrovich G,
Paula MB De, Carol B, et al. EVALUATION OF Rinaman L. Stress exposure, food intake and
DEPRESSION AND QUALITY OF LIVING IN emotional state. Stress 2015;18:381–99.
ELDERLY EVALUATION OF DEPRESSION doi:10.3109/10253890.2015.1062981.
AND QUALITY OF LIVING IN ELDERLY. Int J [28] Landmann-Szwarcwald C, Macinko J. A
Curr Res 2018:2016– 8. panorama of health inequalities in Brazil. Int J
[18] Dias S, Ramos S, Mara M, Gonçalves C, Paula A, Equity Health 2016;15:174. doi:10.1186/s12939-
Dutra R, et al. EVALUATING THE LEVEL OF 016-0462-1.
PHYSICAL ACTIVITY AND COMMON [29] Chan RR, Larson JL. Meditation Interventions for
MENTAL DISORDERS IN ELDERLY PEOPLE Chronic Disease Populations. J Holist
WHO USE CHRONIC MEDICINES. Int J Dev Nurs2015;33:351–65.
Res 2018;08:24313–7. doi:10.1177/0898010115570363.
[19] Serra RD, Dinato SLM e, Caseiro MM. Prevalence [30] Botha E, Gwin T, Purpora C. The effectiveness of
of depressive and anxiety symptoms in medical mindfulness based programs in reducing stress
students in the city of Santos. J Bras experienced by nurses in adult hospital settings: a
Psiquiatr2015;64:213–20. doi:10.1590/0047- systematic review of quantitative evidence
2085000000081. protocol. JBI Database Syst Rev Implement
www.ijaers.com Page | 244
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol -6, Issue-5, May- 2019]
https://dx.doi.org/10.22161/ijaers.6.5.31 ISSN: 2349-6495(P) | 2456-1908(O)
Reports 2015;13:21–9. doi:10.11124/jbisrir-2015-
2380.
[31] Spitzer RL, Endicott J, Micoulaud Franchi JA.
Medical and mental disorder: Proposed definition
and criteria. Ann Med Psychol (Paris)
2018;176:656–65. doi:10.1016/j.amp.2018.07.004.
[32] Małyszczak K, Rymaszewska J. Depression and
anxiety in cardiovascular disease. Kardiol Pol
2016;74:603– 9. doi:10.5603/KP.a2016.0063.
[33] Fulford KWM. Mental Disorder, Concept of. vol.
3. Second Edi. Elsevier Inc.; 2012.
doi:10.1016/b978-0-12-373932-2.00156-3.
[34] Krueger RF, Eaton NR. Transdiagnostic factors of
mental disorders. World Psychiatry 2015;14:27–9.
doi:10.1002/wps.20175.
www.ijaers.com Page | 245
You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaDocument4 pagesThe Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaIJAERS JOURNALNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Facing Dengue and Malaria As A Public Health Challenge in BrazilDocument6 pagesFacing Dengue and Malaria As A Public Health Challenge in BrazilIJAERS JOURNALNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Climatic Rhythms and Prevalence of Malaria in The Municipality of Sinende in Northern BeninDocument8 pagesClimatic Rhythms and Prevalence of Malaria in The Municipality of Sinende in Northern BeninIJAERS JOURNALNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Beef Cattle Farmers' Economic Behavior in The Minahasa Tenggara Regency, IndonesiaDocument7 pagesBeef Cattle Farmers' Economic Behavior in The Minahasa Tenggara Regency, IndonesiaIJAERS JOURNALNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Enhancing Cybersecurity: The Power of Artificial Intelligence in Threat Detection and PreventionDocument6 pagesEnhancing Cybersecurity: The Power of Artificial Intelligence in Threat Detection and PreventionIJAERS JOURNALNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Analysis of The Thermal Behavior of Masonry Concrete Block With Internal Natural Element CoatingDocument11 pagesAnalysis of The Thermal Behavior of Masonry Concrete Block With Internal Natural Element CoatingIJAERS JOURNALNo ratings yet
- The Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaDocument4 pagesThe Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaIJAERS JOURNALNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Impacts On The Mental Health of Professionals in A Prisonal System in Alagoas During The Covid-19 PandemicDocument7 pagesImpacts On The Mental Health of Professionals in A Prisonal System in Alagoas During The Covid-19 PandemicIJAERS JOURNALNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Business Logistics and The Relationship With Organizational SuccessDocument4 pagesBusiness Logistics and The Relationship With Organizational SuccessIJAERS JOURNALNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- VCO Rancidity Analysis Refers To Fermentation Time That Produced by Gradual Heating MethodDocument6 pagesVCO Rancidity Analysis Refers To Fermentation Time That Produced by Gradual Heating MethodIJAERS JOURNAL100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Breastfeeding and Factors Associated With The Prevention of Childhood Obesity: An Integrative Literature ReviewDocument16 pagesBreastfeeding and Factors Associated With The Prevention of Childhood Obesity: An Integrative Literature ReviewIJAERS JOURNALNo ratings yet
- Study of The Extraction Process of The Pleurotus Citrinopileatus Mushroom and Evaluation of The Biological Activity of The ExtractDocument8 pagesStudy of The Extraction Process of The Pleurotus Citrinopileatus Mushroom and Evaluation of The Biological Activity of The ExtractIJAERS JOURNALNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Constructed Wetlands: Technology For Removing Drug Concentration From WaterDocument12 pagesConstructed Wetlands: Technology For Removing Drug Concentration From WaterIJAERS JOURNALNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Associativism As Strategy of Reaching Territorial Rights, Programs, Projects and Public Policies of Rural Development: The Case of The São Francisco Do Mainã Community, Manaus, AMDocument9 pagesAssociativism As Strategy of Reaching Territorial Rights, Programs, Projects and Public Policies of Rural Development: The Case of The São Francisco Do Mainã Community, Manaus, AMIJAERS JOURNALNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Water Quality Assessment Using GIS Based Multi-Criteria Evaluation (MCE) and Analytical Hierarchy Process (AHP) Methods in Yenagoa Bayelsa State, NigeriaDocument11 pagesWater Quality Assessment Using GIS Based Multi-Criteria Evaluation (MCE) and Analytical Hierarchy Process (AHP) Methods in Yenagoa Bayelsa State, NigeriaIJAERS JOURNALNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Childhood/ Pediatric Cancer: Nursing Care in Oncopediatrics With A Central Focus On HumanizationDocument12 pagesChildhood/ Pediatric Cancer: Nursing Care in Oncopediatrics With A Central Focus On HumanizationIJAERS JOURNALNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Design and Building of Servo Motor Portable Coconut Peller MachineDocument5 pagesDesign and Building of Servo Motor Portable Coconut Peller MachineIJAERS JOURNALNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Modeling of Geological and Geophysical Data, Onshore Field of Potiguar Basin, Northeastern BrazilDocument5 pagesModeling of Geological and Geophysical Data, Onshore Field of Potiguar Basin, Northeastern BrazilIJAERS JOURNALNo ratings yet
- Komla Uwolowudu Amegna: International Journal of Advanced Engineering Research and Science (IJAERS)Document9 pagesKomla Uwolowudu Amegna: International Journal of Advanced Engineering Research and Science (IJAERS)IJAERS JOURNALNo ratings yet
- Process Sequence Optimization and Structural Analysis of Nanoscale Heterostructure Using Compound Semiconductors AlAsSb/In0.59Ga0.41As/GaAs0.53Sb0.47Document5 pagesProcess Sequence Optimization and Structural Analysis of Nanoscale Heterostructure Using Compound Semiconductors AlAsSb/In0.59Ga0.41As/GaAs0.53Sb0.47IJAERS JOURNALNo ratings yet
- Morphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaDocument9 pagesMorphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaIJAERS JOURNALNo ratings yet
- Morphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaDocument9 pagesMorphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaIJAERS JOURNALNo ratings yet
- Sociodemographic and Clinical Profile of Women With Uterine Cervical Cancer Attended in An Oncological Hospital in The State of Acre, BrazilDocument9 pagesSociodemographic and Clinical Profile of Women With Uterine Cervical Cancer Attended in An Oncological Hospital in The State of Acre, BrazilIJAERS JOURNALNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Multiprofessional Care For A Patient With Gestational DiabetesDocument12 pagesMultiprofessional Care For A Patient With Gestational DiabetesIJAERS JOURNALNo ratings yet
- Humanization in Undergraduate Medical Education: The Brazilian Learner's PerspectiveDocument12 pagesHumanization in Undergraduate Medical Education: The Brazilian Learner's PerspectiveIJAERS JOURNALNo ratings yet
- Mining and Its Impacts On Environment and Health With Special Reference To Ballari District, Karnataka, IndiaDocument7 pagesMining and Its Impacts On Environment and Health With Special Reference To Ballari District, Karnataka, IndiaIJAERS JOURNALNo ratings yet
- Association of Bacterial Vaginosis To Atypia in Squamous Cells of The CervixDocument15 pagesAssociation of Bacterial Vaginosis To Atypia in Squamous Cells of The CervixIJAERS JOURNALNo ratings yet
- Does Blended Learning Approach Affect Madrasa Students English Writing Errors? A Comparative StudyDocument12 pagesDoes Blended Learning Approach Affect Madrasa Students English Writing Errors? A Comparative StudyIJAERS JOURNALNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Psychologist's Role in The Process of Listening To Children Victims of Sexual Violence in Legal ProceedingsDocument8 pagesThe Psychologist's Role in The Process of Listening To Children Victims of Sexual Violence in Legal ProceedingsIJAERS JOURNALNo ratings yet
- Assessment of The Risk of Cardiovascular Diseases and Its Relationship With Heart Rate Variability in Physically Active and Sedentary IndividualsDocument13 pagesAssessment of The Risk of Cardiovascular Diseases and Its Relationship With Heart Rate Variability in Physically Active and Sedentary IndividualsIJAERS JOURNALNo ratings yet
- Goal attainment theory-based empowerment improves health of older adultsDocument9 pagesGoal attainment theory-based empowerment improves health of older adultsJASTINE JOY PEREZNo ratings yet
- Research Article: Factors Affecting The Occurrence of Out-of-Hospital Sudden Cardiac ArrestDocument7 pagesResearch Article: Factors Affecting The Occurrence of Out-of-Hospital Sudden Cardiac ArrestHandrian RahmanNo ratings yet
- Successful 10-Second One-Legged Stance Performance Predicts Survival in Middle-Aged and Older Individuals 2022Document7 pagesSuccessful 10-Second One-Legged Stance Performance Predicts Survival in Middle-Aged and Older Individuals 2022Felipe MunizNo ratings yet
- Research PaperDocument4 pagesResearch PaperJian Padasas JimenezNo ratings yet
- Braddoms 2020 - Capitulo 10 - Protesis Eeii y MarchaDocument38 pagesBraddoms 2020 - Capitulo 10 - Protesis Eeii y MarchaSergio Navarrete VidalNo ratings yet
- Cognitive Therapy Improves Sleep DisordersDocument12 pagesCognitive Therapy Improves Sleep DisordersJulian PintosNo ratings yet
- Trailblazer Medicare Audit ToolDocument4 pagesTrailblazer Medicare Audit Tooladultmedicalconsultants100% (10)
- Chapter 37: Dialysis Decisions in The Elderly Patient With Advanced CKD and The Role of Nondialytic TherapyDocument8 pagesChapter 37: Dialysis Decisions in The Elderly Patient With Advanced CKD and The Role of Nondialytic Therapykhangha.ptNo ratings yet
- Chung 2014Document6 pagesChung 2014Retno ManggalihNo ratings yet
- Icu-Related Dysphagia Epidemiology, Pathophysiology, Diagnostics and TreatmentDocument6 pagesIcu-Related Dysphagia Epidemiology, Pathophysiology, Diagnostics and TreatmentLuis De jesus SolanoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Medically Unexplained Symptoms BAHRIDocument58 pagesMedically Unexplained Symptoms BAHRIAhmed AlabwabiNo ratings yet
- Learning Module in NCM 114Document28 pagesLearning Module in NCM 114JIMENEZ, TRISHA MARIE D.No ratings yet
- Assessing The Relationship Between Anxiety Levels and Panic Attacks Among The Youth in ShimlaDocument52 pagesAssessing The Relationship Between Anxiety Levels and Panic Attacks Among The Youth in ShimlaAni RudhNo ratings yet
- Silabus KDK Dengan MingguDocument24 pagesSilabus KDK Dengan MingguIin Prima FitriahNo ratings yet
- Clinical Practice Guideline For Schizophrenia and Incipient Psychotic DisorderDocument9 pagesClinical Practice Guideline For Schizophrenia and Incipient Psychotic DisorderFranco MascayanoNo ratings yet
- RCGP GP Consultation CurriculumDocument20 pagesRCGP GP Consultation CurriculumAn TonNo ratings yet
- Ansu 265 466Document8 pagesAnsu 265 466BlayneNo ratings yet
- RCDSO Guidelines Diagnosis and Management of TMDDocument12 pagesRCDSO Guidelines Diagnosis and Management of TMDdoctorlupuNo ratings yet
- NeurologiaDocument216 pagesNeurologiaPietro BracagliaNo ratings yet
- MSF OCA NCD Guidelines v3 2018Document139 pagesMSF OCA NCD Guidelines v3 2018PepepottNo ratings yet
- Attention Deficit Hyperactivity Disorder in Nepal: A Qualitative StudyDocument9 pagesAttention Deficit Hyperactivity Disorder in Nepal: A Qualitative StudyNijan KhatiwadaNo ratings yet
- 0849370655Document450 pages0849370655Luisa LopezNo ratings yet
- Anesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFDocument11 pagesAnesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFtiaraleshaNo ratings yet
- Shining The Light On Eating Disorders Incidence Prognosis and Profiling of Patients in Primary and Secondary Care National Data Linkage StudyDocument8 pagesShining The Light On Eating Disorders Incidence Prognosis and Profiling of Patients in Primary and Secondary Care National Data Linkage StudyarijanaNo ratings yet
- The Association Between Internet Addiction and Psychiatric Disorder A Review of The Literature 2012 European PsychiatryDocument8 pagesThe Association Between Internet Addiction and Psychiatric Disorder A Review of The Literature 2012 European PsychiatryElena CrisNo ratings yet
- E Learning General OncoGeriatrics PDFDocument46 pagesE Learning General OncoGeriatrics PDFMartina BonillaNo ratings yet
- Hospital Readmission in General Medicine Patients, A Prediction ModelDocument9 pagesHospital Readmission in General Medicine Patients, A Prediction ModelchairunnisyaNo ratings yet
- Bm33 11 Co Infectionsandco Morbidities Report enDocument15 pagesBm33 11 Co Infectionsandco Morbidities Report enUtary Rezki SakinahNo ratings yet
- Primer On Nephrology 2022Document1,713 pagesPrimer On Nephrology 2022Maievp53100% (1)
- Neuropsychology of PTSDDocument352 pagesNeuropsychology of PTSDAmar NiksicNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)