You might also like
- DHP W. TableDocument21 pagesDHP W. Tablejenika studiesNo ratings yet
- Proximal BicepsDocument23 pagesProximal BicepsPrabath ChinthakaNo ratings yet
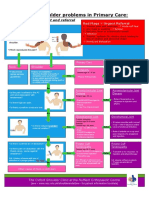
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertNo ratings yet
- Rheumatology: - Red Flag DiagnosisDocument3 pagesRheumatology: - Red Flag DiagnosisEmilee Joice Rochelle MalutoNo ratings yet
- Handout Lat Elbow Pain PDFDocument47 pagesHandout Lat Elbow Pain PDFgemichan26No ratings yet
- Shoulder ProblemsDocument1 pageShoulder ProblemsulaNo ratings yet
- GP Assessment of The Shoulder: Keith Littlebury MSC Grad Dip Phys Extended Scope Physiotherapist Camden Cats ServiceDocument29 pagesGP Assessment of The Shoulder: Keith Littlebury MSC Grad Dip Phys Extended Scope Physiotherapist Camden Cats ServiceapriliatnaNo ratings yet
- Musculoskeletal Trauma RSIJPKDocument41 pagesMusculoskeletal Trauma RSIJPKPegyNo ratings yet
- Scfe PDFDocument39 pagesScfe PDFMuhammad Tabish SaleemNo ratings yet
- Traction Is A Mechanical Force Applied To TheDocument3 pagesTraction Is A Mechanical Force Applied To TheAshley Franceska CansanayNo ratings yet
- Orthopaedic Emergencies AndreDocument49 pagesOrthopaedic Emergencies AndreLusi MunawarohNo ratings yet
- Examination of Knee PainDocument40 pagesExamination of Knee PainEmme BihNo ratings yet
- MSK AllDocument113 pagesMSK AllMuhammed Elgasim100% (1)
- McEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFDocument2 pagesMcEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFRamesh SinghNo ratings yet
- Common Sports Injuries: Ukris Gunadham, MD, FRCOST Department of Orthopaedics Trang HospitalDocument71 pagesCommon Sports Injuries: Ukris Gunadham, MD, FRCOST Department of Orthopaedics Trang HospitalMohammed SaqoorNo ratings yet
- Quade Lindsay October 3 A1 and B1-Evaluation of The Painful Shoulder - 1Document47 pagesQuade Lindsay October 3 A1 and B1-Evaluation of The Painful Shoulder - 1Pratibha YadavNo ratings yet
- Anatomy Case Correlate: "Shoulder Pain"Document24 pagesAnatomy Case Correlate: "Shoulder Pain"Uloko ChristopherNo ratings yet
- Degenerative in ShoulderDocument49 pagesDegenerative in Shoulderari rujatiNo ratings yet
- Spinal Cord Injury Oleh DR Cok SP - OtDocument50 pagesSpinal Cord Injury Oleh DR Cok SP - OtPipit ArikaNo ratings yet
- Some Issues in Spine Imaging: DR Greg CowderoyDocument156 pagesSome Issues in Spine Imaging: DR Greg Cowderoysubramanyam LAKSHMIPURAMNo ratings yet
- Spine Disease and Fractures For StudentsDocument79 pagesSpine Disease and Fractures For StudentsAbdullah MohdNo ratings yet
- High Velocity Manipulation TechniquesDocument2 pagesHigh Velocity Manipulation TechniquesBhargavaNo ratings yet
- Lower Back Pain: DR Robert Ramcharan MBBS, Frcsed, DM (Neurosurgery) NeurosurgeonDocument69 pagesLower Back Pain: DR Robert Ramcharan MBBS, Frcsed, DM (Neurosurgery) NeurosurgeonShimmering MoonNo ratings yet
- Low Back Pain: Kyaw Htet AgDocument51 pagesLow Back Pain: Kyaw Htet AgKyaw Htet AungNo ratings yet
- Pathway For Shoulder PainDocument1 pagePathway For Shoulder Painrizk86No ratings yet
- To Refer or Not To ReferDocument56 pagesTo Refer or Not To Refer健康生活園Healthy Life GardenNo ratings yet
- Red Flag: MSK Services Pathway - Shoulder PathologyDocument11 pagesRed Flag: MSK Services Pathway - Shoulder PathologyMuhammed ElgasimNo ratings yet
- Case Report EmmaDocument34 pagesCase Report EmmaAnwar Mo SajaNo ratings yet
- Lumber SpineDocument37 pagesLumber SpineSerena AlshafeeNo ratings yet
- Approach To Shoulder InstabilityDocument63 pagesApproach To Shoulder InstabilitySubarna PaudelNo ratings yet
- Acute OsteomyelitisDocument7 pagesAcute OsteomyelitisAhmad Syahmi YZNo ratings yet
- 1-22 Osteoporosis & Hip PainDocument79 pages1-22 Osteoporosis & Hip PaintarikeopsNo ratings yet
- 3-22 Slides Arthritis-CIS2016 CoxDocument42 pages3-22 Slides Arthritis-CIS2016 CoxbAmNo ratings yet
- Week 8 Category 2Document4 pagesWeek 8 Category 2api-468093714No ratings yet
- Section 1: General OrthopaedicsDocument25 pagesSection 1: General OrthopaedicsAditio PranandaNo ratings yet
- ..1 Midterm Shoulder RehabilitationDocument7 pages..1 Midterm Shoulder RehabilitationELIZABETH GRACE AMADORNo ratings yet
- SpineInjury - Dr. PuntodewaDocument41 pagesSpineInjury - Dr. PuntodewaWindy MentariNo ratings yet
- The Musculoskeletal System: An OverviewDocument46 pagesThe Musculoskeletal System: An OverviewDavid L KriegelNo ratings yet
- Basic Fracture ManagementDocument107 pagesBasic Fracture ManagementPrabath ChinthakaNo ratings yet
- 4 - Orthopedic HistoryDocument7 pages4 - Orthopedic HistoryshaifNo ratings yet
- OsteoarthritisDocument29 pagesOsteoarthritisfizhazhiNo ratings yet
- Cowderoy 180329152104Document156 pagesCowderoy 180329152104subramanyam LAKSHMIPURAMNo ratings yet
- Knee ExaminationDocument14 pagesKnee ExaminationAsimNo ratings yet
- 3D Regional Rheumatic PainDocument50 pages3D Regional Rheumatic PainIkhsan Amadea9969No ratings yet
- NCM 116 - Musculoskeletal Conditions Part 3Document21 pagesNCM 116 - Musculoskeletal Conditions Part 3Gabrielle Frances FernandezNo ratings yet
- High Ankle SprainDocument10 pagesHigh Ankle Sprainferd dinanNo ratings yet
- Lesson - Elbow Region Examination and EvaluationDocument8 pagesLesson - Elbow Region Examination and EvaluationJULIANE MAE BALANGNo ratings yet
- Club Foot PDFDocument54 pagesClub Foot PDFBelle Sakunrat SarikitNo ratings yet
- Femur FractureDocument19 pagesFemur FractureMadx VNo ratings yet
- Subaxial Cervical Spine TruamaDocument46 pagesSubaxial Cervical Spine TruamaWasim R. IssaNo ratings yet
- Orthopedic ConditionsDocument11 pagesOrthopedic ConditionsErin Hoffmann100% (3)
- The Hip: Therapeutic Exercise 2 Lino Linford BangayanDocument91 pagesThe Hip: Therapeutic Exercise 2 Lino Linford BangayanLino Linford Yu Bangayan100% (1)
- Osteomyelitis - Kaye WilkinsDocument50 pagesOsteomyelitis - Kaye WilkinsWindy MentariNo ratings yet
- 4-Orthopedic History Taking PDFDocument25 pages4-Orthopedic History Taking PDFDivya GNo ratings yet
- Trauma Spinal Wates Dr. WRDocument68 pagesTrauma Spinal Wates Dr. WRLanlan LesmanaNo ratings yet
- Spinal Stenosis: Jung U. Yoo, M.DDocument52 pagesSpinal Stenosis: Jung U. Yoo, M.DGabriel KlemensNo ratings yet
- Pain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowFrom EverandPain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowRating: 1 out of 5 stars1/5 (1)
- Distal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDistal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The DR Sebi Diet A Healing Journey 100 - DR Sebi Research CenterDocument159 pagesThe DR Sebi Diet A Healing Journey 100 - DR Sebi Research CenterDEEJAY NERVSNo ratings yet
- Process of ReproductionDocument18 pagesProcess of ReproductionAxielvie BabateNo ratings yet
- WIDALDocument17 pagesWIDALNasti YL HardiansyahNo ratings yet
- Case 1Document1 pageCase 1younggirldavidNo ratings yet
- POLYPHASE 678 SdsDocument8 pagesPOLYPHASE 678 SdsMarianna JassoNo ratings yet
- BPOC Si SDR MetabolicDocument29 pagesBPOC Si SDR MetabolicMarta DumitracheNo ratings yet
- IDocument14 pagesIjasdeepkaurnagra100% (1)
- Exam Questions For Students 1-350Document26 pagesExam Questions For Students 1-350Komal valve100% (2)
- GROUPER Medan WorkshopDocument232 pagesGROUPER Medan WorkshopNia Prajnya SyailendraNo ratings yet
- Advertising Solutions From Oxford University PressDocument12 pagesAdvertising Solutions From Oxford University PressGeorge FelintoNo ratings yet
- Feco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)Document133 pagesFeco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)TekletsadikNo ratings yet
- What Are The Parts of A Nursing Diagnosis? Know How To Write An Appropriate Nursing DiagnosisDocument9 pagesWhat Are The Parts of A Nursing Diagnosis? Know How To Write An Appropriate Nursing DiagnosisNoah ClevengerNo ratings yet
- 3a DnDestiny - BestiaryoftheWilds - v0.5Document46 pages3a DnDestiny - BestiaryoftheWilds - v0.5HectorNo ratings yet
- Lectures in PediatricsDocument217 pagesLectures in PediatricsPachiappan NatarajanNo ratings yet
- Outline of The Controversial Issue ParagraphDocument2 pagesOutline of The Controversial Issue ParagraphLeo WangNo ratings yet
- JCI Fact Sheet CCPCDocument1 pageJCI Fact Sheet CCPCAna Sofìa Sanchez CastilloNo ratings yet
- Hospital Team Match These Following Jobs Below With Their Definition A B ADocument2 pagesHospital Team Match These Following Jobs Below With Their Definition A B AIlhamNo ratings yet
- The SoundMind Meditation SystemDocument6 pagesThe SoundMind Meditation SystemDunga AlexandraNo ratings yet
- Active Management of LabourDocument4 pagesActive Management of LabourHytham AtiaNo ratings yet
- Q3 2019 Management Review SHEQ Presentation-1Document23 pagesQ3 2019 Management Review SHEQ Presentation-1Warren KabichiNo ratings yet
- General Dentistry Informed Consent FormDocument3 pagesGeneral Dentistry Informed Consent FormNishtha KumarNo ratings yet
- Group 01: Articles For ReviewDocument4 pagesGroup 01: Articles For ReviewPrincess Krenzelle BañagaNo ratings yet
- Nestle Inc.,: Submitted By: Ruazol, Jayrus A. Flores Kenneth R. Tepait, Mark Kenjie R. Aragon, Howell TDocument10 pagesNestle Inc.,: Submitted By: Ruazol, Jayrus A. Flores Kenneth R. Tepait, Mark Kenjie R. Aragon, Howell THowell AragonNo ratings yet
- Argumentative Essay: Is Meat Murder?Document2 pagesArgumentative Essay: Is Meat Murder?Petra Gabriella PatakiNo ratings yet
- Early Diagnosis of Childhood Cancer: © Pan American Health OrganizationDocument45 pagesEarly Diagnosis of Childhood Cancer: © Pan American Health Organizationcindy8127No ratings yet
- Aug28..signage Prohibiting Detention of Patients Is A Must For Hospitals and ClinicsDocument1 pageAug28..signage Prohibiting Detention of Patients Is A Must For Hospitals and Clinicspribhor2No ratings yet
- Three Components of Energy ExpenditureDocument26 pagesThree Components of Energy ExpenditureDustin HarrisonNo ratings yet
- SDS Car Shampoo US enDocument13 pagesSDS Car Shampoo US enoptionality458No ratings yet
- BonvieDocument1 pageBonvieTony Peterz KurewaNo ratings yet
- Observership ApplicationDocument3 pagesObservership ApplicationMatheus AzevedoNo ratings yet