You might also like
- Maternity and Pediatric Nursing 3rd EditionDocument347 pagesMaternity and Pediatric Nursing 3rd EditionTaylor Talley80% (15)
- 5 Weight LossDocument41 pages5 Weight LossTasniiem KhmbataNo ratings yet
- Post Test AtlsDocument6 pagesPost Test Atlsnurul huda85% (62)
- Principles of Molecular Medicine - J. Larry Jamenson - Humana Press - 1998Document1,144 pagesPrinciples of Molecular Medicine - J. Larry Jamenson - Humana Press - 1998BOC100% (1)
- American Board of Family Medicine: TTT SAMPLE TTTDocument148 pagesAmerican Board of Family Medicine: TTT SAMPLE TTTAbdulrhman AlruwiliNo ratings yet
- Pathophysiology of Peptic Ulcer Disease: Pylori InfectionDocument2 pagesPathophysiology of Peptic Ulcer Disease: Pylori InfectionJim Christian Ellaser100% (1)
- ENT - Topical Past Papers (2005-2020) - 1Document39 pagesENT - Topical Past Papers (2005-2020) - 1medical notesNo ratings yet
- A Case of ThalassemiaDocument10 pagesA Case of ThalassemiaAnas MohiuddinNo ratings yet
- Case Study TyphoidDocument10 pagesCase Study TyphoidArchana Sahu100% (3)
- Case Study On Head InjuryDocument58 pagesCase Study On Head InjuryISLAMIC KNOWLEDGE BASED ON TRULY HADIS50% (2)
- Dialysis Center in BPDHDocument29 pagesDialysis Center in BPDHXien Cadiz100% (5)
- Kawasaki DiseaseDocument38 pagesKawasaki DiseaseJayson CabarceNo ratings yet
- Case PresentationDocument43 pagesCase Presentationkayal100% (1)
- PNC PresentationDocument42 pagesPNC PresentationRijoy ZuzadNo ratings yet
- INTUSSUSCEPTIONDocument43 pagesINTUSSUSCEPTIONValarmathi100% (3)
- Complete - Gordon's Functional Health Pattern - Group 4Document7 pagesComplete - Gordon's Functional Health Pattern - Group 4TaanzNo ratings yet
- Rds CPDocument31 pagesRds CPSwati Sharma100% (1)
- Kawasaki Disease-Case-Study LATEST CHANGESDocument24 pagesKawasaki Disease-Case-Study LATEST CHANGESJesse James Advincula Edjec100% (7)
- I. INTRODUCTION Cesarean Section Is A SurgicalDocument62 pagesI. INTRODUCTION Cesarean Section Is A SurgicalLuis R. Dela Cruz86% (7)
- Get Ready to Get Pregnant: Your Complete Prepregnancy Guide to Making a Smart and Healthy BabyFrom EverandGet Ready to Get Pregnant: Your Complete Prepregnancy Guide to Making a Smart and Healthy BabyRating: 3.5 out of 5 stars3.5/5 (14)
- Case VaricellaDocument39 pagesCase VaricellaRatna Kurnia NingsihNo ratings yet
- Pediatric AGE EditedDocument4 pagesPediatric AGE EditedMichael VillavertNo ratings yet
- Pedia Clinics Case Marfans 18yo Epigastric Pain Dyspnea RHDDocument9 pagesPedia Clinics Case Marfans 18yo Epigastric Pain Dyspnea RHDTrisNo ratings yet
- CP Acute and Chornic DiseaseDocument27 pagesCP Acute and Chornic DiseaseTopeshwar TpkNo ratings yet
- Precept2 - Cardio BlockDocument9 pagesPrecept2 - Cardio BlockMary Christine IlangaNo ratings yet
- Sample Pediatric History 2Document2 pagesSample Pediatric History 2Chelsea PialagoNo ratings yet
- Acut - Lymphoid LukemiaDocument28 pagesAcut - Lymphoid LukemiaAya AlntshNo ratings yet
- February 12 SGDDocument7 pagesFebruary 12 SGDRONALDO CUANo ratings yet
- Generalclinics12 151014131450 Lva1 App6891Document16 pagesGeneralclinics12 151014131450 Lva1 App6891Amanina Zahraa ZainolNo ratings yet
- Pedia PT 4 PMH FinalDocument6 pagesPedia PT 4 PMH FinalJoherNo ratings yet
- Broncho Pnuemonia MEDICALDocument9 pagesBroncho Pnuemonia MEDICALArchana SahuNo ratings yet
- Disjag CKDDocument21 pagesDisjag CKDselvi destariaNo ratings yet
- DH NisaDocument36 pagesDH Nisahielmy scootNo ratings yet
- Precept1 - Pulmo BlockDocument15 pagesPrecept1 - Pulmo BlockMary Christine IlangaNo ratings yet
- Dengue Hemorrhagic Fever: Dian Rahayu Ningtias 030.14.052 Pembimbing: Dr. Andri Firdaus, Sp.ADocument35 pagesDengue Hemorrhagic Fever: Dian Rahayu Ningtias 030.14.052 Pembimbing: Dr. Andri Firdaus, Sp.Adirani rahmanNo ratings yet
- Pertinent Positive Pertinent Negative Weight Loss (41 KG To 37 KG in 1-2 Months) Productive Cough Double Vision Lymph Node Swelling Fatigue Bruising Syncope Body Tremors DyspneaDocument8 pagesPertinent Positive Pertinent Negative Weight Loss (41 KG To 37 KG in 1-2 Months) Productive Cough Double Vision Lymph Node Swelling Fatigue Bruising Syncope Body Tremors DyspneaMary Christine IlangaNo ratings yet
- Timeline: October 7 2017 October 8 2017 October 12 2017 October 13 2017Document43 pagesTimeline: October 7 2017 October 8 2017 October 12 2017 October 13 2017ireneaureliaNo ratings yet
- HirschprungsDocument6 pagesHirschprungsasdfNo ratings yet
- LaporanDocument9 pagesLaporanDaleKadalNo ratings yet
- Cerebral Palsy Amdekar SirDocument42 pagesCerebral Palsy Amdekar SirVishalSapateNo ratings yet
- CASE AppDocument25 pagesCASE AppreshianeNo ratings yet
- Pedia NowDocument9 pagesPedia NowJim Christian EllaserNo ratings yet
- Longcase Ira New FixDocument44 pagesLongcase Ira New FixMuhammad Rifani KnNo ratings yet
- Final Case (Postpartum)Document14 pagesFinal Case (Postpartum)KimJohnSanchoManeroNo ratings yet
- Enteric FeverDocument30 pagesEnteric FeverShivam MalikNo ratings yet
- Nurul Sylvana Long Case Baru-1 (1) - 1Document42 pagesNurul Sylvana Long Case Baru-1 (1) - 1Abdurrahman HasanuddinNo ratings yet
- CP MatterDocument11 pagesCP MatterShikhar SinghNo ratings yet
- Jeanne Lloraine R. Fiel Date&Time: November 23, 2020 at 5:00 P.M. Informant: Mother % Reliability: 95%Document6 pagesJeanne Lloraine R. Fiel Date&Time: November 23, 2020 at 5:00 P.M. Informant: Mother % Reliability: 95%Jeanne Lloraine FielNo ratings yet
- Pedia HX Seizure 1Document25 pagesPedia HX Seizure 1Amer Hussein DomadoNo ratings yet
- Case Study CSDocument21 pagesCase Study CSThessa Lonica GarciaNo ratings yet
- 3 Care PlanDocument25 pages3 Care PlanKhushbu KatariaNo ratings yet
- Tugas Kelompok 1 PemDocument28 pagesTugas Kelompok 1 PemKaslan ElrealNo ratings yet
- Case Report AnemiaDocument54 pagesCase Report AnemiahaekalNo ratings yet
- Askep Atrial Septal DefectDocument20 pagesAskep Atrial Septal DefectDar YanaNo ratings yet
- Clinico Social CaseDocument6 pagesClinico Social CaseNakshatra ReddyNo ratings yet
- Learning Objective:: ST THDocument34 pagesLearning Objective:: ST THYPramudiyaNo ratings yet
- NP J Gonzales FinalDocument56 pagesNP J Gonzales FinalAra_Ongaco_8894No ratings yet
- Patient'S Name: ND STDocument8 pagesPatient'S Name: ND STayunisallehNo ratings yet
- Longcase Fix TB MilierDocument42 pagesLongcase Fix TB MilierAbdurrahman HasanuddinNo ratings yet
- Gordon'S Functional Health Pattern: Client ProfileDocument6 pagesGordon'S Functional Health Pattern: Client ProfileRainier Rhett ConchaNo ratings yet
- Nursing History I. Client's ProfileDocument6 pagesNursing History I. Client's ProfileLc RamboyongNo ratings yet
- Demographic Data: Social HistoryDocument13 pagesDemographic Data: Social HistoryplokatzNo ratings yet
- Case Melita FixedDocument40 pagesCase Melita FixedMelita Aditya SariNo ratings yet
- Nutrition Care ProcessDocument20 pagesNutrition Care ProcessAdrianNo ratings yet
- Lanuza Demo LabDocument57 pagesLanuza Demo LabShaina MillanNo ratings yet
- Lanuza Demo LabDocument57 pagesLanuza Demo LabShaina MillanNo ratings yet
- Chief Complaint History of Present Illnes Relates To The Chief Complain or ProblemDocument2 pagesChief Complaint History of Present Illnes Relates To The Chief Complain or ProblemImukNo ratings yet
- Pedia Case PreDocument3 pagesPedia Case PreMikkelo SususcoNo ratings yet
- Anak Stase UinDocument38 pagesAnak Stase UinSaisabelaPrmNo ratings yet
- Clinical PresentationsDocument37 pagesClinical PresentationsJim Christian EllaserNo ratings yet
- Pathophysiology of Acute GastroenteritisDocument2 pagesPathophysiology of Acute GastroenteritisArlan AbraganNo ratings yet
- Patient 1 GS, VS, Neuro ExamDocument1 pagePatient 1 GS, VS, Neuro ExamJim Christian EllaserNo ratings yet
- Diagnostic ExamsDocument1 pageDiagnostic ExamsJim Christian EllaserNo ratings yet
- Causes EffectsDocument1 pageCauses EffectsJim Christian EllaserNo ratings yet
- Intrauterine Fetal DemiseDocument7 pagesIntrauterine Fetal DemisesalamredNo ratings yet
- General Objective:: JERIEL Pregnancy-Related BleedingDocument6 pagesGeneral Objective:: JERIEL Pregnancy-Related BleedingJim Christian EllaserNo ratings yet
- Pathophysiology PUD 2Document2 pagesPathophysiology PUD 2Jim Christian EllaserNo ratings yet
- Differentials Cap-MrDocument3 pagesDifferentials Cap-MrJim Christian EllaserNo ratings yet
- Differential DiagnosisDocument2 pagesDifferential DiagnosisJim Christian EllaserNo ratings yet
- Diagnosis: Congestive Heart Failure Pathophysiology: Differential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsDocument7 pagesDiagnosis: Congestive Heart Failure Pathophysiology: Differential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsJim Christian EllaserNo ratings yet
- Diagnostic Tests: Community-Acquired PneumoniaDocument23 pagesDiagnostic Tests: Community-Acquired PneumoniaJim Christian EllaserNo ratings yet
- CBDDocument2 pagesCBDJim Christian EllaserNo ratings yet
- SGD #3 Date of Consult: December 11, 2020: Divine Word Hospital Department of Obstetrics and GynecologyDocument2 pagesSGD #3 Date of Consult: December 11, 2020: Divine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserNo ratings yet
- Pediatric Clinics PT 1 (Meningitis)Document10 pagesPediatric Clinics PT 1 (Meningitis)Jim Christian EllaserNo ratings yet
- SGD #1 Date of Consult: December 5, 2020: Divine Word Hospital Department of Obstetrics and GynecologyDocument1 pageSGD #1 Date of Consult: December 5, 2020: Divine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserNo ratings yet
- SGD #6 Date of Consult: December 19, 2020: Divine Word Hospital Department of Obstetrics and GynecologyDocument3 pagesSGD #6 Date of Consult: December 19, 2020: Divine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserNo ratings yet
- Hypoxic-Ischemic EncephalopathyDocument34 pagesHypoxic-Ischemic EncephalopathyJim Christian EllaserNo ratings yet
- CaseDocument2 pagesCaseJim Christian EllaserNo ratings yet
- Divine Word Hospital Department of Obstetrics and GynecologyDocument1 pageDivine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserNo ratings yet
- Divine Word Hospital Department of Obstetrics and GynecologyDocument1 pageDivine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserNo ratings yet
- SGD #4 Date of Consult: October 21, 2020: Divine Word Hospital Department of Obstetrics and GynecologyDocument2 pagesSGD #4 Date of Consult: October 21, 2020: Divine Word Hospital Department of Obstetrics and GynecologyRose Ann RaquizaNo ratings yet
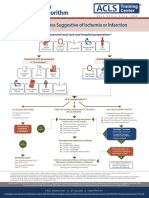
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserNo ratings yet
- PT 01Document14 pagesPT 01Jim Christian EllaserNo ratings yet
- Dengue DifferentialsDocument5 pagesDengue DifferentialsJim Christian EllaserNo ratings yet
- Ramel Pedro D. Tadong Post-Graduate Intern Department of PediatricsDocument5 pagesRamel Pedro D. Tadong Post-Graduate Intern Department of PediatricsJim Christian EllaserNo ratings yet
- Typhoid Fever PathophysiologyDocument1 pageTyphoid Fever PathophysiologyJim Christian EllaserNo ratings yet
- Dengue DifferentialsDocument5 pagesDengue DifferentialsJim Christian EllaserNo ratings yet
- SURGERY Hemorrhoids PEDocument3 pagesSURGERY Hemorrhoids PEJim Christian EllaserNo ratings yet
- Askep CKDDocument55 pagesAskep CKDyuli ariyantiNo ratings yet
- hw499 Unit5 3 Assignment Massage Therapy Rachel MartinezDocument9 pageshw499 Unit5 3 Assignment Massage Therapy Rachel Martinezapi-557736833No ratings yet
- Aproach in Difficult Airway ManagementDocument24 pagesAproach in Difficult Airway Managementarnawa ekaNo ratings yet
- Water Birth PPDocument5 pagesWater Birth PPAzi SamiNo ratings yet
- Rajkumar PDFDocument5 pagesRajkumar PDFAmaradeepika JagannathanNo ratings yet
- Efficacy of A Harvest Graft Substitute For Recession Coverage and Soft Tissue Volume Augmentation. A Randomized Controlled TrialDocument21 pagesEfficacy of A Harvest Graft Substitute For Recession Coverage and Soft Tissue Volume Augmentation. A Randomized Controlled TrialGabriela Lou GomezNo ratings yet
- Full Report-Disinfectant and SanitizerDocument19 pagesFull Report-Disinfectant and Sanitizermohd addinNo ratings yet
- 11 Grammar Test: 94 Photocopiable © Oxford University PressDocument1 page11 Grammar Test: 94 Photocopiable © Oxford University PressLauri RosseNo ratings yet
- Controversies in Condylar Fracture Repair UntalanDocument35 pagesControversies in Condylar Fracture Repair UntalanFrederick Mars Untalan100% (1)
- Living With Diabetes in Uganda Uda 1Document12 pagesLiving With Diabetes in Uganda Uda 1hiNo ratings yet
- 6 Best Homeopathic Medicines For KeloidsDocument3 pages6 Best Homeopathic Medicines For KeloidssuganNo ratings yet
- Catheter Ablation For AFDocument12 pagesCatheter Ablation For AFPeny Ruth Jessica DamanikNo ratings yet
- Anatomi Pembuluh Darah KoronerDocument36 pagesAnatomi Pembuluh Darah KoronerenriNo ratings yet
- NCLEX QuestionsDocument5 pagesNCLEX QuestionsTindo Esa SariNo ratings yet
- Cystitis & UrethritisDocument13 pagesCystitis & UrethritisfemmyNo ratings yet
- ImciDocument3 pagesImciJohn Benzon0% (1)
- Lugols Solution Schillers Test IFU V9 EN4Document1 pageLugols Solution Schillers Test IFU V9 EN4Mary's CatzNo ratings yet
- Chap-2 Notes For Clinical Nutrition and DieteticsDocument5 pagesChap-2 Notes For Clinical Nutrition and Dieteticsstar “Hjaljimmer” platinumNo ratings yet
- Bacterial Skin and Soft Tissue Infections: Clinical Review ArticleDocument9 pagesBacterial Skin and Soft Tissue Infections: Clinical Review ArticleRini MayaSariNo ratings yet
- LAB 4 Simple Stain 2nd 2020-2021Document17 pagesLAB 4 Simple Stain 2nd 2020-2021Deena Hajj QasemNo ratings yet
- Phool Vati BillDocument13 pagesPhool Vati BillVivek PaylaNo ratings yet
- Stomatitis: Overview of The AnatomyDocument6 pagesStomatitis: Overview of The Anatomyjhing_tajulNo ratings yet