You might also like
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pathophysiology-Kni Ns PLZZZDocument8 pagesPathophysiology-Kni Ns PLZZZAnna Lira Manluyang MungcalNo ratings yet
- Lymphangitis LymphadenitisDocument5 pagesLymphangitis LymphadenitisGabriela Cocieru MotelicaNo ratings yet
- LymphadenitisDocument28 pagesLymphadenitisNurul Aini YuditaNo ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- Anatomy and Phsyiology of MeningococcemiaDocument2 pagesAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- Buerger DiseaseDocument3 pagesBuerger DiseaseElmer DizonNo ratings yet
- Hypothyroidism PathophysiologyDocument1 pageHypothyroidism PathophysiologyCleo Joyce C. CristalNo ratings yet
- PATHOPHYSIOLOGYDocument1 pagePATHOPHYSIOLOGYJeroham CoNo ratings yet
- Addison's Disease (Primary Adrenal Insufficiency)Document5 pagesAddison's Disease (Primary Adrenal Insufficiency)sunnnydayNo ratings yet
- Concept MapDocument4 pagesConcept MapChelsyann FerolinoNo ratings yet
- Oral Revalida Round 2Document63 pagesOral Revalida Round 2Mercy Anne EcatNo ratings yet
- Pathophysiology MaiaDocument2 pagesPathophysiology Maiajia88No ratings yet
- Schematic Diagram Pathophysiology (Book-Based) COPD and TuberculosisDocument1 pageSchematic Diagram Pathophysiology (Book-Based) COPD and Tuberculosispragna novaNo ratings yet
- Pneumonia PathoDocument2 pagesPneumonia PathoDerick Nyl PascualNo ratings yet
- Pa Tho Irritable Bowel SyndromeDocument1 pagePa Tho Irritable Bowel Syndromekaye0403No ratings yet
- Acute Rheumatic Fever PathophysiologyDocument1 pageAcute Rheumatic Fever PathophysiologyMoonyeen Jann Casera BalicNo ratings yet
- POTTs Disease PathoDocument3 pagesPOTTs Disease PathoEdgel QuidolesNo ratings yet
- Pa Tho Physiology Part 1Document1 pagePa Tho Physiology Part 1anonymous89ify100% (2)
- Pathophysiology of HyperthyroidismDocument4 pagesPathophysiology of HyperthyroidismKitty YuffieNo ratings yet
- Communicating Pathophysiology: Impaired Absorption of The CSF in The Arachnoid SpaceDocument2 pagesCommunicating Pathophysiology: Impaired Absorption of The CSF in The Arachnoid SpaceAyaBasilioNo ratings yet
- Tension Pneumothorax PDFDocument2 pagesTension Pneumothorax PDFClarissa Aileen Caliva AdoraNo ratings yet
- Patho DengueDocument3 pagesPatho DengueLindy Shane BoncalesNo ratings yet
- Concept MapDocument3 pagesConcept MapKevin T. KatadaNo ratings yet
- CASE PRESentationDocument30 pagesCASE PRESentationllanelli.graciaNo ratings yet
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- Pathophysiology of OsteomyelitisDocument2 pagesPathophysiology of Osteomyelitissorryandreosayanisalreadytaken100% (1)
- Osteosarcoma-Ana and PhysiologyDocument4 pagesOsteosarcoma-Ana and PhysiologyNeirfla WassabiNo ratings yet
- PathophysiologyDocument2 pagesPathophysiologyKarla Karina Dela CruzNo ratings yet
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- 3 NCP AsthmaDocument6 pages3 NCP AsthmajaninenicoleNo ratings yet
- Right-Sided Heart FailureDocument4 pagesRight-Sided Heart FailureKhalid Mahmud ArifinNo ratings yet
- Pathophysiology of Meniere FinalDocument1 pagePathophysiology of Meniere Final1S VILLEGAS GabrielNo ratings yet
- Schistosomiasis Case StudyDocument5 pagesSchistosomiasis Case Studyapi-318749549No ratings yet
- V. Pathophysiology Modifiable Non-ModifiableDocument3 pagesV. Pathophysiology Modifiable Non-ModifiableSteffi MurielNo ratings yet
- LymphadenitisDocument6 pagesLymphadenitisWendy FXNo ratings yet
- Annotated Group 2 Impetigo Concept Mapping 1Document30 pagesAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANONo ratings yet
- Pa Tho Physiology of RaDocument7 pagesPa Tho Physiology of Ralisalmar2008No ratings yet
- BPH Pathophysio 4CDocument2 pagesBPH Pathophysio 4CPatricia Camille Ponce JonghunNo ratings yet
- Pathophysiology - Acute Respiratory Distress Syndrome (ARDS)Document1 pagePathophysiology - Acute Respiratory Distress Syndrome (ARDS)Jewel YapNo ratings yet
- Age - Weather: Aspiration of Secretions Containing MicrobesDocument4 pagesAge - Weather: Aspiration of Secretions Containing Microbeslouie john abilaNo ratings yet
- Pathophysiology of CHFDocument1 pagePathophysiology of CHFLance MarquezNo ratings yet
- Preeclampsia Pathophysiology and ManagementDocument7 pagesPreeclampsia Pathophysiology and ManagementAuliaNo ratings yet
- Hypertensive Crisis - PathophysiologyDocument1 pageHypertensive Crisis - Pathophysiologyaaron tabernaNo ratings yet
- Case Presentation (Final)Document35 pagesCase Presentation (Final)Denie BoyonasNo ratings yet
- Sandeep Sharma Deepa Rawat Sandeep Sharma, Deep RawatDocument29 pagesSandeep Sharma Deepa Rawat Sandeep Sharma, Deep RawatAngelica PingulNo ratings yet
- Discharge PlanDocument5 pagesDischarge PlanrraksNo ratings yet
- PATHOPHYDocument3 pagesPATHOPHYArlly Faena AbadNo ratings yet
- Influenza PATHOPHYSIOLOGYDocument3 pagesInfluenza PATHOPHYSIOLOGYElle RosalesNo ratings yet
- CroupDocument20 pagesCroupFariezuan HamidNo ratings yet
- CARBUNCLEDocument11 pagesCARBUNCLEKesavanadh T M100% (1)
- Hypovolemic Shock 05Document50 pagesHypovolemic Shock 05Chary JaztineNo ratings yet
- (Patho) PTB COPDDocument1 page(Patho) PTB COPDKyle HannahNo ratings yet
- B. Diagram: Predisposing Factors: Precipitating Factors EtiologyDocument3 pagesB. Diagram: Predisposing Factors: Precipitating Factors EtiologyKenneth Torres100% (1)
- Book Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsDocument7 pagesBook Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsIrish EspinosaNo ratings yet
- Mycobacterium Tuberculosis: Precipitating Factors: Predisposing FactorsDocument1 pageMycobacterium Tuberculosis: Precipitating Factors: Predisposing FactorsYoko Mae Yano100% (1)
- Pathophysiology of TuberculosisDocument3 pagesPathophysiology of TuberculosisMonica Marie Morales86% (14)
- Path o Physio TB EffusionDocument2 pagesPath o Physio TB EffusionSergi Lee OrateNo ratings yet
- PathophysiologyDocument6 pagesPathophysiologyElbert Hermogino ﭢNo ratings yet
- Pathophysiology of TBDocument3 pagesPathophysiology of TBEddie Lou GuzmanNo ratings yet
- Math Edge Oct13Document5 pagesMath Edge Oct13Paulo ParenasNo ratings yet
- MATH Module 1Document3 pagesMATH Module 1Paulo ParenasNo ratings yet
- Geas Module NotesDocument3 pagesGeas Module Notesemely p. tangoNo ratings yet
- 3.1 Understanding Formative AssessmentDocument5 pages3.1 Understanding Formative Assessmentemely p. tangoNo ratings yet
- 3.2 Differentiating Formative and Summative AssessmentsDocument6 pages3.2 Differentiating Formative and Summative Assessmentsemely p. tangoNo ratings yet
- 3.3 Applying Different Formative Assessment TasksDocument8 pages3.3 Applying Different Formative Assessment Tasksemely p. tangoNo ratings yet
- Training Design - PRIMALS 4-6 (Math)Document1 pageTraining Design - PRIMALS 4-6 (Math)emely p. tangoNo ratings yet
- Training Design - PRIMALS 4-6 (Science)Document1 pageTraining Design - PRIMALS 4-6 (Science)emely p. tangoNo ratings yet
- Deficiency of Iron: First Semester A.Y. 2015-2016Document8 pagesDeficiency of Iron: First Semester A.Y. 2015-2016emely p. tangoNo ratings yet
- 3.0 Identifying Learning Progression and Learning TargetsDocument8 pages3.0 Identifying Learning Progression and Learning TargetsNelia Grafe75% (4)
- Training Design - PRIMALS 4-6 (Science)Document1 pageTraining Design - PRIMALS 4-6 (Science)emely p. tangoNo ratings yet
- Training Design - PRIMALS 4-6 (Science)Document1 pageTraining Design - PRIMALS 4-6 (Science)emely p. tangoNo ratings yet
- Training Design - PRIMALS 4-6 (Science)Document1 pageTraining Design - PRIMALS 4-6 (Science)emely p. tangoNo ratings yet
- Patho Supplement Handout For Sept 2018 UPDATED May 2018Document27 pagesPatho Supplement Handout For Sept 2018 UPDATED May 2018emely p. tangoNo ratings yet
- ChorioamnionitisDocument1 pageChorioamnionitisemely p. tangoNo ratings yet
- CPG On Dengue in Children 2017Document108 pagesCPG On Dengue in Children 2017Hannah LeiNo ratings yet
- Patho Supplement Handout For Sept 2018 UPDATED May 2018 PDFDocument25 pagesPatho Supplement Handout For Sept 2018 UPDATED May 2018 PDFemely p. tango100% (1)
- 4.2 Drugs Used in Coagulation DisordersDocument10 pages4.2 Drugs Used in Coagulation Disordersemely p. tangoNo ratings yet
- 11 - SurgpathDocument22 pages11 - Surgpathemely p. tangoNo ratings yet
- Pedia Case 3Document18 pagesPedia Case 3emely p. tangoNo ratings yet
- TB Journal PDFDocument108 pagesTB Journal PDFemely p. tangoNo ratings yet
- ChorioamnionitisDocument1 pageChorioamnionitisemely p. tangoNo ratings yet
- Informant: Grandmother (70 %) Reliability General DataDocument8 pagesInformant: Grandmother (70 %) Reliability General Dataemely p. tangoNo ratings yet
- Respiratory MCQDocument10 pagesRespiratory MCQSyeda Aroosa Abbas Naqvi100% (1)
- (See Next Diagram) : Autonomic Nervous System Rashelle Lopez-Salvatierra, MD Somatic DivisionDocument7 pages(See Next Diagram) : Autonomic Nervous System Rashelle Lopez-Salvatierra, MD Somatic Divisionemely p. tango100% (4)
- Vocabulary Exercises: 1) Complete in The Correct WayDocument5 pagesVocabulary Exercises: 1) Complete in The Correct Waylaura1pinilla1domingNo ratings yet
- Chest RadiographyDocument65 pagesChest RadiographyMunish Dogra100% (1)
- HSC 430 Lesson PlanDocument13 pagesHSC 430 Lesson Planapi-486607583No ratings yet
- 144 Diagnosa FKTPDocument5 pages144 Diagnosa FKTPpuskesmas100% (1)
- A To Z Orthodontics Vol 3 Malocclusion1Document36 pagesA To Z Orthodontics Vol 3 Malocclusion1Ishtiaq HasanNo ratings yet
- Petri DishDocument7 pagesPetri DishMizzannul HalimNo ratings yet
- Vaccines CHNDocument2 pagesVaccines CHNLyra LorcaNo ratings yet
- CiprofloxacinDocument2 pagesCiprofloxacinNika Joy Cabrera AlarconNo ratings yet
- RH D Immunoglobulin (Anti-D)Document4 pagesRH D Immunoglobulin (Anti-D)Ywagar YwagarNo ratings yet
- (Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringDocument8 pages(Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringKim RamosNo ratings yet
- CBSE Class 7 English - Comprehension PassageDocument7 pagesCBSE Class 7 English - Comprehension PassagemotherhoodNo ratings yet
- Prepartion of Blood Smear Hematology PresentationDocument44 pagesPrepartion of Blood Smear Hematology PresentationArslan ArshadNo ratings yet
- Development of The Fetal Membranes and PlacentaDocument4 pagesDevelopment of The Fetal Membranes and PlacentaBandula KusumsiriNo ratings yet
- Global Zoonoses: Merck Manual Veterinary ManualDocument86 pagesGlobal Zoonoses: Merck Manual Veterinary ManualPaula PollNo ratings yet
- ENGLISH GRAMMER For STD 6Document21 pagesENGLISH GRAMMER For STD 6Joy OtanielNo ratings yet
- Blood DopingDocument16 pagesBlood Dopingpriyanka lalwaniNo ratings yet
- Refinements in The Care and Use of Animals in Toxicology Studies - Regulation, Validation and ProgressDocument8 pagesRefinements in The Care and Use of Animals in Toxicology Studies - Regulation, Validation and Progressgabriela_mariangela5929No ratings yet
- Cusack Protocol .. Supplement Dosages Information Chart. Word PDFDocument2 pagesCusack Protocol .. Supplement Dosages Information Chart. Word PDFNaomy DC100% (6)
- Articulo 3Document5 pagesArticulo 3Valeria Rodriguez GomezNo ratings yet
- The Vodka Diet Edit 12.20Document114 pagesThe Vodka Diet Edit 12.20Late Knight GamingNo ratings yet
- TonsillitisDocument3 pagesTonsillitisVina MuspitaNo ratings yet
- Nutrition: Important ConceptsDocument12 pagesNutrition: Important ConceptshafizaqaiNo ratings yet
- Poodle Papers Winter 2007Document36 pagesPoodle Papers Winter 2007PCA_website100% (8)
- Nur112: Anatomy and Physiology ISU Echague - College of NursingDocument14 pagesNur112: Anatomy and Physiology ISU Echague - College of NursingWai KikiNo ratings yet
- Respiratory Distress SyndromeDocument4 pagesRespiratory Distress SyndromeRommar RomeroNo ratings yet
- 5937 Understanding Nonverbal Communication Guidebook PDFDocument116 pages5937 Understanding Nonverbal Communication Guidebook PDFSalomao RodriguesNo ratings yet
- Samphire2003 PDFDocument9 pagesSamphire2003 PDFYacine Tarik AizelNo ratings yet
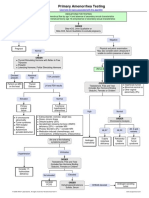
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmGabriella AguirreNo ratings yet
- 11 16Document128 pages11 16WoodsNo ratings yet
- Platelet CountsDocument35 pagesPlatelet Countsshikhar623No ratings yet