You might also like
- DAAD - Health CertificateDocument2 pagesDAAD - Health Certificaterosenrot1100% (2)
- Fulbright Certificate of HealthDocument8 pagesFulbright Certificate of HealthLinda Klimavicius100% (1)
- Clinical Pathology: Test Name Result Unit Biological Reference Interval Urine R & MDocument5 pagesClinical Pathology: Test Name Result Unit Biological Reference Interval Urine R & MAbhishek ChaudharyNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- BKI KUL: Ibrahim / Mokhtar Bin MRDocument1 pageBKI KUL: Ibrahim / Mokhtar Bin MRkv likasNo ratings yet
- Four Seasons Hotel Vancouver Reservation - Booking PDFDocument1 pageFour Seasons Hotel Vancouver Reservation - Booking PDFHakan DemirciNo ratings yet
- Lab Report NewDocument3 pagesLab Report Newhacebe2685No ratings yet
- COVID 19 Positive Test Report Form: 24 HoursDocument2 pagesCOVID 19 Positive Test Report Form: 24 HoursRaju SambheNo ratings yet
- Decleration LetterDocument1 pageDecleration LetterRT WorkNo ratings yet
- RT PCR Test ReportDocument2 pagesRT PCR Test ReportMoumita MandalNo ratings yet
- Department of Molecular Biology. Covid 19 RTPCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Molecular Biology. Covid 19 RTPCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodAryan RathoreNo ratings yet
- Diagnostic Report: Patient Name: Gopal Mondal GOPAM301119980 0002UF026577Document2 pagesDiagnostic Report: Patient Name: Gopal Mondal GOPAM301119980 0002UF026577world one AR BABUNo ratings yet
- Molecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassDocument4 pagesMolecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassmeezNo ratings yet
- O Redmi Note 8 Co Al Quad Camera: Test Report Status Final Results Biological Reference Interval UnitsDocument1 pageO Redmi Note 8 Co Al Quad Camera: Test Report Status Final Results Biological Reference Interval Unitsyash yadavNo ratings yet
- E Ticket ReceiptDocument4 pagesE Ticket ReceiptChitrakNo ratings yet
- All India Institute of Medical Sciences (Aiims) : Laboratory Observation ReportDocument2 pagesAll India Institute of Medical Sciences (Aiims) : Laboratory Observation ReportPiyush TripathiNo ratings yet
- Sars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRDocument3 pagesSars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRAmbareen AbidNo ratings yet
- Research PaperDocument2 pagesResearch PaperSUHAIL BABANo ratings yet
- TUV Rheinland of North America, Inc.: 12 Commerce Road, Newton, CT 06470, USADocument1 pageTUV Rheinland of North America, Inc.: 12 Commerce Road, Newton, CT 06470, USAahmadNo ratings yet
- Department of Molecular Biology. Covid 19 RTPCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodDocument3 pagesDepartment of Molecular Biology. Covid 19 RTPCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodPraveen KumarNo ratings yet
- Https Covid19.aarogyasri - Telangana.gov - in COVID Covidaction - Do Actionflag generateLabReportOTP&entryId COV4184742 PDFDocument2 pagesHttps Covid19.aarogyasri - Telangana.gov - in COVID Covidaction - Do Actionflag generateLabReportOTP&entryId COV4184742 PDFJayanth GowdaNo ratings yet
- Lab ResultDocument1 pageLab ResultShubhNo ratings yet
- ConsolidatedDocument1 pageConsolidatedLatif KhanNo ratings yet
- Form No. 10iDocument2 pagesForm No. 10idinesh makwanaNo ratings yet
- Muhammad AsgharDocument1 pageMuhammad AsgharayazNo ratings yet
- Arms 0Document2 pagesArms 0Jewel Mae DanielNo ratings yet
- Compulsory Health Certificate (Form B)Document1 pageCompulsory Health Certificate (Form B)Gmv VijuNo ratings yet
- MR Ravi Kiran Maddali: TEG83R Confirmed CompleteDocument3 pagesMR Ravi Kiran Maddali: TEG83R Confirmed CompletemasterrkNo ratings yet
- Certificate Equalancy Department.Document17 pagesCertificate Equalancy Department.Um Roumman0% (1)
- Vaccination Certificate PDFDocument1 pageVaccination Certificate PDFVivek SinghNo ratings yet
- Lab No. Age/Gender Coll. On Name Reg. On Ref. Dr. Approved On 16/aug/2021 03:05PM Rpt. Centre Printed OnDocument1 pageLab No. Age/Gender Coll. On Name Reg. On Ref. Dr. Approved On 16/aug/2021 03:05PM Rpt. Centre Printed OnPratik GargNo ratings yet
- RDS - TTR 1887Document1 pageRDS - TTR 1887emc roorkee59No ratings yet
- 1.0 Customer's Details: Calibration Certificate NDocument2 pages1.0 Customer's Details: Calibration Certificate NCyriaque KagororaNo ratings yet
- Form E2Document4 pagesForm E2Charles DanieNo ratings yet
- T2100001419 ML2100001252 115620 6691600 19370729 $mole-DefauDocument2 pagesT2100001419 ML2100001252 115620 6691600 19370729 $mole-DefauPeony03No ratings yet
- Part One: Applicant Details (To Be Completed by Applicant)Document4 pagesPart One: Applicant Details (To Be Completed by Applicant)MahmudNo ratings yet
- Appointment RecieptDocument3 pagesAppointment Recieptsiva5256No ratings yet
- Man Ishta MtaDocument2 pagesMan Ishta MtaDhairya TamtaNo ratings yet
- E-Ticket Passenger and 1 MoreDocument7 pagesE-Ticket Passenger and 1 MoreArmaNo ratings yet
- Air India - Fulfilment AIBE37491169 JMG3SDocument2 pagesAir India - Fulfilment AIBE37491169 JMG3SAnandNo ratings yet
- Case 2Document12 pagesCase 2bekbekk cabahugNo ratings yet
- JJJHJHDocument1 pageJJJHJHDrAbhishek SarafNo ratings yet
- Ticket From Jessore To DhakaDocument3 pagesTicket From Jessore To DhakaSugrib K ShahaNo ratings yet
- Personal Accident: Claim FormDocument3 pagesPersonal Accident: Claim FormAmr TarekNo ratings yet
- Medical CertificateDocument1 pageMedical Certificate2101641530003100% (1)
- 44 Ansari Mohammad IrfanDocument2 pages44 Ansari Mohammad IrfanAlaa HusseinNo ratings yet
- Fare Details:: Log in Print Ticket Cancel TicketDocument4 pagesFare Details:: Log in Print Ticket Cancel TicketShanky ChakrabortyNo ratings yet
- Physical Examination Report: 23/FEMALE Dalig, Balayan, Batangas 7/11/1997 8:50 AM Waltermart Balayan 6/4/2021 SingleDocument3 pagesPhysical Examination Report: 23/FEMALE Dalig, Balayan, Batangas 7/11/1997 8:50 AM Waltermart Balayan 6/4/2021 SingleIan De LeonNo ratings yet
- AdmitDocument1 pageAdmitDrisha PaulNo ratings yet
- Health Questionnaire For Online Version - Retail Revised VersionDocument4 pagesHealth Questionnaire For Online Version - Retail Revised VersionTrushaba B. JadejaNo ratings yet
- FormatDocument3 pagesFormatchiragNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsMaria JessaNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsJaj EscNo ratings yet
- Medical Declaration Form: Family History of The ApplicantDocument3 pagesMedical Declaration Form: Family History of The ApplicantJae WaiNo ratings yet
- GHS Health Declaration Form PDFDocument2 pagesGHS Health Declaration Form PDFFattah AfawNo ratings yet
- 3 Health PDFDocument2 pages3 Health PDFAndré DomanskiNo ratings yet
- Latihan MTK Un SMP BahasDocument2 pagesLatihan MTK Un SMP Bahasdinas pertanianNo ratings yet
- 3 Health PDFDocument2 pages3 Health PDFpierlisurNo ratings yet
- Prulife Uk Form PiDocument3 pagesPrulife Uk Form PiPaulie TitoNo ratings yet
- Application CoopMED Health Insurance Plan BarbadosDocument2 pagesApplication CoopMED Health Insurance Plan BarbadosKammieNo ratings yet
- SB 10054865 6305Document15 pagesSB 10054865 6305Ralph WamaeNo ratings yet
- 18-00027-16 2018 - NCA - EPRP - Final - Evaluation - AAH - No - Annex 593197 - 1 - 1Document84 pages18-00027-16 2018 - NCA - EPRP - Final - Evaluation - AAH - No - Annex 593197 - 1 - 1Ralph WamaeNo ratings yet
- TSB For The Ob5 With Software Update OptionDocument13 pagesTSB For The Ob5 With Software Update OptionRalph WamaeNo ratings yet
- 001002-2011732-8 00 Software Version Management (SVM), Operating InstructionsDocument8 pages001002-2011732-8 00 Software Version Management (SVM), Operating InstructionsRalph WamaeNo ratings yet
- Policy On Emergency Preparedness and Response: Key PointsDocument10 pagesPolicy On Emergency Preparedness and Response: Key PointsRalph WamaeNo ratings yet
- Abrites J2534 Passthru Driver User ManualDocument37 pagesAbrites J2534 Passthru Driver User ManualRalph WamaeNo ratings yet
- Vvdi2 OverviewDocument30 pagesVvdi2 OverviewRalph Wamae100% (1)
- DSG Clutch Removal Tool Set Eng PrinterDocument15 pagesDSG Clutch Removal Tool Set Eng PrinterRalph Wamae100% (1)
- South Sudan Field Presence Map Feb May2016bDocument4 pagesSouth Sudan Field Presence Map Feb May2016bRalph WamaeNo ratings yet
- Mag Pro2 V4.2 Installation ManualDocument10 pagesMag Pro2 V4.2 Installation ManualRalph WamaeNo ratings yet
- Airwerks IntroDocument32 pagesAirwerks IntroRalph WamaeNo ratings yet
- Si Luk 0041 Malfunctions On The Direct Shift Transmission de en PreviewDocument1 pageSi Luk 0041 Malfunctions On The Direct Shift Transmission de en PreviewRalph WamaeNo ratings yet
- Rodcraft Workshop2012Document28 pagesRodcraft Workshop2012Ralph WamaeNo ratings yet
- Operational HandbookDocument51 pagesOperational HandbookRalph WamaeNo ratings yet
- CDC - Fasciola - BiologyDocument2 pagesCDC - Fasciola - BiologypecopecochanNo ratings yet
- Uterus Body Pathology: Dr. Mona RashedDocument29 pagesUterus Body Pathology: Dr. Mona RashedSavin PetersNo ratings yet
- Handbook Pikeperch ReproductionDocument80 pagesHandbook Pikeperch ReproductioniddiottNo ratings yet
- Surrogacy Affirmative 1st CsDocument3 pagesSurrogacy Affirmative 1st CsMay-may TambaoanNo ratings yet
- Stem CellDocument63 pagesStem CellashubhalaaNo ratings yet
- Unit 1. PlantsDocument31 pagesUnit 1. PlantsMiriam GonzálezNo ratings yet
- Artículo Estudio Ramachandran AGI Personas Bigénero PDFDocument6 pagesArtículo Estudio Ramachandran AGI Personas Bigénero PDFMikaNo ratings yet
- Cytogenetic Analysis of Male InfertilityDocument7 pagesCytogenetic Analysis of Male InfertilityIOSRjournal100% (1)
- SituationdDocument64 pagesSituationdIvory SantiagoNo ratings yet
- Quantitative Morphological Changes in The Interplacentomal Wall of The Gravid Uterine Horn of Cattle During PregnancyDocument8 pagesQuantitative Morphological Changes in The Interplacentomal Wall of The Gravid Uterine Horn of Cattle During PregnancyfeyisaNo ratings yet
- Human Embryology, Research and EthicsDocument42 pagesHuman Embryology, Research and EthicsnorjannahhassanNo ratings yet
- Occult Forces of SexDocument6 pagesOccult Forces of Seximmortality2045_841960% (5)
- MCN QuizDocument6 pagesMCN QuizMÖna Macaranas100% (5)
- A Clinical Study On Oligohydramnios in The ThirdDocument23 pagesA Clinical Study On Oligohydramnios in The ThirdDickyNo ratings yet
- vARICOCELE3 PDFDocument3 pagesvARICOCELE3 PDFSylvia AnggraeniNo ratings yet
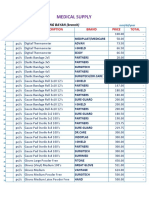
- Medical Supplies, & Baby Products PricelistDocument5 pagesMedical Supplies, & Baby Products PricelistParmasya Ng Bayan Bacolor Main BranchNo ratings yet
- James W.D., Elston D.M., 2011. Andrews' Diseases of The Skin: Clinical Dermatology. 11th Ed. Saunders/Elsevier London, UK: P. 126Document4 pagesJames W.D., Elston D.M., 2011. Andrews' Diseases of The Skin: Clinical Dermatology. 11th Ed. Saunders/Elsevier London, UK: P. 126FranditaNo ratings yet
- Zoology II PDFDocument6 pagesZoology II PDFKasuriZaffarNo ratings yet
- Physiology of ReproductionDocument34 pagesPhysiology of ReproductionCalcium QuèNo ratings yet
- Dominance RelationshipsDocument30 pagesDominance RelationshipsGretz AnticamaraNo ratings yet
- CultureCoin Preparation Procedure For Miri Time-Lapse IncubatorDocument2 pagesCultureCoin Preparation Procedure For Miri Time-Lapse IncubatorernestoveigaNo ratings yet
- Does DHT Affect Transplanted HairDocument2 pagesDoes DHT Affect Transplanted HairsahakhanshahNo ratings yet
- Obtaining Valid Consent: Clinical Governance Advice No. 6Document9 pagesObtaining Valid Consent: Clinical Governance Advice No. 6Ywagar YwagarNo ratings yet
- Parasites of Medical ImportanceDocument156 pagesParasites of Medical ImportanceFlavius BeleanNo ratings yet
- 2022 P2 CV Form 3 San AntonioDocument13 pages2022 P2 CV Form 3 San AntonioShai SdmpNo ratings yet
- Fetal Colonic GradeDocument7 pagesFetal Colonic Gradedgina8800No ratings yet
- Responsible ParenthoodDocument21 pagesResponsible ParenthoodFrances Quibuyen DatuinNo ratings yet
- Abnormal-Uterine-Bleeding Case StudyDocument57 pagesAbnormal-Uterine-Bleeding Case StudyOneForAll :100% (1)
- 12 Biology - Reproductive HealthDocument4 pages12 Biology - Reproductive HealthTanya Mishra100% (1)
- Advantages of ContraceptivesDocument4 pagesAdvantages of ContraceptivesArgel Linard Francisco MabagaNo ratings yet