You might also like
- FNP: Skin ReviewDocument11 pagesFNP: Skin ReviewOMGStudy100% (2)
- SketchyPharm Antineoplastics FINALDocument19 pagesSketchyPharm Antineoplastics FINALKlNo ratings yet
- Head To Toe Assessment Checklist Older Adults-1Document1 pageHead To Toe Assessment Checklist Older Adults-1spatrick32100% (4)
- THyroid DisorderDocument39 pagesTHyroid DisorderT.A.BNo ratings yet
- Lista OndamedDocument2 pagesLista Ondamedmona miaNo ratings yet
- Management of Benign Breast Conditions: Part 2 - Breast Lumps and LesionsDocument3 pagesManagement of Benign Breast Conditions: Part 2 - Breast Lumps and Lesionspeter_mrNo ratings yet
- Radical Orchiectomy DURDocument17 pagesRadical Orchiectomy DURyulian salis patriawanNo ratings yet
- COPD (Chronic Obstructive Pulmonary Disease)Document8 pagesCOPD (Chronic Obstructive Pulmonary Disease)Emily Anne86% (7)
- 40 Phimosis 1Document8 pages40 Phimosis 1Navis Naldo AndreanNo ratings yet
- Konsensus FIGO 2016Document106 pagesKonsensus FIGO 2016Anonymous Tzn8RGBZ4100% (1)
- Cesarean Scar Pregnancies and Their ManagementDocument7 pagesCesarean Scar Pregnancies and Their ManagementClinton SitanggangNo ratings yet
- Surgical Atlas Transureteroureterostomy: John M. BarryDocument7 pagesSurgical Atlas Transureteroureterostomy: John M. BarrycristiangelsNo ratings yet
- Drug Study - Vitamin B ComplexDocument1 pageDrug Study - Vitamin B ComplexmikErlh0% (1)
- Pathophysiology of CryptorchidismDocument5 pagesPathophysiology of CryptorchidismAlaiza Aberasturi50% (2)
- Laparoscopy: Shenillee Burgess Reyad HoseinDocument31 pagesLaparoscopy: Shenillee Burgess Reyad HoseinShenillee BurgessNo ratings yet
- The Management of Asherman Syndrome: A Review of LiteratureDocument11 pagesThe Management of Asherman Syndrome: A Review of LiteratureEuphra Adellheid100% (1)
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 pagesLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghNo ratings yet
- Hypospadias Surgery An Illustrated GuideDocument20 pagesHypospadias Surgery An Illustrated GuideyumnamuzakkirNo ratings yet
- Female Genital Tuberculosis HysterosalpingographicDocument7 pagesFemale Genital Tuberculosis HysterosalpingographicDyan Riza Indah TamiNo ratings yet
- Cancer Program SeminarDocument98 pagesCancer Program SeminarhemihemaNo ratings yet
- Imaging Features: Cleidocranial DysplasiaDocument13 pagesImaging Features: Cleidocranial DysplasiaLevina DermawanNo ratings yet
- HemorrhoidsDocument20 pagesHemorrhoidsEdwin PratamaNo ratings yet
- Endoscopic SurgeryDocument152 pagesEndoscopic SurgeryiciNo ratings yet
- Birth Defects - PPSXDocument47 pagesBirth Defects - PPSXCharith R Ramesh100% (1)
- Urological EmergencyDocument83 pagesUrological EmergencyIrwan SaputraNo ratings yet
- Ananth Narayan and Paniker 11th EditionDocument42 pagesAnanth Narayan and Paniker 11th EditionArjun Kandara50% (2)
- Buried PenisDocument3 pagesBuried Penischoirin nurNo ratings yet
- Urodynamics: Committee 7Document56 pagesUrodynamics: Committee 7Coral Garcia RiveraNo ratings yet
- Concealed Penis PDFDocument5 pagesConcealed Penis PDFZlatan ZvizdicNo ratings yet
- Retractile Testis PDFDocument6 pagesRetractile Testis PDFDella Elvina RoeslandNo ratings yet
- Dermatofitosis: Ema Surya Pertiwi (1102005108) Putu Mita Wulandari (1102005130)Document49 pagesDermatofitosis: Ema Surya Pertiwi (1102005108) Putu Mita Wulandari (1102005130)Cox AbeeNo ratings yet
- Hipo HiperthyroidDocument49 pagesHipo HiperthyroidMuhammad Bilal Bin AmirNo ratings yet
- Rcog 2016 Emarazo EctopicoDocument41 pagesRcog 2016 Emarazo EctopicoJose Luis Morales BautistaNo ratings yet
- EXTERNAL CEPHALIC VERSION AND REDUCING THE INCIDENCE OF Breech PDFDocument8 pagesEXTERNAL CEPHALIC VERSION AND REDUCING THE INCIDENCE OF Breech PDFrolla_hiraNo ratings yet
- Paper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionDocument14 pagesPaper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionAimanNo ratings yet
- Absorbable Suture IndicationDocument57 pagesAbsorbable Suture IndicationSariSyamerNo ratings yet
- 2017 Bone Modifying Agents in Met BC Slides - PpsDocument14 pages2017 Bone Modifying Agents in Met BC Slides - Ppsthanh tinh BuiNo ratings yet
- Table 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationDocument111 pagesTable 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationArya Syafaromania RachmaNo ratings yet
- Non Hodgkin's Lymphoma: Rakesh BiswasDocument16 pagesNon Hodgkin's Lymphoma: Rakesh BiswasDayledaniel SorvetoNo ratings yet
- Double Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF:ICSI Programmes (Shanghai Protocol) - ScienceDirectDocument3 pagesDouble Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF:ICSI Programmes (Shanghai Protocol) - ScienceDirectsamirNo ratings yet
- Omphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Document17 pagesOmphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Rully Riyan DikaNo ratings yet
- Handrub Vs HandscrubDocument7 pagesHandrub Vs HandscrubElisya KharuniawatiNo ratings yet
- Diaphragma InjuryDocument18 pagesDiaphragma InjuryAhmedNo ratings yet
- Digital Atlas of Cystoscopy: Jan SchönebeckDocument48 pagesDigital Atlas of Cystoscopy: Jan SchönebeckdemisNo ratings yet
- Pregnancy Related Skin Changes and Skin DiseaseDocument22 pagesPregnancy Related Skin Changes and Skin DiseaseNellaNo ratings yet
- Cryptorchidism: The Absence of One or Both Testes From The ScrotumDocument7 pagesCryptorchidism: The Absence of One or Both Testes From The ScrotumClaudetteanne6171No ratings yet
- Snake Bite National Protocol PediatricsDocument45 pagesSnake Bite National Protocol Pediatricsarjun_paulNo ratings yet
- Physical and Sexual Abuse (Kuliah Power Point Blok 2)Document39 pagesPhysical and Sexual Abuse (Kuliah Power Point Blok 2)Saputra Tri Nopianto100% (1)
- Sign of Hyperandrogenism PDFDocument6 pagesSign of Hyperandrogenism PDFmisbah_mdNo ratings yet
- Pathologic and Physiologic PhimosisDocument7 pagesPathologic and Physiologic Phimosisdianita507No ratings yet
- Phimosis 5 PDFDocument4 pagesPhimosis 5 PDFNurul YaqinNo ratings yet
- Pediatrics in Review 2006 Sugar 213 23Document13 pagesPediatrics in Review 2006 Sugar 213 23Berry BancinNo ratings yet
- Pathologic and Physiologic PhimosisDocument4 pagesPathologic and Physiologic PhimosisJuwita PratiwiNo ratings yet
- Paediatric Urology - Peno-Scrotal: Case 1 Case 2Document2 pagesPaediatric Urology - Peno-Scrotal: Case 1 Case 2HardiTariqHammaNo ratings yet
- 201111asmith PDFDocument3 pages201111asmith PDFkamil abdulieNo ratings yet
- Human Chromosomal AbnormalitiesDocument3 pagesHuman Chromosomal Abnormalitiescindy0% (1)
- Isrn Urology2012-707329 PDFDocument6 pagesIsrn Urology2012-707329 PDFNaomiRimaClaudyaNo ratings yet
- Review Article: Phimosis in ChildrenDocument7 pagesReview Article: Phimosis in ChildrenmerlinNo ratings yet
- Study of Congenital Malformations in Central Nervous System & Gastro-Intestinal TractDocument3 pagesStudy of Congenital Malformations in Central Nervous System & Gastro-Intestinal TractDayuKurnia DewantiNo ratings yet
- Phimosis and Paraphimosis: February 2017Document8 pagesPhimosis and Paraphimosis: February 2017Rollin SidaurukNo ratings yet
- Paediatric Vaginal DischargeDocument3 pagesPaediatric Vaginal DischargeTanwi SinghNo ratings yet
- Microglossia in A Newborn: A Case Report and Review of The LiteratureDocument1 pageMicroglossia in A Newborn: A Case Report and Review of The LiteratureSela PutrianaNo ratings yet
- Proper Care of The Intact PenisDocument13 pagesProper Care of The Intact PenisJL VMNo ratings yet
- Benign Penile Skin Anomalies in Children: A Primer For PediatriciansDocument8 pagesBenign Penile Skin Anomalies in Children: A Primer For Pediatriciansdrfebri86No ratings yet
- Amniotic Band Sequence: Consult SeriesDocument2 pagesAmniotic Band Sequence: Consult SeriesRamos Zavala Julio CesarNo ratings yet
- 781 2987 1 PBDocument3 pages781 2987 1 PBniroshniroshNo ratings yet
- Admin,+27 Ism.v11i1.633Document5 pagesAdmin,+27 Ism.v11i1.633Fasih Djam'an DikaNo ratings yet
- Anomalies of The Penies ...Document6 pagesAnomalies of The Penies ...Firas Abu-SamraNo ratings yet
- Surat Edaran Antisipasi Corona PDFDocument2 pagesSurat Edaran Antisipasi Corona PDFAbdul MalikNo ratings yet
- The Title Must Be Brief, Concise, Informative, and Not Exceed 10 Words (Style: Title) - 16pt, BoldDocument8 pagesThe Title Must Be Brief, Concise, Informative, and Not Exceed 10 Words (Style: Title) - 16pt, BoldAbdul MalikNo ratings yet
- Curriculum Vitae (CV) Abdul Malik SetiawanDocument4 pagesCurriculum Vitae (CV) Abdul Malik SetiawanAbdul MalikNo ratings yet
- Phimosis in A 10-Yr-Old Boy Without Urinary Infection-How To Inform Parents: For CircumcisionDocument2 pagesPhimosis in A 10-Yr-Old Boy Without Urinary Infection-How To Inform Parents: For CircumcisionAbdul MalikNo ratings yet
- Heat-Related Emergencies: BradyDocument33 pagesHeat-Related Emergencies: BradyAbdul MalikNo ratings yet
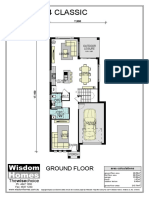
- Modena 24 Classic: Ground FloorDocument2 pagesModena 24 Classic: Ground FloorAbdul MalikNo ratings yet
- EBUS Kazuhiro YasufukuDocument27 pagesEBUS Kazuhiro YasufukuOrion JohnNo ratings yet
- Emergence of Multidrug Resistant Acinetobacter Baumannii As Nosocomial Pathogen: Clinical Significance and Antimicrobial SensitivityDocument5 pagesEmergence of Multidrug Resistant Acinetobacter Baumannii As Nosocomial Pathogen: Clinical Significance and Antimicrobial SensitivityIOSRjournalNo ratings yet
- Annex 8. Viral Transport Media (VTM)Document2 pagesAnnex 8. Viral Transport Media (VTM)deancoksNo ratings yet
- Galvano Terapy Topic - 2Document3 pagesGalvano Terapy Topic - 2Gigi CotoraNo ratings yet
- Antenatal Care Draft Assessment Tool2Document14 pagesAntenatal Care Draft Assessment Tool2Vin BitzNo ratings yet
- Svvfuip Brochure VersionDocument16 pagesSvvfuip Brochure VersionViswasukthamNo ratings yet
- Ake Quick Action If Someone Is Choking On A Swallowed ObjectDocument29 pagesAke Quick Action If Someone Is Choking On A Swallowed ObjectYAMINIPRIYANNo ratings yet
- Question: 1 of 100 / Overall Score: 80%: True / FalseDocument84 pagesQuestion: 1 of 100 / Overall Score: 80%: True / FalseGalaleldin AliNo ratings yet
- Cardiolab Practical-PharmacologyDocument2 pagesCardiolab Practical-PharmacologyGul HassanNo ratings yet
- Data For EMRDocument13 pagesData For EMRggggangNo ratings yet
- Case PresentationDocument53 pagesCase PresentationKristine Dela Cruz100% (2)
- Pre Op GuidelinesDocument11 pagesPre Op GuidelinesHanif FebrianNo ratings yet
- Exercise PrescriptionDocument53 pagesExercise PrescriptionEvangeline A. Alegre100% (1)
- Catheter Ablationin in AF With CHFDocument11 pagesCatheter Ablationin in AF With CHFKristian Sudana HartantoNo ratings yet
- Ioftn IndexDocument7 pagesIoftn IndexDelta JackNo ratings yet
- AbbreviationsDocument37 pagesAbbreviationsElie RizkNo ratings yet
- Schallware (Watermark)Document9 pagesSchallware (Watermark)mat koolNo ratings yet
- 0812 Gelofusine PDFDocument2 pages0812 Gelofusine PDFMsglow WulanNo ratings yet
- Opioid-Free AnesthesiaDocument8 pagesOpioid-Free AnesthesiaPaulina LugoNo ratings yet
- Bài Tập Tự Luyện Unit 2: Your Body And You (Lesson 1) #hasuenglishclassDocument4 pagesBài Tập Tự Luyện Unit 2: Your Body And You (Lesson 1) #hasuenglishclassThu Tra NguyenNo ratings yet
- Lab Policies Alkaline Phosphatase C311 Lab 8803Document4 pagesLab Policies Alkaline Phosphatase C311 Lab 8803Valdez Francis ZaccheauNo ratings yet
- Thesis Related To Breast Self ExaminationDocument6 pagesThesis Related To Breast Self Examinationfjfyj90y100% (3)